Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Review Article - (2014) Volume 2, Issue 5
In the past, thrombotic thrombocytopenic purpura (TTP) was defined as a syndrome of the pentad of thrombocytopenia, microangiopathic hemolytic anemia, neurologic deficits, renal abnormalities and fever. To include patients with incomplete features, the pentad definition was replaced by the triad of thrombocytopenia, microangiopathic hemolytic anemia (MAHA), and neurologic deficits; or the diad of thrombocytopenia and MAHA. None of these definitions provides a clear distinction of TTP from atypical hemolytic uremic syndrome (aHUS) or other causes of the syndrome of MAHA and thrombocytopenia or thrombotic microanangiopathy. This brief review describes a mechanistic definition of TTP, provides a framework for assessing the role of various co-morbid conditions in the pathogenesis of the syndrome of thrombocytopenia and MAHA, and summarizes new insights of the natural course of TTP. Based on these new insights, a strategy of ADAMTS13-guided preemptive rituximab therapy is proposed to prevent relapses in patients with acquired TTP. Thrombotic thrombocytopenic purpura (TTP) has been defined as a clinical syndrome of pentad (thrombocytopenia, microangiopathic hemolytic anemia [MAHA], neurological deficits, fever and renal abnormalities), triad (thrombocytopenia, MAHA, neurological deficits) or diad (thrombocytopenia and MAHA). In addition to this uncertainty, there was also no consensus on whether and how patients with prominent renal failure or co-morbid conditions should be excluded. The difficulty of defining TTP as a clinical syndrome arises from two facts: More than one disorder may cause the syndrome of diad, triad or pentad; and some patients of TTP do not present with thrombocytopenia or MAHA.
Keywords: Atypical hemolytic uremic syndrome; Thrombotic thrombocytopenic purpura; Renal failure; Relapse; Rituximab
Thrombotic thrombocytopenic purpura (TTP) has been defined as a clinical syndrome of pentad (thrombocytopenia, microangiopathic hemolytic anemia [MAHA], neurological deficits, fever and renal abnormalities), triad (thrombocytopenia, MAHA, neurological deficits) or diad (thrombocytopenia and MAHA). In addition to this uncertainty, there was also no consensus on whether and how patients with prominent renal failure or co-morbid conditions should be excluded.
The difficulty of defining TTP as a clinical syndrome arises from two facts: More than one disorder may cause the syndrome of diad, triad or pentad; and some patients of TTP do not present with thrombocytopenia or MAHA.
Analysis of patients presenting with MAHA and thrombocytopenia reveals that in the absence of vascular devices such as ventricular assist devices, extracorporeal membrane oxygenator or prosthetic heart valves, MAHA and thrombocytopenia are associated with at least five different types of pathology in the arterioles and capillaries: von Willebrand factor (VWF)-platelet thrombosis; fibrin-platelet thrombosis; thrombotic microangiopathy (TMA); vasculitis/vasculopathy; and tumor cell embolism (intravascular clusters of tumor cells) (Table 1). Each of the lesions in turn may result from one or more etiologic mechanisms.
| Pathology | Characteristics | Example |
| VWF-platelet thrombosis | Luminal thrombi of VWF and platelets | TTP |
| Fibrin-platelet thrombosis | Luminal thrombi of fibrin and platelets | DIC, CAPS, HIT, PNH, HELLP |
| Thrombotic microangiopathy (TMA) | Endothelial swelling or disruption Subendothelial expansion Thrombosis at sites of endothelial disruption |
Shiga toxin-HUS Neuraminidase-HUS Anti-VEGF drugs Other drugs aHUS DGKE nephropathy MMACHC mutations (cobalamine C disease) |
| Vasculitis | Fibrinoid necrosis Inflammatory cell infiltration Destruction of IEL Fibrosis Occasional thrombosis |
Autoimmune vasculitis Infectious vasculitis Rocky Mountain spotted fever Fungemia Viremia |
| Vasculopathy | Intimal fibrinoid necrosis, fibrosis Duplication of IEL Occasional thrombosis |
Renal scleroderma |
| Tumor cell embolism | Intravascular clusters of neoplastic cells | Metastatic neoplasm |
Table 1: Arteriolar pathology associated with the syndrome of thrombocytopenia and MAHA, Abbreviations: aHUS: Atypical Hemolytic Uremic Syndrome; CAPS: Catastrophic Anti-Phospholid Antibody Syndrome; DGKE: Diacylglycerol kinase epsilon; DIC: Disseminated Intravascular Coagulopathy; HELLP: Hemolysis, elevated liver enzymes and low platelet; HIT: Heparin Induced Thrombocytopenia; IEL: Internal Elastic Lamina; MMACHC: Methylmalonic Aciduria and Type C Homocystinuria; VWF: Von Willebrand Factor.
These pathological lesions have the common feature of arteriolar stenosis, which generates abnormal shear stress in the microcirculation and causes fragmentation of red blood cells. MAHA is often accompanied with thrombocytopenia because thrombosis is the most common cause of arteriolar stenosis. In metastatic diseases, thrombocytopenia may result from bone marrow involvement or other causes.
