Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 1
Background: Oral appliances have emerged as an important alternative in treating patients with mild-moderate obstructive sleep apnea (OSA). They are effective, simple to use and well tolerated by the patient compared to other therapeutic solutions, such as continuous positive airway pressure (CPAP) or surgery of the upper airways. Aim: The aim of this preliminary study was to assess the effectiveness of a new mandibular advancement device, the BestMAD, in the treatment of OSA patients.
Materials and methods: We selected 10 patients, 9 males and 1 female, with an average age of 51.5 years, affected by OSA, with a BMI (Body Mass Index) value ≤25 kg/m2. All patients used the BestMAD for at least 6 months. A control polysomnography was repeated after 6 months and a questionnaire was administered to assess the side effects eventually felt by the patient.
Results: After treatment with BestMAD, a statistically significant improvement was found in AHI (p=0.0051), RDI (p=0.0051) and ESS (p=0.0049). With regard to adherence to the treatment, 8 patients claimed to have used the BestMAD for the entire duration of nocturnal rest, while the remaining 2 only for a few hours at night.
Conclusions: BestMAD is a comfortable device which has proved effective in improving the polysomnographic parameters.
Keywords: Obstructive sleep apnea; Oral appliance; Mandibular advancement device
Obstructive sleep apnea (OSA) is a common clinical condition affecting 2-26% of the general population [1,2]. It is characterized by partial or complete obstruction of the upper airways during sleep, resulting in repetitive events of apnea and hypopnea with a consequent negative impact on the health and the behavior of patients [3,4]. Furthermore, OSAS is considered today a cardio-metabolic disease with a great impact on public health, related to increased risk of hypertension, cardiovascular disease and mortality, methabolic imbalance and cerebrovascular accidents [5-7]. The treatment with continuous positive airway pressure (CPAP) is considered the gold standard, but some patients find it intolerable [8]. A study assessing compliance with CPAP, found that only 46% of patients used the device for more than 4 hours per night for more than 70% of the nights [9]. For patients with mild or moderate OSA, oral appliances may be appropriate therapy as suggested by the Standards of Practice Committee of the American Academy of Sleep Medicine and the Deutshe Gesellschaft fur Zahnarztliche Schlafmedizin [10,11]. In recent years, several clinical randomized trials compared the effectiveness of treatment with CPAP and oral devices [12,13]. Although CPAP demonstrated superior efficacy in terms of apnea-hypopnea index (AHI) reduction, self-reported compliance with oral appliance was higher. The resulting effects on clinical outcomes in patients with mild, moderate or severe OSA were equivalent or better in the oral appliance. These devices are designed to increase the pharyngeal airway space (PAS) by three fundamental mechanisms: 1) the protrusion of the jaw and the tongue away from the back wall of the pharynx; 2) the stabilization of the jaw and the inhibition of the opening of the mouth, allowing the anterior positioning of the hyoid bone and the tongue; 3) the implementing of the vertical dimension to induce a reflex at the level of the TMJ, which activates the genioglossus muscle and tends to extend the tongue [13-16]. On the basis of scientific assessments and international guidelines, the use of the protrusion guides is recommended for the treatment of sleep-related breathing disorders as an alternative choice after a previous attempt treatment with CPAP, or as initial therapy in the presence of primary snoring, upper airway resistance syndrome (UARS), mild-moderate OSA with little symptoms in conditions of sufficient intraoral anchorage [17]. More than 60 different oral appliances are in use, with considerable variations in design [18-21]. Mandibular advancement devices (MAD) have been the most intensely researched, and their effectiveness documented by the Cochrane Collaboration as the highest level of scientific evidence [22,23]. In 2007, Dr. Enzo Iacomino, Dr. Vittorio Bisogni and the expert in orthodontic technique Mr. Franco Pestilli developed the BestMAD, a device for mandibular and tongue base advancement for the treatment of OSA in patients intolerant to CPAP, alone or in combination with other therapeutic options. The device was clinically applicable since 2008. The purpose of this study was to evaluate the effectiveness of BestMAD in the treatment of patients with OSA.
BestMAD
The BestMAD is a tailor-made patient device, structured in two arches that run on each other (Figure 1).
