Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Case Report - (2016) Volume 5, Issue 1
Nocturnal tongue biting presents as a diagnostic dilemma, especially in children. We report two siblings with nocturnal tongue biting who were ultimately diagnosed with Faciomandibular Myoclonus (FMM) based on video polysomnography.
Keywords: Nocturnal tongue biting; Faciomandibular myoclonus; Bruxism; Hereditary chin trembling; Oromandibular myoclonus; Clonazepam; Recurrent tongue biting
Faciomandibular myoclonus involves the sudden, forceful contraction of masticatory muscles during sleep [1] and presents as recurrent tongue biting.
We present two pediatric cases of familial FMM with a brief review of the literature.
A four-year-old boy was referred for evaluation of recurrent tongue biting during sleep which was thought to have commenced as early as 8 months of age. Episodes were intermittent with no obvi-ous precipitating factors and occurred soon after sleep onset. Rarely, events also occurred when awake.
He had occasional snoring and moderate daytime sleepiness but no obvious sleep apnea or behavioural concerns. At presentation, significant ulceration of the lateral aspect of the tongue and a minor amputation defect of the tongue were noted. At the age of 14 months, protective dental material was placed on his teeth to smooth the cusps and reduce trauma.
Use of a soft oral splint and a trial of melatonin were undertaken with no appreciable benefit. Surgical release of tongue tie was also performed at age 3 years without improvement in tongue biting.
The younger sibling presented at the age of 22 months with similar episodes, often with blood staining of his pillow. He also had mild bruxism.
Apart from ulceration and scarring of the tongue, examination of both siblings, including neurodevelopmental assessment, was normal. There was no family history of epilepsy, chin trembling or sleep-related disorders other than their father having bruxism.
Video Polysomnography (PSG) was performed in the older sibling with an Electromyography (EMG) lead placed over the masseter muscle. No respiratory events were recorded. There was no evidence of seizure activity on the limited PSG montage.
Four episodes of tongue biting were noted, two in REM sleep and two in non-REM sleep. During each episode, sleep was disturbed leading to crying out with pain. Video recordings of the episodes were consistent with FMM rather than bruxism.
A PSG epoch demonstrating one of the events is presented in Figure 1. Formal awake and asleep EEGs in both siblings were normal.
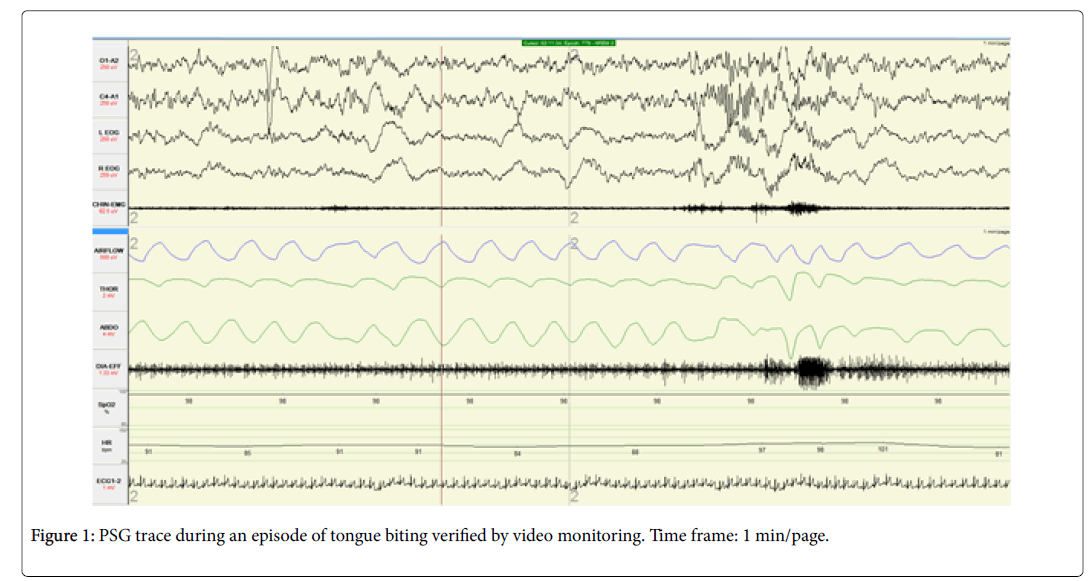
Figure 1: PSG trace during an episode of tongue biting verified by video monitoring. Time frame: 1 min/page.
Following these investigations, a diagnosis of FMM was established. As the clinical presentation in the younger sibling was identical, PSG was not performed.Management incorporated treatment with clonazepam 1 mg nocte in the older sibling and 0.5 mg nocte in the younger sibling.
Symptoms initially improved in the older sibling but then recrudesced, hence clonazepam was increased to 1.4 mg nocte with improvement. The parents ceased medica-tion in the younger sibling as his symptoms became less problematic.
The differential diagnosis of nocturnal tongue biting includes bruxism, nocturnal epilepsy, hereditary chin trembling, hereditary geniospasm and FMM. FMM is subcortical in origin. It entails the sudden and forceful contraction of masticatory muscles during sleep, either isolated or in clusters, and is considered to be a form of brainstem reticular myoclonus involving the 5th and 7th cranial nerve nuclei along polysynaptic pathways [1]. The usual presenting feature of FMM is nocturnal tongue biting, often initially diagnosed as sleep bruxism [2] or epilepsy [3].
Kato et al. [2] performed PSG in 41 patients diagnosed with bruxism. Four (10%) had what they de-scribed as oromandibular myoclonus. Bruxism, as in our case, has been found as an associated phenomenon in some cases of FMM [1].
Hereditary chin trembling, an autosomal dominant condition, has also been associated with noctur-nal tongue biting. Johnson et al. [4] have reported nocturnal myoclonus and tongue biting in dizygotic twins with hereditary chin trembling. Goraya et al. [5] have described a case of hereditary chin trembling presenting as nocturnal tongue biting in a 13-month-old child.
A case of sporadic geniospasm in an adolescent boy presenting with nocturnal tongue biting episodes has also been reported [6]. Other pediatric cases of nocturnal tongue biting attributed to developmental and maturational phenomena have also been described.
PSG results vary between studies. Myoclonic jerks, predominantly in non-REM sleep, are noted in the majority of cases [1,3]. In our case, myoclonic jerks were observed in both REM and non-REM sleep.
No consensus for treatment exists for this condition. A beneficial response to clonazepam has been reported in some cases with only a partial response in others [1]. In our siblings, clonazepam was partially successful. One case report described improvement in the form of reduced arousals with an interdental plate leading to improved sleep but there was no effect on tongue biting itself. This approach has also been offered to our patients.