In the literature, TTP is often considered a disorder of TMA, which in turn is often equated with the syndrome of thrombocytopenia and MAHA. In fact, the pathology of TTP, characterized with VWF-rich thrombosis in arterioles and capillaries but no apparent evidence of microangiopathy (endothelial injury) (Figure 1, panel A), except for subtle apoptosis [1], is distinct from TMA, which comprises two components: microangiopathy, as evidenced by endothelial cell swelling, necrosis or disruption, and/or subendothelial edema or cellular proliferation; and intraluminal thrombosis of fibrin and platelets (Figure 1, panel B). In TMA, it is believed that endothelial injury is the primary event, while thrombosis occurs secondarily at sites of endothelial cell disruption where platelets and blood coagulation proteins come in contact with exposed subendothelial components.
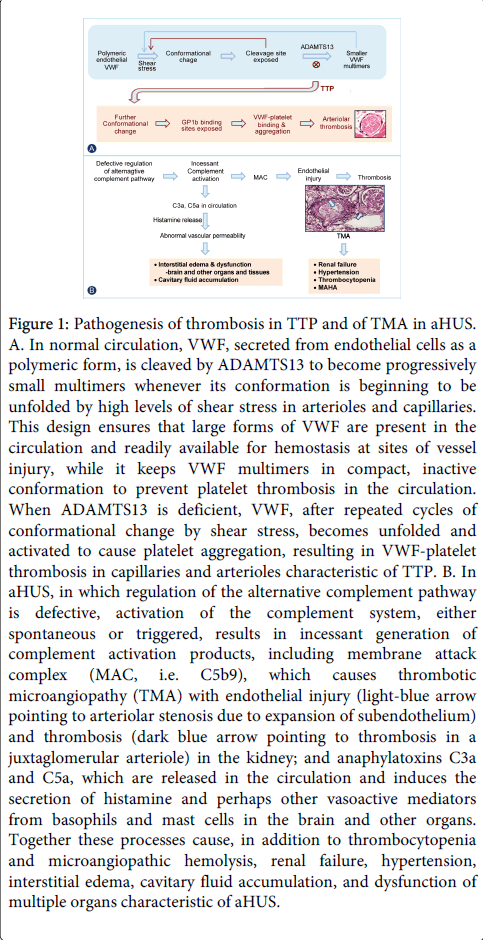
Figure 1: Pathogenesis of thrombosis in TTP and of TMA in aHUS. A. In normal circulation, VWF, secreted from endothelial cells as a polymeric form, is cleaved by ADAMTS13 to become progressively small multimers whenever its conformation is beginning to be unfolded by high levels of shear stress in arterioles and capillaries. This design ensures that large forms of VWF are present in the circulation and readily available for hemostasis at sites of vessel injury, while it keeps VWF multimers in compact, inactive conformation to prevent platelet thrombosis in the circulation. When ADAMTS13 is deficient, VWF, after repeated cycles of conformational change by shear stress, becomes unfolded and activated to cause platelet aggregation, resulting in VWF-platelet thrombosis in capillaries and arterioles characteristic of TTP. B. In aHUS, in which regulation of the alternative complement pathway is defective, activation of the complement system, either spontaneous or triggered, results in incessant generation of complement activation products, including membrane attack complex (MAC, i.e. C5b9), which causes thrombotic microangiopathy (TMA) with endothelial injury (light-blue arrow pointing to arteriolar stenosis due to expansion of subendothelium) and thrombosis (dark blue arrow pointing to thrombosis in a juxtaglomerular arteriole) in the kidney; and anaphylatoxins C3a and C5a, which are released in the circulation and induces the secretion of histamine and perhaps other vasoactive mediators from basophils and mast cells in the brain and other organs. Together these processes cause, in addition to thrombocytopenia and microangiopathic hemolysis, renal failure, hypertension, interstitial edema, cavitary fluid accumulation, and dysfunction of multiple organs characteristic of aHUS.
While arteriolar thrombosis of VWF and platelets is found only in TTP, the pathology of TMA may result from at least seven different mechanisms of endothelial injury (Table 1). The best known is shiga toxin associated hemolytic uremic syndrome (stx-HUS), in which shiga toxins produced by certain strains of E. coli or other microorganisms cause endothelial cytotoxicity. TMA can also occur in patients with pneumococcal sepsis and other infections in which microbial neuraminidases expose the Thomsen-Friedenreich (TF)-antigen on endothelial cells, subjecting the cells to attack by pre-existing antibodies against the antigen [2,3]. TMA can occur with anti-vascular endothelial growth factor (VEGF) drugs such as bevacizumab, a humanized monoclonal antibody of VEGF [4]. Anti-VEGF therapy deprives VEGF signaling in glomerular endothelial cells, resulting in glomerular microangiopathy and occasionally thrombosis. TMA is also known to occur in association with a variety of other drugs such as mitomycin, gemcitabine, calcineurin inhibitors, quinine and cocaine, via as yet unknown mechanisms.
In patients without infections or drugs (i.e. idiopathic cases), three groups of molecular defects have been detected in association with TMA: mutations or antibodies of complement factor H, membrane cofactor protein, complement factor I, complement factor B, C3, or thrombomodulin that affect the regulation of complement activation [5]; mutations of diacylglycerol kinase epsilon (DGKE) that causes the accumulation of arachidonoyl diacylglycerol and consequent activation of protein kinase C, resulting in endothelial activation, apoptosis, and down-regulation of the expression of VEGF receptor 2 and podocyte nephrin [6-8]; and mutations of methylmalonic aciduria and homocysteinuria type C (MMACHC) gene (i.e. cobalamine C disease) [9-12], in which endothelial injury presumably is a consequence of high plasma levels of homocysteine. Atypical hemolytic uremic syndrome (aHUS) with mutations or antibodies causing defective regulation of the alternative complement pathway is the most common cause of idiopathic TMA and is the subject of a recent review [5].