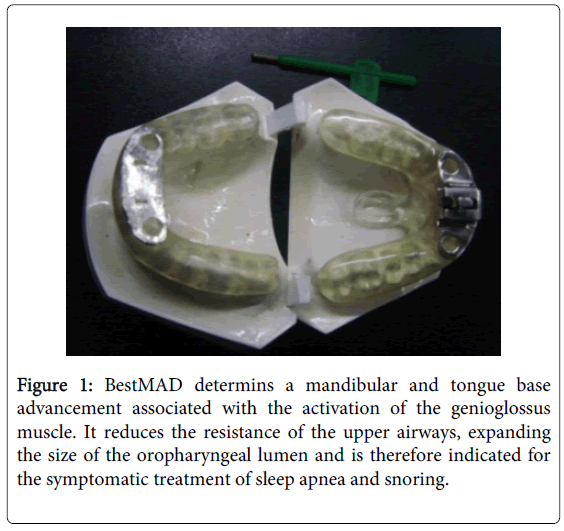
Figure 1: BestMAD determins a mandibular and tongue base advancement associated with the activation of the genioglossus muscle. It reduces the resistance of the upper airways, expanding the size of the oropharyngeal lumen and is therefore indicated for the symptomatic treatment of sleep apnea and snoring.
The part in contact with the teeth and the gingival mucosa (1 mm) is soft and made of vacuum-polyurethane, while the outside part is rigid and made of copolyester completed with acrylate (1 mm). An adjustable screw (MDSA® Pty Ltd, Australia) joins the two arches, and the protrusion is adjustable from a minimum of 4 mm to a maximum of 10 mm (2 mm in crackdown) (Figure 2).
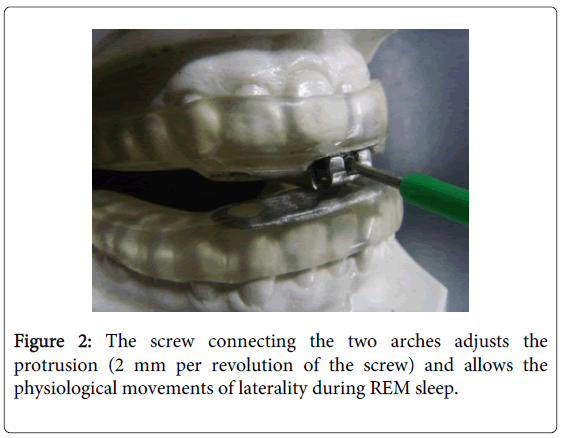
Figure 2: The screw connecting the two arches adjusts the protrusion (2 mm per revolution of the screw) and allows the physiological movements of laterality during REM sleep.
The screw provides lateral movements (compatible with any physiological movements during the REM stage of sleep) (Figure 3) the initial adjustment of the protrusion is established on clinical and radiological data and is generally of 6 mm.

Figure 3: Lateral movements with BestMAD.
It is not advisable to exceed 10-12 mm in protrusion. A proprioceptive indicator or oral tongue stimulator (Figure 4) was included in the device as reference point for the anterior positioning of the tongue.
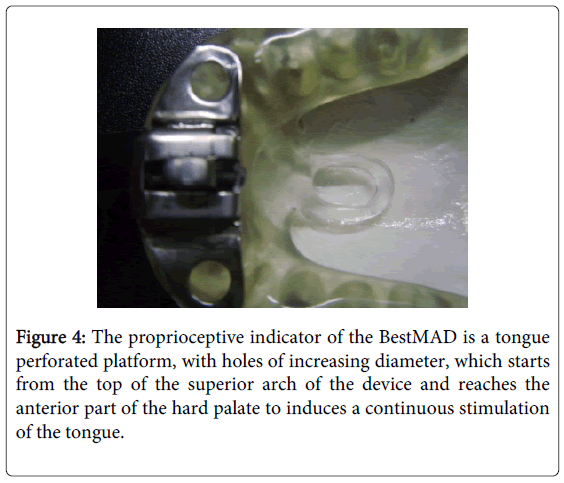
Figure 4: The proprioceptive indicator of the BestMAD is a tongue perforated platform, with holes of increasing diameter, which starts from the top of the superior arch of the device and reaches the anterior part of the hard palate to induces a continuous stimulation of the tongue.
