Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2018) Volume 8, Issue 2
Objective: Natural killer cell (NK-cell) has an important role in tumor immunosurveilance. We investigate the NKcell count and its function in producing IFN-γ on normal cervix, subclinical high risk-HPV (hr-HPV) infection, precancerous lesion of cervix, and cervical cancer in order to understand the natural history of uterine cervical cancer.
Methods: This is a descriptive comparative numerical study with more than two unpaired group with total subjects of 40 females who met the inclusion and exclusion criteria. Samples were gathered from cervical tissue using cytobrush and were processed in the laboratory to calculate NK-cell count and NK-cell expression of IFN-γ by phyta hemagglutinin (PHA) stimulation using flow cytometry. Data was analyzed using Kruskal Wallis and post hoc analysis was done to determine the difference between groups.
Results: The mean NK-cell count on normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer were 2.6%, 11.6%, 12%, and 7.4%. The mean NK-cell producing IFN-γ on normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer were 8.1%, 3.3%, 1.1%, and 1.8%. There is significant difference of NK-cell count between 4 groups (p=0.001) but there is no significant difference of NK-cell producing IFN-γ (p=0.577).
Conclusion: NK-cell count on normal cervix was significantly lower than other group but it has highest expression of IFN-γ after stimulation. On the other hand, precancerous lesion and cervical cancer has lower expression of IFN-γ after stimulation. Eventhough statistically there is no NK-cell activity difference, this study shows that NK-cell activity in disease groups were impaired. Further study is needed to understand NK-cell activity and its role in cervical cancer natural history. Nowdays, NK-cells as immunotherapy are potential tools for cancer therapy. In the future, we hope that NK-cell activity can be a parameter of cervical cancer progression and strategy to treat cervical cancer.
Keywords: NK-cell; IFN-γ; Cervical Cancer; HPV; Precancerous lesion
Cervical cancer is one of the main health issues and the second most common female malignant neoplasm in Indonesia. There were 20.928 new cases of cervical cancer and 9498 cancer-related deaths in 2012 in Indonesia. In years to come, it is predicted that there will be an increase in new cases and mortality since there hasn’t been any effective prevention and treatment program [1,2].
Cervical cancer is one of the cancers that can be prevented because the etiology is known. Human Papilloma Virus (HPV) has been acknowledged as the etiology of cervical cancer. Although HPV is well established to be the cause of cervical cancer, only a small percentage of HPV infections will develop clinically or histologically recognizable lesion [3]. Most of the infections will have resolutions and about 70-90 percent of HPV infection would not be detected in 1-2 years. High-risk HPV (hr-HPV) infection that has oncogenic characteristic is the most important factor contributing to the progression of HPV infection into cervical cancer [4]. However, there were other contributing factors, such as host immune response [5,6]. Innate immune response represent the first line the first line of defense against HPV infection and transforming cells. If the host has good immune response, the infection will be cleared or become subclinical [7].
Natural killer cell (NK-cell) has an important role in tumor immunosurveilance.8 NK-cell has the capacity to recognize and eliminate infected cells and transformed cell without prior sensitization by: (1) its cytotoxic activity through secretion of perforin/granzym and (2) cytokine production [8-11]. Some studies found that there was a decreasing number of NK-cell and its activity in cervical cancer. Interferon gamma (IFN-γ) is one of the cytokines produced by activated NK-cell. It is believed that that (IFN-γ) can control viral infection by increasing NK-cell cytotoxic activity. In some studies, higher (IFN-γ) correlates with higher clearance in high-risk HPV infection, while low (IFN-γ) is found in women with cervical cancer [12,13].
There are still few studies that explore NK-cells and its activity in relation with the natural progression of cervical cancer. The role of NK-cell and its (IFN-γ) secreting activity related to HPV infection and progressivity hasn't been fully understood. From the clinical perspective, NK-cell count and its activity can be used as the risk indicator of cervical cancer, especially in high-risk population. Nowdays, NK-cells used as immunotherapy are potential tools for cancer therapy. If proven significant, the result of this study can be used as a new strategy in secondary and tertiary prevention against cervical cancer.