Other types of pathology that may be associated with the syndrome of thrombocytopenia and MAHA include fibrin thrombosis that is typical of disseminated intravascular coagulopathy but occasionally occurs in patients with catatrophic antiphospholipid antibody syndrome, heparin induced thrombocytopenia, paroxysmal nocturnal hemoglobinurial, or the syndrome of hemolysis, elevated liver enzymes and low platelet counts (HELLP) of pregnancy; and vasculitis/vasculopathy; and intravascular clusters of neoplastic cells. These entities are distinct from but are often referred to indiscriminately in the literature as ‘TMA’.
The pathology of the HELLP syndrome of pregnancy, defined as a constellation of hemolysis, often with schistocytes, elevated liver transaminases, and low platelet counts, is characterized by foci of hemorrhage, subcapsular hematoma, peri-sinusoidal hepatocellular necrosis and extensive fibrin network in liver parenchyma in the liver [13]. As will be further elaborated later, the HELLP syndrome, as well as preeclampsia, may transition to aHUS in women with underlying defects in the regulation of the alternative complement pathway. Consequently, extra-hepatic findings often attributed to the HELLP syndrome or preeclampsia may in fact be the consequence of aHUS.
Vasculitis and vasculopathy are distinct from the pathology of TTP and TMA in that they affect the internal elastic lamina and deeper layers of the vascular wall. Fibrinoid necrosis may be observed in acute lesions. Vasculitis, which may be autoimmune (e.g. lupus erythematosus) or infectious (e.g. Rickettsia rickettsii) in nature, is distinguished from vasculopathy by the presence of infiltration of inflammatory cells. In milder cases, a distinction between vasculopathy and TMA may not be straightforward.
Thus, the pathology of TTP is different from TMA. In addition to TTP and TMA, there are other types of pathology associated with the syndrome of thrombocytopenia and MAHA. On the other hand, while most cases of TTP present with thrombocytopenia and MAHA, TTP may occasionally present with stroke or transient ischemic attack without apparent thrombocytopenia or MAHA [14,15]. MAHA and thrombocytopenia are apparent only when thrombosis and arteriolar stenosis are extensive to cause notable thrombocytopenia and red cell fragmentation. Similarly, it is not uncommon to encounter cases with TMA in kidney biopsy performed for renal dysfunction, yet without MAHA or thrombocytopenia in the peripheral blood.
A syndrome-based diagnosis cannot reliably distinguish TTP from aHUS and the other causes of MAHA and thrombocytopenia. With the discovery of ADAMTS13 and its inhibitors in patients with acquired TTP and genetic mutations in patients with hereditary TTP, TTP is now mechanistically defined as a disease with a propensity to arteriolar thrombosis due to genetic mutations or autoimmune inhibitors of ADAMTS13 (Table 2). Similarly, aHUS, instead of being defined as a syndrome of renal failure, MAHA and thrombopcytopenia, is re-defined as a disorder with a propensity to TMA due to defective regulation of the alternative complement pathway. The mechanism-based definitions encompass patients presenting with incomplete features and provide a clear distinction of TTP from aHUS, which are otherwise often lumped together as TTP/HUS.
| Disorder | Clinical state |
| TTP A Propensity to arteriolar and capillary thrombosis due to ADAMTS13 deficiency, resulting from Genetic mutations, or Inhibitory antibodies |
Active thrombosis (ADAMTS13 is <10% of normal) Diad, triad, or pentad (conventional TTP) Thrombocytopenia (often mistaken to be ITP) Stroke, TIA or MI ± thrombocytopenia Thrombocytosis and MAHA Normal platelet count and no MAHA (plasma infusion increases the platelet count) Clinical remission (ADAMTS13 is normal or decreased, even <10%) Normal platelet count and no MAHA No symptoms of vascular insufficiency |
| Atypical HUS A propensity to thrombotic microangiopathy due to defective regulation of the alternative complement pathway, resulting from deficient regulators or hyperactive activators Loss of function mutations of regulators Complement factor H Membrane cofactor protein Complement factor I Thrombomodulin Antibodies of CFH Gain of function mutations of activators Complement factor B C3 Undetected genetic alternations |
Active Renal failure, MAHA and thrombocytopenia Renal failure and MAHA Renal failure, progressive or end-stage Hypertension, ± MAHA, ±renal failure Inactive (clinical remission) Normal platelet count and no or resolving MAHA Stable or resolving renal dysfunction No extra-renal comlications |
Table 2: Mechanistic definitions of TTP and aHUS, Abbreviations: CFH: Complement Factor H; ITP: Idiopathic Thrombocytopenic Purpura; MAHA: Microangiopathic Hemolytic Anemia; MI: Myocardial Infarction; TIA: Transient Ischemic Attack.
