Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Case Report - (2014) Volume 2, Issue 2
The authors present the case of a 27 yr old female who failed conservative management for a tibial stress fracture. The patient was known to suffer from “Female Athlete Triad” and as a consequence of decreased bone mineral density had been started on long-term bisphosphonates. Though this medication has been proposed as a treatment for stress fractures, an anabolic homeostatic bone state is required; this is known to be deficient in the presence of eating disorder and low body mass index. A non-fibrous atrophic non-union was found at the time of surgery. The patient has responded well to operative fixation including bone graft and modification of risk factors, which included stopping bisphosphonate therapy.
<Keywords: Bisphosphonate; Stress fracture; Bone mineral density
Stress fractures occur as a result of overuse injuries to bone, either secondary to bone fatigue of bone insufficiency [1]. They represent approximately 10% of the overuse injuries in sport and are most common in the lower limbs of runners.
Young women who suffer from “Female Athlete Triad” are at particular risk of stress fractures. The syndrome comprises interrelated eating disorders, amenorrhoea and osteopososis [2]. The consequence of lost bone mineral density can be devastating [3]. The condition, though well recognised in elite and competitive level athletes, where body composition can have great influence on performance, also occurs in the general population and is in many ways is a manifestation of the societal pressure on body image.
Osteoporosis is a disease characterised by low bone mass and micro architectural deterioration leading to increased risk of fracture [4]. Severe osteoporosis in young female adults is defined as a bone mineral density of more than -2.5 SD below the mean, plus one or more fragility fractures. The cause for loss of bone mass is thought to be similar to that of the postmenopausal woman where a hypoestrogenic state exists. The occurrence of disordered eating and low calcium intake along with menstral dysfunction exacerbates this loss [2]. Of note, bone mineral density is lost at the greatest rate in the 5-6 years following onset of amenorrhea, however, duration of amenorrhea in the presence of energy imbalance of as little as 6-12 months has been correlated in significant bone density loss, if not identified and treated in this crucial period this loss can be irreversible [5,6].
In an effort to modify the decrease bone mineral density bisphosphonates have been proposed as a potential treatment [7]. Their role in postmenopausal women is well founded where the marked inhibitory action on osteoclast-mediated bone resorption has led to successful increases in bone mass and decreased fracture risk [8]. Their action has also been utilised in the treatment of athletes with stress fractures, however this is controversial and has been poorly investigated [8].
The use of bisphosphonates in young females remains controversial. Their potential teratogenic effects have meant that their use is restricted to premenopausal women who continue to have fragility fractures and bone loss [7]. In the presence of a fracture there also remains a concern that the suppression or bone remodelling may also interfere with fracture healing [9].
The utility of bisphosphonates in female athlete triad, when a fracture is present, represents a theoretical concern yet evidence based guidance is very limited on the subject. To date there are no case studies that report a fracture non-union in a patient with female athlete triad treated with bisphosphonates.
A 27yr old female receptionist and keen runner were assessed initially in an orthopaedic outpatient clinic complaining or anterior shin pain. The patient had a past history of anorexia and previous insufficiency fractures to the pubic rami and stress fractures to the left 2nd metatarsal. She had regular input from her General Practitioner and Rheumatologist and 3 years prior to presentation and following DEXA scanning had been started on Bisphosphonate and Calcium supplementation. Rami fractures and metatarsal fractures healed fully with conservative treatment.
At initial presentation she complained of pain over the proximal left tibia when running. Radiographs revealed a transverse fracture of the proximal tibia involving the anterior cortex (Figure 1). A conservative management approach was initiated with initial full leg casting followed by functional brace and modified weight bearing. At 2 months, callus was seen on plain radiograph, brace removed but continued modification in weight bearing. At 3 months patient starts to use the cross trainer at the gym, no symptoms of pain on activity and no pain to palpation on examination.
At 4 months the patient was admitted to hospital with a displaced proximal third tibial fracture at the sight of the stress fracture (Figure 2). The mechanism of injury was a low-energy mechanical fall on a wet paving slab.
Open reduction internal fixation was undertaken for the displaced proximal third tibia fracture. Intraoperative findings were of poor bone quality with a brittle texture to the cortical bone. A non-fibrous atrophic non-union was present at the fracture site.