Natural killer cell (NK-cell) has an important role in tumor immunosurveilance. We hypothesized that there will be a variance in NK-cell counts and its activity in different population. We investigate the NK-cell count and its function in producing IFN-γ on normal cervix, subclinical high risk-HPV (hr-HPV) infection, precancerous lesion, and cervical cancer in order to understand the natural history of uterine cervical cancer.
This study is a cross-sectional study with total sample of 40 female subjects. The subjects were divided into four groups of: normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer. Each group consists of 10 female subjects.
Inclusion criteria in this study were: sexually active women aged 20-60 years old; normal cytology and negative HPV DNA (group 1); normal cytology with positive hr-HPV DNA (group 2); abnormal cytology in precancerous lesion with positive or negative HPV DNA (group 3); abnormal histopathology result in cervical cancer (group 4); and signed consent to be included in the study. Exclusion criteria were menstruation, malnutrition, pregnancy, presence of autoimmune disease or HIV, long-term steroid medication, and genito-urinary tract infection.
Cervico-vaginal samples were taken by cytobrush from the subjects who met all the inclusion and exclusion criteria. Samples were transferred into tubes containing buffer and were processed in the laboratory to calculate the NK-cell count and NK-cell expression of IFN-γ after phytahemagglutinin (PHA) stimulation. Flow cytometry analysis was done to determine the number of NK-cell (CD16+ CD56+ dan CD3-) and NK-cell expressing IFN-γ. The number of NK-cell was compared with the number of CD45+ (in percentage.)
Data was analyzed using SPSS version 23. This is a descriptive comparative numerical study with more than two unpaired group. Data was analyzed Kruskal Wallis. Post hoc analysis was done if there were any significant different between groups. This study was approved by Ethics Committee for Health Researches Faculty of Medicine Universitas Indonesia.
There were total 40 subjects: 10 subjects with normal cervix; 10 subjects with subclinical hr-HPV infection; 10 subjects with precancerous lesion and 10 subjects with cervical cancer. The mean age of subjects was 45.6 years old. Mean age of subjects in groups of normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer were 47 years old, 44.5 years old, 41 years old and 48 years old. In hr-HPV group, 5 patients (50%) had mono-infection and 5 patients (50%) had multiple hr-HPV infection. The most common hr-HPV type was type 52 (5 patients), type 16 (3 patients) and type 66/68 (3 patients). Types of hr-HPV in subclinical infection were shown in Table 1.
| HPV Types | Subclinical hr-HPV infection (n=10)* |
|---|---|
| HPV 16 | 3 |
| HPV 18 | 1 |
| HPV 52 | 5 |
| HPV 53 | 1 |
| HPV 56 | 1 |
| HPV 59 | 2 |
| HPV 66/68 | 3 |
*5 subjects have multiple HPV infection
Table 1: Types of hr-HPV detected in subclinical infection.
NK-cell Count
In this study, mean NK-cell count in four groups of normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer were: 2.6%, 11.6%, 12%, and 7.4% respectively. The lowest proportion was in normal cervix group (2.6%), while the highest proportion was in precancerous lesion group (12%). Analysis was performed using Kruskal Wallis. The analysis produced significant difference in NK-cell count (p=0.001) between 4 subject groups (Table 2).
| Variable | n | Mean (SD) | Median (Min-Max) | P Value# |
|---|---|---|---|---|
| Number of NK-cell (%) | 0.001 | |||
| Normal cervix | 10 | 2.60 (0.96) | 2.5 (1-4) | |
| Subclinical HPV infection | 10 | 11.6 (10.88) | 7.5 (2-38) | |
| Precancerous lesion | 10 | 12.00 (8.93) | 10.5 (3-31) | |
| Cervical cancer | 10 | 7.40 (2.91) | 7.5 (1-11) |
#Analysis using Kruskal Wallis
Table 2: NK-cell count.
Post-hoc analysis was performed using Mann Whitney and there were significant difference between these groups:
(1) normal cervix and subclinical infection.
(2) normal cervix and subclinical infection.