Serial investigation of TTP patients at acute presentation, during the course of plasma exchange therapy and in clinical remission show that the plasma ADAMTS13 activity is invariably less than 10% of normal when there is evidence of active thrombosis such as thrombocytopenia or decreasing platelet counts. On the other hand, among patients with TTP in clinical remission (i.e. no active thrombosis) the ADAMTS13 activity may be normal or decreased, even less than 10% of normal in some cases. A plasma ADAMTS13 activity <10% (or 5%, depending on the assays) is not necessarily associated with active thrombosis, as the threshold of thrombosis is variable, being affected by multiple factors such as the shear stress profile of the circulation, VWF secretion from endothelial cells, platelet count and reactivity, plasma thrombospondin [16] and other poorly understood factors. However, such patients are at risk of thrombotic complications either spontaneously or in association with infection, fever, dehydration, surgery, trauma, or pregnancy that further decreases the plasma ADAMTS13 activity, increases VWF secretion from endothelial cells, or augments the shear stress profile in the circulation.
ADAMTS13 cleaves VWF whenever it is beginning to be conformationally altered by shear stress in the circulation (Figure 1, panel A). By cleaving VWF before it is fully activated by shear stress, ADAMTS13 prevents VWF-platelet binding and intravascular thrombosis. When ADAMTS13 is severely deficient, VWF is activated by shear stress in the circulation to cause thrombosis in the arterioles and capillaries, where physiologic shear stress is at its highest. For comparison, a scheme of the steps leading to renal failure and other organ dysfunction of aHUS is also depicted (Figure 1, panel B).
The scheme of ADAMTS13 deficiency causing VWF-platelet thrombosis in TTP is based on the findings of in-vitro experiments, the detection of ADAMTS13 deficiency due to inhibitory antibodies in acquired TTP, and the linkage of hereditary TTP to ADAMTS13 mutations [17,18]. The scheme is further supported by two types of animal models: a murine model with homozygous ADAMTS13 gene inactivation and a baboon model given an inhibitory monoclonal antibody of ADAMTS13 [19-22]. Both models confirm that ADAMTS13 deficiency creates a propensity to arteriolar and capillary VWF-platelet thrombosis of TTP. The mouse model also highlights the heterogeneity of various murine strains in their responses to ADAMTS13 deficiency.
This definition of TTP focuses on whether a patient has ADAMTS13 deficiency rather than on the presence of MAHA or thrombocytopenia. Therefore it not only includes patients who present with the conventional diad, triad, or pentad; but also the less common and less well known groups of patients such as those presenting with thrombocytopenia alone and are often mistaken to have idiopathic thrombocytopenic purpura (ITP); patients presenting with strokes, transient ischemic attacks or myocardial infarction, with or without thrombocytopenia but without MAHA [14,15], patients presenting with thrombocytosis (presumably due to overcompensating thrombocytopoiesis) [23], and those with subclinical platelet consumption whose disease activity, as first described by Schulman and Upshaw [24,25], is only revealed when plasma or blood transfusion, by raising circulating ADAMTS13 activity levels, leads to an increase in the platelet count.
One of the main lessons learned from the new definition of TTP is that the disorder does not cause advanced renal failure [26]. Similar findings are also observed in other recent series [27,28]. At autopsy of patients died of TTP, examination of the kidney typically shows foci of glomerular and arteriolar thrombosis; yet extensive thrombosis with destruction of the renal architecture is not observed. Therefore, when a patient with acquired TTP also has renal failure, it should not be attributed to TTP; the physician is obligated to search for other causes to account for the renal failure.
In vitro, it is estimated that the critical level of shear stress for activation of VWF is in the range of 90 dynes/cm2 [29]. The relatively low levels of shear stress (23 ± 25 dynes/cm2) in renal glomeruli [30], and the potential protection provided by locally secreted ADAMTS13 [31] before it is neutralized by circulating inhibitors, may explain why renal thrombosis is not extensive in TTP.
Among more than 200 cases of acquired TTP in the author’s records [26], only three patients had renal failure with maximal serum creatinine greater than 2.5 mg/dL, all with a cause: one with anti-GBM nephropathy that was only diagnosed in retrospect when the patient presented during remission of TTP with a relapse of renal failure unaccompanied with thrombocytopenia, MAHA or ADAMTS13 deficiency [32]; one case immediately after a renal allograft transplantation; [33]; and one case with atypical hemolytic uremic syndrome [34]. In the literature, two cases of TTP with renal failure also had concurrent stx-HUS [35,36].
Renal failure with serum creatinine levels >2.5 mg/dL is observed in up to 47% of a series of patients with ticlopidine-associated TTP [37]. However, many of the patients had intravenous contrast media immediately prior to the onset of TTP or co-morbid conditions that may amplify the severity of renal function impairment in association with TTP.
In contrast to acquired TTP, advanced renal failure is not uncommon in patients with hereditary TTP. In our series of hereditary TTP who were not receiving maintenance plasma therapy, 20% of the patients had at least one episode of acute renal failure with maximal serum creatinine greater than 2.5 mg/dL and 12% of the patients had chronic renal insufficiency [38]. Lack of protection by locally expressed ADAMTS13 and cumulative effect of long-term repetitive insults may be the reasons that renal failure can be severe in patients with hereditary TTP.