Patients
A total of 10 patients (9 males and 1 female, mean age 51.5 years, range 20-70) selected from those relating to the service for the diagnosis and treatment of sleep-disordered breathing of the Hospital “San Pietro Fatebenefratelli” in Rome and to the ENT department of the Hospital “San Salvatore” in L'Aquila from 2008 to 2013, were enrolled in the study. The inclusion criteria were: a diagnosis of OSA with no compliance to the CPAP, BMI (Body Mass Index) ≤ 25 kg/m2, hypopharyngeal collapse observed in the fiberoptic endoscopy with Muller maneuver and a positive mandibular advancement test at the sleep endoscopy. All the patients underwent a preliminary ENT and dental examination, complete overnight cardio-respiratory polysomnography, medical questionnaire on the sleep-disordered breathing and related conditions, Epworth Sleepiness Scale (ESS) to measure daytime sleepiness, nasolaryngeal fiberoptic endoscopy with Muller maneuver, sleep endoscopy with mandibular advancement test, Computerized Tomography (CT) of the facial bones. All the selected patients were treated with the BestMAD. Patients no. 4, 6, 7, 8, 9 and 10 also underwent oropharyngeal surgery before starting the therapy with the BestMAD. All of them had an uvulopalatopharyngoplasy, and one of them also had a septoplasty (patient no. 10). A control polysomnography was repeated after six months and a questionnaire we specifically created was administered to assess the side effects eventually felt by the patient (difficulty in chewing and/or breathing, drooling, xerostomia, dental, lingual, gingival and/or mandibular discomfort, headache, changes in occlusal, masseter and/or temporomandibular joint pain, spinal pain, dizziness).
Clinical data collected before and after 6 month of treatment with BestMAD are shown in Tables 1 and 2.
| Patients no. | AHI | RDI | Snore ind (/h) | ODI (/h) | ESS |
|---|---|---|---|---|---|
| 1 | 32 | 44 | 330.7 | 18.8 | 5 |
| 2 | 28.5 | 52.1 | 359.7 | 23 | 12 |
| 3 | 20 | 24.8 | 435.3 | 5.8 | 9 |
| 4 | 3 | 41.4 | 145 | 0 | 7 |
| 5 | 2.3 | 4.2 | 32.5 | 0.4 | 8 |
| 6 | 46.4 | 38.8 | 294 | 67 | 8 |
| 7 | 10.2 | 92 | 389 | 1.2 | 11 |
| 8 | 34.8 | 63.8 | 224 | 21.1 | 7 |
| 9 | 36.7 | 30 | 250 | 5.3 | 6 |
| 10 | 27 | 49 | 327 | 19 | 8 |
| Mean Values | 24.09 | 44.01 | 278.72 | 16.16 | 8.1 |
Table 1: Clinical data before starting the therapy with Best-MAD. AHI: Apnea-Hypopnea Index. RDI: Respiratory Disturbance Index. ODI: Oxygen Desaturation Index. ESS: Epworth Sleepiness Scale.
| Patients no. | AHI (/h) | RDI (/h) | Snore ind (/h) | ODI (/h) | ESS | |
|---|---|---|---|---|---|---|
| 1 | 0.1 | 25 | 184.3 | 0 | 3 | |
| 2 | 14.1 | 28.7 | 408.5 | 12.8 | 4 | |
| 3 | 1.1 | 2.9 | 488.1 | 0.1 | 3 | |
| 4 | 2.5 | 35.5 | 198.6 | 0.7 | 4 | |
| 5 | 0.7 | 0.7 | 56.7 | 0.4 | 3 | |
| 6 | 16.6 | 20.3 | 194 | 15 | 3 | |
| 7 | 4.6 | 33 | 33 | 0.3 | 2 | |
| 8 | 7.8 | 22.8 | 120 | 1.1 | 2 | |
| 9 | 12.7 | 10 | 150 | 1.3 | 3 | |
| 10 | 2.6 | 5 | 128 | 1.9 | 2 | |
| Mean Values | 6.28 | 18.39 | 196.12 | 3.36 | 2.9 | |
Table 2: Clinical data after 6 months of therapy with Best-MAD. AHI: Apnea-Hypopnea Index. RDI: Respiratory Disturbance Index. ODI: Oxygen Desaturation Index. ESS: Epworth Sleepiness Scale.