Figure 1:AP Radiograph showing proximal tibial stress fracture at initial presentation.

Figure 2:Lateral Radiograph showing the displaced fracture sustained at time of traumatic injury.
A locking plate system was used (Zimmer®, UK). The fracture was held with a single plate applied anterolaterally with 4 cortices held distally to the fracture and 6 proximally. Autograft was harvested from locally resected decortication and was applied as a corticocancellous on-lay graft.
Post-operatively she was held partially weight bearing for 3 months. A low-intensity pulsed ultrasound device was used as an adjunct (EXOGEN®, Smith and Nephew, UK) . Her bisphosphonates were discontinued.
At 9 months following surgical intervention she is mobilising fully weight bearing. She is pain free at the site of the fracture. Radiological investigation reveals callus healing (Figure 3). She continues to modify her weight bearing and is yet to return to running.
Tibial shaft fractures constitute approximately half of the reported lower limb stress fractures [1]. Patients generally present with a history pain that is gradually getting worse either at rest or progressively earlier during activity. Examination may reveal localised tenderness. The mainstay of diagnosis is through imaging. The diagnosis of the above patient was assisted through plain radiographs demonstrating a visible fracture.
Delayed union mid-tibia stress fractures represent about 5% of tibial stress fractures [10] and typically involve the anterior tibial cortex. They were originally reported in ballet dancers by Burrows in 1956 where it was commented that failure to heal was likely caused by persistent provocative activity producing stress across the distraction surface of the bone [11].
The conservative approach has been reported as variably successful for this particular form of tibial stress fracture. Of importance however has been progression to surgery only in those who have persistent symptoms. One case report has commented on the presence of nonunion in a patient who was able to participate in competitive football with very limited pain [12]. The case presented here further highlights a patient who progressed to non-union but was able to return to activity with minimal if any discomfort. Hence, surgical intervention was not felt appropriate initially whilst clinically the conservative approach appeared to be consistent with an improvement in symptoms.
Her risk factors for progression to non-union were numerous and include the position of her fracture, her nutritional state and potential poor adherence to conservative measures. However, there were also important modifiable pharmacological risk factors that were not noted until her traumatic fracture displacement. She had, for approximately 3 years, been using bisphosphonates prescribed following DEXA scanning. Bisphosphonates have an inhibitory effect on osteoclast function and hence and effect on slowing the process of osteoporosis. They have in the past been used for the treatment of stress fractures however this is poorly evidenced based. A case series of five female atheletes with tibial fractures treated with bisphosphonates appeared promising [13], though no clear comment of efficacy can be made in this uncontrolled study.
Their beneficial mechanism of action is an anti-catabolic process (bone destruction) in the remodelling phase, however for this to be effective the anabolic (bone forming) mechanisms must be adequate [8]. In the case of the “Female Athlete Triad” the anabolic process is deficient primarily due to poor nutritional state. Though bisphosphonates have been found to increase bone mineral density in young women with anorexia nervosa [7], in the presence of a high-risk stress fracture their effect may in-fact be quite destructive.
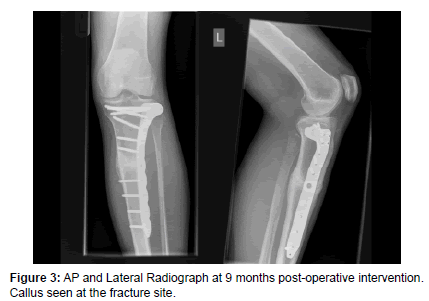
Figure 3:AP and Lateral Radiograph at 9 months post-operative intervention. Callus seen at the fracture site.
Concern regarding long term bisphosphonate use and subtrochanteric fracture in the elderly has been widely reported over the last few years, with recommendations to stop the medication whilst the patient is evaluated if they present with atraumatic hip, groin or leg pain [14]. This case highlights concern in a younger demographic where there is requirement to stop bisphosphonate therapy in the presence of a tibial stress fracture. Clearly, those young patients taking bisphosphonates for low bone mineral density are at a higher risk of sustaining a stress fracture; when that occurs the physician should take particular note of the patient’s nutritional state. Where there is concern that bone remodelling will be effected by poor nutritional state, discontinuation of bisphosphonate therapy should be considered.