A good example of how the new mechanistic definitions of TTP and aHUS help unravel complex cases is illustrated in a patient of TTP who was resistant to plasma exchange therapy but improved with eculizumab, a humanized monoclonal anti-C5 that is approved for the treatment of aHUS [39]. When thrombocytopenia relapsed after both plasma exchange and eculizumab were discontinued, the patient was treated only with eculizumab and achieved clinical remission. The patient was thought to have TTP because his ADAMTS13 activity level was very low (<5%) at presentation and at relapse, and the ADAMTS13 inhibitor test was positive on both occasions. The report of this case raised high hopes among many hematologists that anti-complement therapy with eculizumab may provide an effective rescue treatment for TTP that is unresponsive to plasma exchange therapy and other current second-line therapies.
However, the patient’s maximal serum creatinine level was greater than 2.5 mg/dL during the course, indicating that this was not an uncomplicated case of TTP. Re-analysis of the patient’s plasma samples revealed that although his plasma ADAMTS13 activity was decreased (14%) and his ADAMTS13 inhibitor test was positive, the plasma ADAMTS13 activity was not sufficiently low to cause the relapse of thrombocytopenia [34]. Further investigation revealed that the patient had antibodies of complement factor H (CFH) when he had relapse of thrombocytopenia (no sample from the time of presentation was available for study.) During follow-up, his CFH antibody test remained positive and the patient continued to require eculizumab to control his symptoms, although his plasma ADAMTS13 activity had increased to 103%. Therefore, although the patient did have acquired TTP with inhibitory ADAMTS13 antibodies, his clinical complications were due to aHUS rather than TTP. This explains why he responded to eculizumab but not to plasma exchange therapy.
This case illustrates the importance of not attributing advanced renal failure to TTP in a patient with the disease. Acquired TTP and aHUS, both autoimmune in nature, can co-exist in the same patient. However, these two disorders evolve independently, suggesting that the B-cell clones producing ADAMTS13 inhibitors and CFH antibodies are under separate regulations.
A case of hereditary TTP with renal failure due to concurrent atypical hemolytic uremic syndrome of complement factor H mutations has also been described [40].
A variety of disorders such as autoimmune disorders, hematopoietic stem cell therapy, HIV infection and pregnancy are known to be associated with the syndrome thrombocytopenia and MAHA, which are often represented in the literature as, TTP/HUS or ‘TMA’ in their various forms of definitions. The mechanisms of this association are complex. Each disorder needs to be evaluated individually in four types of pathogenetic contributions: a trigger of VWF-platelet thrombosis in patients with pre-existing TTP or TMA in patients with pre-existing aHUS; defective regulation of the immune system with the emergence of B-cell clones producing ADAMTS13 inhibitors (TTP) or CFH antibodies (aHUS); a cause of TMA via mechanisms other than defective complement regulation; and a cause of other types of pathology (fibrin-platelet thrombosis, vasculitis/vasculopathy or intravascular clusters of neoplastic cells) (Table 3).
| Co-morbidity | Disorder or pathology | Mechanism | |
| Infection, inflammation Surgery, trauma, vascular catheters |
TTP | Trigger of thrombosis in patients with pre-existing TTP | |
| aHUS | Trigger of complement activation in patients with pre-existing aHUS | ||
| Pregnancy | HELLP syndrome | Unknown | |
| TTP | Trigger of platelet thrombosis in patients with pre-existing TTP ADAMTS13 inhibitorsdue to postpartum immune dysregulation |
||
| aHUS | Trigger of complement activation in patients with pre-existingaHUS, with or without preceding HELLP or preeclampsia CFH Ab due to postpartum immune dysregulation |
||
| HSCT | TTP | Trigger of thrombosis in patients with pre-existing TTP ADAMTS13 inhibitors due to immune dysregulation |
|
| TMA | Trigger of complement activation in patients with pre-existingaHUS CFH Ab due to immune dysregulation Endothelial injury by myeloablative regimens Endothelial injury by calcineurin or mTOR inhibitors |
||
| Infectious vasculitis | Viremia or fungemia associated with immunodeficiency | ||
| Autoimmune disorders | Lupus Still’s disease Anti-GBM |
TTP | Trigger of platelet thrombosis in patients with TTP ADAMTS13 inhibitors due to immune dysregulation |
| Lupus | aHUS | Trigger of complement activation in patients with aHUS CFH Ab due to immune dysregulation |
|
| Lupus Scleroderma |
Vasculitis Vasculopathy |
Autoimmunity targeting vessel wall components | |
| CAPS | Fibrin-platelet thrombosis | Activation of the platelet-coagulation system | |
| Renal transplantation | TMA | Trigger of complement activation in patients with pre-existing aHUS Endothelial injury by calcineurin or mTOR inhibitors |
|
| Infectious vasculitis | Fungemia or viremia associated with immunodeficiency | ||
| Hypertension | A consequence of TMA or vasculopathy | Dysregulation of renin secretion due to TMA or vasculopathy affecting the juxtaglomerular arterioles | |
| Drugs | Ticlopidine | TTP | Induction of ADAMTS13 inhibitors |
| RCM | aHUS | Trigger of complement activation in patients with pre-existing aHUS | |
| Other drugs | TMA | Deprivation of VEGF signaling (e.g. bevacizumab) Other mechanisms (e.g. gemcitabine, mitomycine, cocaine, etc.) |
|
| HIV infection | TTP | ADAMTS13 inhibitors due immune dysregulation | |
| TMA | Presumably CFHantibodies due to immune dysregulation | ||
| Neoplasms | TMA | Endothelial injury by chemotherapeutic drugs | |
| Intravascular tumor cells | Intravascular invasion of neoplasm (‘tumor cell embolism’) | ||
Table 3: Potential mechanisms of MAHA and thrombocytopenia in patients with various co-morbid conditions, Abbreviations: CAPS: Catastrophic Antiphospholipid Antibody Syndrome; CFH: Complement Factor H; HELLP: Hemolysis, Elevated Liver Enzymes And Low Platelet; HSCT: Hematopoietic Stem Cell Therapy; MAHA: Microangiopathic Hemolytic Anemia; mTOR: Mammalian Target Of Rapamycine; RCM: Intravenous Contrast Media; TMA: Thrombotic Microangiopathy
Surgery, trauma and various infections
These conditions may trigger the complications of TTP in patients with ADAMTS13 inhibitors or mutations by releasing VWF from endothelial cells, increasing the shear stress profile in the circulation, or further decreasing the plasma ADAMTS13 activity. These conditions, radiographic contrast media, or vascular catheters may also trigger complement activation and the development of TMA in patients with defects in regulating complement activation (aHUS).