(3) normal cervix can cervical cancer. This study found no significant NK-cell count difference between the cervical cancer and subclinical hr-HPV group; and the precancerous lesion and cervical cancer group (Table 3). Flow cytometry analysis of NK-cell count is depicted in Figure 1.
| Comparison of NK-cell count | P Value |
|---|---|
| Normal cervix vs subclinical hr-HPV infection | 0.001 |
| Normal cervix vs precancerous lesion | 0.001 |
| Normal cervix vs cervical cancer | 0.002 |
| Subclinical hr-HPV infection vs precancerous lesion | 0.571 |
| Subclinical hr-HPV infection vs cervical cancer | 0.571 |
| Cervical cancer vs precancerous lesion | 0.548 |
Table 3: Post-hoc Mann Whitney analysis of NK-cell count.
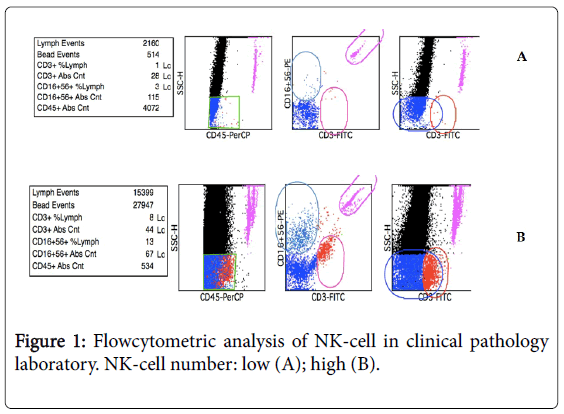
Figure 1: Flow cytometric analysis of NK-cell in clinical pathology laboratory. NK-cell number: low (A); high (B).
NK-cell activity in producing IFN-γ
After measuring the number of NK-cells, this study was followed by assessing the activity of NK-cell in producing IFN-γ. Flow cytometry was used to evaluate the intracellular activity of NK-cell (Figure 2). The mean number of NK-cell producing IFN-γ in normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer were 8.1%, 3.3%, 1.1% and 1.8% respectively. Kruskal Wallis analysis between those 4 groups yields no significant result. The result is depicted in Table 4.
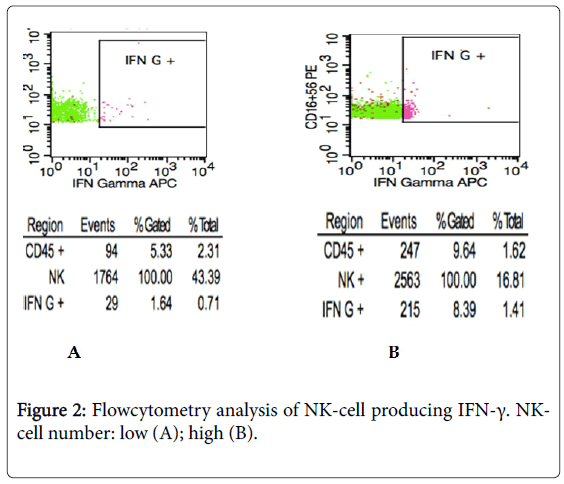
Figure 2: Flow cytometry analysis of NK-cell producing IFN-γ. NKcell number: low (A); high (B).
| Variable | n | Mean (SD) | Median (Min-Max) | P Value# |
|---|---|---|---|---|
| NK-cell producing IFN-γ (%) | 0.577 | |||
| Normal cervix | 10 | 8.145 (16.63) | 0.745 (0.1-49.6) | |
| Subclinical HPV infection | 10 | 3.393 (6.40) | 1.35 (0.13-21.15) | |
| Precancerous lesion | 10 | 1.1750 (1.61) | 0.63 (0.02-5.56) | |
| Cervical cancer | 10 | 1.871 (3.20) | 0.375 (0.06-8.39) |
#Analysis using Kruskal Wallis
Table 4: Number of NK-cell producing IFN-γ.