Statistical analysis was performed using the Wilcoxon test for all the parameters. This entails the need to bring the threshold of statistical significance by α=0.05 to α*=0.008.
The improvement of the values of AHI (Apnea-Hypopnea Index), RDI (Respiratory Disturbance Index) and ESS after treatment with BestMAD was statistically significant (p=0.0051, p=0.0051, and p=0.0049 respectively). The ODI (Oxygen Desaturation Index) and the index of arrhythmia were reduced drastically, even if the values were not statistically significant (p=0.0107 and p=0.0363 respectively). The snore index remained almost unchanged (p=0.0743).
With regard to adherence to the treatment and side effects, 8 patients claimed to have used the BestMAD for the entire duration of nocturnal rest, while the remaining 2 only for a few hours at night. Six of 10 patients complained of xerostomia, 6 of drooling, 4 of temporomandibular joint pain, 2 of dental discomfort, 2 of mandibular discomfort, 2 of respiratory irritation and 2 of masseter pain.
Data emerging from this study suggested the efficacy of the therapy with BestMAD in patients with OSA, alone or in combination with surgery. In our clinical practice, the use of BestMAD in selected patients has proved of high clinical efficacy, especially in patients with sleep apnea that occur mainly in the supine position, with a positive mandibular advancement test detected during the sleep endoscopy and hypopharyngeal collapse observed in the fiberoptic endoscopy with Muller maneuver.
In our opinion, one of the greatest strengths of the BestMAD consists in the oral tongue stimulator. The neurological control of tongue posture is surely determined by many factors, but the current state of our knowledge does not yet allow us to know their mode of action. The central nervous system processes sensory information, in particular the tactile and proprioceptive, which come from the dorsal surface of the tongue. The ability to recognize the position of the tongue and the surrounding anatomical structures depends largely on these sensory afferents, determining stereognosic and tactile discriminative ability. In most cases, atypical swallowing, abnormal tongue rest position, decreased sensitivity and OSA are associated [24-26]. Sensory impulses necessary for the maintenance of a proper tongue posture come from mutual stimulation of the dorsum of the tongue with the teeth and the mucosa of the hard palate. In orthodontic practice, some devices are commonly used to change the neuromuscular behavior of the stomatognathic apparatus through automatic acts committed unintentionally. These are described in the literature as "oral stimulators" or "reminders". The function of these devices is to normalize the muscle behavior in the dynamic (mastication, deglutition, phonation and mimicry) and in the static phases. From these neurophysiological considerations was born the idea of ??applying a tongue proprioceptive stimulus to the BestMAD. For its realization, we started from the classic oral stimulators known in the orthodontic practice, such as perforated plates or Tucat palatine pearl. The oral tongue stimulator placed on the BestMAD consists in a perforated platform (Figure 4) which reaches the anterior part of the hard palate and induces a continuous anterior stimulation of the tongue, expanding the pharyngeal airway space (PAS) during sleep.
Another strength of BestMad is the screw that connects the two arches of the device. In the first equipment we use, and in most of those commercially available, the structure is represented by a single block that is anchored on the maxilla and holds the lower jaw in a forward position. An adjustment screw regulates its advancement. We noticed that, in some patients (especially those with obesity, hypertrophy of the masseter and bruxism), the device was often detached from the maxilla during sleep, probably under the pressure of the unconscious movements of the jaw, resulting in a fall back of the jaw and tongue. From this evidence the idea to replace the old screw with a new connection between the two arches of the device that allows the movements of laterality keeping the jaw protrusion. In this way the kinetic energy of the can dissipate, avoiding the detachment of the device during the night.
In conclusion, the BestMad has proved to be a good choice among the many oral devices available on the market, either alone or in combination with other procedures, for the treatment of selected patients with OSA.
Considering that the BestMad should be used mainly at night and for the whole life, we have tried to make it as comfortable as possible, trying to prevent, at the same time, any kind of unwanted tooth movement. However, there is the need for further studies involving a greater number of patients and with a long-term control of the results.