Pregnancy
The HELLP syndrome, affecting about 0.2% to 0.6% of all pregnancies, is the most common cause of the syndrome of thrombocytopenia and MAHA during pregnancy.
Pregnancy increases the plasma ADAMTS13 level and decreases the plasma ADAMTS13 activity [41]. Consequently, it is not surprising that pregnancy may trigger the onset of VWF-platelet thrombosis in patients with hereditary TTP [42]. Such triggering occurs less frequently in women with a history of acquired TTP, presumably because pregnancy often ameliorates autoimmunity.
Activation of the complement system often occurs during pregnancy, more intensely when it is complicated with the HELLP syndrome or preeclampsia [43-45]. Complement activation may trigger the development of TMA in pregnant women with pre-existing genetic defects in the regulation of the alternative complement pathway. Further complicating the distinction between aHUS and preeclampsia or the HELPP syndrome, some patients initially present with the HELLP syndrome or preeclampsia but then transition to aHUS. This transition occurs because the HELLP syndrome or preeclampsia causes intense complement activation, thereby triggering the complications of TMA in patients who have mild defects in complement regulation. Because of the possibility of this transition, patients with the diagnosis of HELLP or preeclampsia should be carefully monitored for the development of aHUS complications such as renal failure, hypertension, interstitial edema of the brain and other organs, and fluid accumulations in the pericardial, pleural or peritoneal spaces. In practice, it is not uncommon to encounter women given the hybrid diagnosis of ‘HELLP/preeclampsia’ or ‘TTP/HUS’ for their aHUS. The misdiagnosis of aHUS as HELPP/preeclampsia likely explains why mutations of complement regulators are detected in greater than 10% of the women with a history of ‘HELLP’ and/or ‘preeclampsia’ [46].
Regulation of the immune system is often defective during the postpartum period. Inhibitors of ADAMTS13 or antibodies of CFH may occasionally occur during the postpartum period, analogous to the development of factor VIII inhibitors that is widely known to occur after delivery.
Hematopoietic stem cell therapy (HSCT)
MAHA after HSCT is heterogeneous in its time of onset, severity and the responsiveness to plasma therapy. Mechanistically, the patients presenting with thrombocytopenia and MAHA may be divided in four groups. In group 1, the extensive cell and tissue injury or infection in association with myeloablation may trigger the onset of VWF-platelet thrombosis in patients with pre-existing TTP or of TMA in patients with pre-existing aHUS [47]. Such coincidental TTP or aHUS can occur but are uncommon.
In group 2 of patients, defective regulation of the immune system following myeloablation or discontinuation of immunosuppressive therapy may allow auto-reactive B-cell clones to emerge during immune recovery to produce inhibitors of ADAMTS13 or antibodies of CFH. This type of acquired TTP or aHUS due to immune dysregulation is more likely to occur in patients of autologous stem cell therapy that do not require anti-graft versus host disease (GVHD) therapy or patients of related matched HSCT after anti-GVH therapy is discontinued [18,47]. Rituximab may be an effective therapy by suppressing ADAMTS13 inhibitors or CFH antibodies in these patients. Nevertheless, the suppression may be incomplete and does not last.
In group 3 of patients, there is no evidence of ADAMTS13 deficiency or defective complement regulation. Some myeloablative regimens are associated with high risk of endothelial injury, although the risk appears to be quite low at most centers with most commonly used regimens [48-50]. Calcineurin inhibitors and other drugs for GVHD may cause endothelial injury and TMA, resulting in MAHA and thrombocytopenia. This type of complication often occurs when immunosuppressive treatment is being intensified for active GVHD. Revising the anti-GVHD regimen often ameliorates the severity of TMA in these patients.
In group 4 of patients, thrombocytopenia and TMA are a consequence of infectious vasculitis due to viremia or fungemia. Viremia or fungemia may cause endothelial injury, often with direct endothelial infection in patients who are immunocompromised. Control of infection may lead to clinical improvement.