Natural killer cells are important components of the innate immune system, owing to their cytokine production and cytotoxic activity against target cells. In clinical settings, in vitro NK-cell activity has been an important predictor of possible correlations between NK-cell activity and disease outcome or progression. NK-cell count will increase if there is an exposure from external pathogen. Viral infected cells, tumor cells or inflammation will trigger signaling cascade that can affect the immune response.
In this study, mean NK-cell count in four groups of normal cervix, high risk HPV (hr-HPV) subclinical infection, precancerous lesion, and cervical cancer were: 2.6%, 11.6%, 12%, and 7.4% respectively. The lowest NK-cell count was in normal cervix group. This result is in accordance with another study by Trinova, et al. (NK-cell count 2.7% in normal cervix group) [14]. The result showed that without any external stimuli or the presence of inflammation, NK-cell count will be relatively low in cervix. Conversely, in groups with subclinical hr-HPV infection, precancerous lesion, and cervical cancer, there was an increase of NK-cell count. It was inferred that infection process or chronic infection could increase the number of NK-cells. In some cancer patients, the increase of NK-cell counts was associated with better prognosis; however it also relied on the remaining functional NK-cell during tumourogenesis [15].
IFN-γ is one of the important cytokines produced by NK-cells that can act as an antivirus and tumor regulation [16,17]. HPV virus has a few avoidance mechanisms from the innate immune response. One of them is by interfering the production of IFN-γ through oncogenic protein in hr-HPV (protein E6 and E7). IFN-γ can increase the activity of NK-cells and macrophage activity; and work together with dendritic cells to induce the differentiation of T-helper [18-20]. In this study, the mean number of NK-cell producing IFN-γ in normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer were 8.1%, 3.3%, 1.1% and 1.8% respectively. Nevertheless, there wasn't any statistical significance between the subject groups (p=0.557). In one study, it was found that in higher IFN-γ, hr-HPV infection tend to have higher clearance rate; while other study also showed that women with cervical cancer tend to have lower IFN-γ level [12]. However, there are also studies that indicate that IFN-γ level is not significantly different between healthy group and cervical cancer group [21,22]. Correlation IFN-γ and cervical cancer progression still unclear. Eventhough statistically there is no activity different between groups, but from the result we can see the mean of nk-cell expressing IFN-γ on normal cervix group has the highest number. It shows the NK-cell activity on disease groups were impaired. We still cannot conclude the different NK-cell activity between groups, because the power of this study is small.
Although one of the functions of NK-cell is releasing cytokines, such as IFN-γ, it doesn't represent all of NK-cell function. One of the main functions of NK-cell is its cytotoxic activity that can recognize pathogen without prior sensitization. While those two functions correlates with each other, they have different activating mechanism (Park, et al.). Although there was no statistical significance in NK-cell producing IFN-γ between the groups, the cytotoxic activity of NK-cell also couldn’t be determined which was not explored in this study. Hence, the whole function of NK-cell couldn't be observed entirely.
This is one of few studies that show the correlation between NK-cell count and cervical cancer natural history using samples from cervical tissue. Through cervical tissue samples, we can associate the number and activity of NK-cell with the natural history of HPV infection locally. Nevertheless, this study cannot portray the whole picture of cervical cancer natural history. The weakness of this study is the number of sample, which is still lacking.
The highest mean NK-cell count in four groups of normal cervix, high risk HPV (hr-HPV) subclinical infection, precancerous lesion, and cervical cancer are: 2.6%, 11.6%, 12%, and 7.4% respectively. There is statistical significance between subject groups (p=0.001). The lowest number found on normal cervix (2.6%), it shows no exposure from pathogen that increase NK-cell number. The mean number of NK-cell producing IFN-γ in normal cervix, subclinical hr-HPV infection, precancerous lesion, and cervical cancer are 8.1%, 3.3%, 1.1% and 1.8% respectively. There is no statistical significance in NK-cell producing IFN-γ between the subject groups, but normal cervix group have the highest NK-cell expressing IFN-γ. It shows that on diseases group the activity were impaired even though we cannot conclude because the power of the study is still lacking. There is a need for further studies with more samples and a follow through study to generate more conclusive result. On the future, we hope that NK-cell activity can be a parameter of cervical cancer progression and strategy to treat cervical cancer.