Lupus and other autoimmune disorders
TTP with ADAMTS13 inhibitors occasionally occurs, albeit quite uncommonly, in patients with lupus [17], anti-glomerular basement membrane (GBM) nephropathy [32], or adult-onset Still’s disease [51]. As described in an earlier section, TTP is also found to occur in a patient with autoantibodies of CFH [34]. In the case of anti-GBM nephropathy, the patient presented with TTP and renal failure. The correct diagnosis of concurrent anti-GBM nephropathy was made in retrospect only after the patient presented 10 months after his TTP presentation with renal failure unaccompanied with MAHA, thrombocytopenia or ADAMTS13 deficiency. In patients with autoimmune disorders, it is presumed that deranged regulation of autoimmunity predisposes the patients to the development of ADAMTS13 inhibitors. In these patients, TTP and the other autoimmune processes evolve independently [18].
TMA in patients with lupus or autoimmune disorders is assumed to be a consequence of aHUS. In fact, molecular defects in complement regulation have been described in the some lupus patients presenting with the syndrome of MAHA, thrombocytopenia and renal failure [52]. In these patients, inflammation and immune complexes of autoimmune disorders may trigger TMA by activating the complement system of patients with pre-existing aHUS.
Vasculitis of the immune complex variant is the most common type of pathology in lupus patients presenting with the syndrome of thrombocytopenia and MAHA. In patients with scleroderma, vasculopathy affecting arterioles is the most common finding. Patients with catastrophic antibody syndrome (CAPS) may occasionally present with MAHA and thrombocytopenia in association with arteriolar fibrin-platelet thrombosis.
Solid organ transplantation
Patients presenting with MAHA after renal transplantation belong to two groups: those with un-diagnosed aHUS as the cause of their pre-transplant renal failure, and those with complications of endothelial injury due to immunosuppressive therapy or vasculitis/vasculopathy due to viremic/fungemic infections.
In patients with undiagnosed aHUS, complications of TMA and thrombocytopenia often occur soon after the transplantation operation, which acts as a trigger of complement activation in patients with aHUS. With the exception of MCP mutations, kidney transplantation in patients with unrecognized aHUS is associated with a very high risk of recurrent TMA in the grafts [53], with or without thrombocytopenia and MAHA. Anti-complement therapy is effective in preventing aHUS and graft failure for this group of patients.
The MAHA after other solid organ transplantations are due to the adverse effects of immunosuppressive drugs or severe viremic or fungemic infections. Occasionally, intense rejection reaction may cause vasculitis and MAHA.
Hypertension
Conventionally hypertension is thought to be a cause of MAHA or TMA. However, some patients of aHUS may present with brittle hypertension, accompanied with no or minimal MAHA, thrombocytopenia or renal dysfunction, weeks to years before their diagnosis of aHUS was suspected and established. Indeed, defective regulation of the alternative complement system has been detected in patients with the diagnosis of ‘malignant hypertension’ [54]. Additionally, severe hypertension is a common complication in patients with TMA due to stx-HUS, drug-associated TMA or renal scleroderma vasculopathy.
Thus, in patients without scleroderma, drug or infection-related HUS, aHUS should be suspected, particularly when hypertension is brittle or accompanied with extra-renal complications of abnormal vascular permeability [18].
Drugs
Ticlopidine increases the risk of TTP by 50 to 300 fold [55,56]. Previous suspicion of an association between clopidogrel and TTP was not substantiated upon further investigation. aHUS is a more likely diagnosis in most of the patients [37]. Many of the patients had received radiographic contrast media during cardiac catheterization or other imaging studies. Intravenous contrast agents, potent triggers of complement activation [57], may cause the development of TMA in patients with pre-existing aHUS.
Anti-VEGF drugs such as bevacizumab may cause endothelial injury and TMA by depriving the VEGF signaling [4]. Other drugs such as gemcitabine, mitomycin and calcineurin inhibitors cause endothelial injury via un-determined mechanisms. Anti-complement therapy with eculizumab is ineffective for gemcitabine associated TMA (personal unpublished data).
HIV infection
In patients with HIV infection, TTP accounts for approximately 75% of the cases presenting with the syndrome of thrombocytopenia. The other patients often have prominent renal failure and are assumed to have aHUS. Occasionally HIV patients have the myelodysplastic syndrome in which some of the poikilocytes may be mistaken to be schistocytes.
When not being treated with anti-retroviral therapy, HIV infection increases the risk of TTP due to ADAMTS13 inhibitors by nearly 40 folds [26]. HIV infection is known to be associated with various autoimmune phenomena or disorders. Therefore, it is conceivable that HIV infection may also induce autoimmunity to either ADAMTS13 or CFH, resulting in acquired TTP or aHUS.
Cancers
The syndrome of MAHA and thrombocytopenia in patients with neoplastic disease may result from chemotherapeutic drug-associated TMA, aHUS, or intravascular invasion of neoplastic cells (‘cancer cell embolism’). TTP may occur, albeit quite infrequently.
Plasma exchange remains the mainstay of therapy for TTP. Plasma therapy prevents death by replenishing the missing ADAMTS13 protease; however, it does not alter the natural course of the ADAMTS13 inhibitors. Clinical remission of TTP is a consequence of spontaneous abatement of ADAMTS13 inhibitors.
With plasma therapy, the median duration of relapse-free survival is only 3.2 months after achieving clinical remission, defined as two consecutive normal platelet counts [26]. Serial analysis shows that the plasma ADAMTS13 activity and inhibitor levels are often quite unstable for weeks before they gradually settle at a steady state range that may be normal or decreased, even less than 10% in approximately 10% of the cases. The fluctuation explains why clinical remission is often un-sustained during the first few months.
When relapses within the first month, which some consider arguably to represent exacerbation instead of relapse, are excluded, the median duration of relapse-free survival is 9.4 months. Indeed, long-term follow-up data shows that after 7-8 years, approximately 90% of the patients will have at least one relapse [26]. Therefore, TTP is a chronic autoimmune disease that is bound to relapse in most patients after its initial presentation.
Rituximab was first used for acquired TTP to suppress ADAMTS13 inhibitors in patients who were unable to wean off plasma exchange therapy [15,23,58,59]. The treatment has been highly effective, allowing 70% - 90% of the patients to come off plasma exchange. With this success, attention is turn to the use of rituximab for prevention of relapses.
Two studies have investigated the efficacy of early, preemptive rituximab therapy in altering the course of TTP [27,28,60]. In one study, by Scully et al. and extended by Westwood et al, rituximab therapy is initiated soon after the diagnosis of rituximab. This study shows that rituximab initiated within 3 days of diagnosis may decrease the number of plasma exchange sessions (median from 24 to 16, P=0.03) and the numbers of days to remission (median from 20 to12, P<0.001). Since the study is a retrospective analysis, one cannot exclude unintended biases. Indeed, of our 39 consecutive non-referral cases [26], the median number (13, range 3-42) of plasma exchange sessions is not different from the rituximab treated group of Westwood et al, although none of the patients in our series received rituximab therapy.
This lack of benefit with early rituximab therapy is not surprising, because that the effect of rituximab often takes more than 2 weeks to occur. On the other hand rituximab therapy is effective in prolonging the duration of remission, increasing the median duration to 31.23 months from 9.4 months in the untreated group [26]. Nevertheless, rituximab therapy does not eliminate the risk of relapses.
Serial monitoring of plasma ADAMTS13 activity during remission reveals that ADAMTS13 gradually decreases in a zig-zag manner over the course of several weeks to months before a clinical relapse occurs. This period of gradual decrease in plasma ADAMTS13 activity provides a window for intervention with preemptive rituximab therapy.
The following protocol of repeated courses of preemptive rituximab therapy guided with the levels of plasma ADAMTS13 activity are thus designed to prevent relapses and obviate the need of plasma exchange therapy.
The ADAMTS13 activity is checked at remission and at least weekly when plasma therapy is being tapered, in additional to CBC daily or every other day.
A course of rituximab is indicated if the ADAMTS13 activity is less than 10% of normal when the patient is achieving clinical remission. This intervention decreases the risk of early relapse and raises the plasma ADAMTS13 level for subsequent monitoring. Since ADAMTS13 assay results are often not available for 1-2 weeks, in practice the threshold level for rituximab therapy is set to 20-30% or higher. This provides the time for rituximab therapy to make its effect before relapses occur.
Plasma ADAMTS13 is checked before each dose of rituximab. If the ADAMTS13 level is normalized following rituximab therapy, the risk of relapse within six months is miniscule. After rituximab therapy plasma ADAMTS13 activity is monitored monthly. Plasma ADAMTS13 activity often begins to show a trend of decrease after 2±1 years.
A preemptive course of rituximab is administered when the ADAMTS13 again decreases to 20% - 30% of normal. Monitoring should continue after each course of rituximab therapy.Using this strategy of ADAMTS13-guided rituximab therapy, a patient who had 11 episodes of relapses requiring plasma exchange therapy over the course of 12 years has remained free of relapse for nearly 5 years (Figure 2).
The course of plasma ADAMTS13 activity shows that preemptive rituximab likely prevents two episodes of clinical relapses that would have required plasma exchange therapy. Another patient with 3 relapses within a year has been free of relapses for nearly 3 years (data not shown). Thus, with ADAMTS13-guided rituximab therapy, it is feasible to prevent the relapses of TTP and obviate the need of repeated courses of plasma exchange therapy, which is invasive, uncomfortable and not infrequently associated with infection or other serious complications. Rituximab treatment carries minimal adverse effects and is obviously superior to the alternative, which is either monitoring of the platelet counts that does not obviate the need of plasma exchange, or a blindly fixed schedule of rituximab therapy.
It is now widely recognized that acquired TTP is an autoimmune disorder with inhibitory antibodies of ADAMTS13. The mechanistic definition of TTP, along with that of aHUS, provides the basis for a rational approach to the differential diagnosis of various clinical conditions that are associated with the syndrome of thrombocytopenia and MAHA. New insights also provide the basis for a strategy of ADAMTS13-guided preemptive rituximab therapy to prevent relapses in patients with acquired TTP. Preliminary data shows that this strategy can prevent relapses of acquired TTP and obviate the need of repeated courses of plasma therapy. Further investigation is necessary to fully delineate the efficacy of this strategy.
Another potential approach to address the problem of relapse is the development of truncated ADAMTS13 variants that are not suppressible by the inhibitors of TTP patients [61]. With such non-suppressible ADAMTS13 variants, it may be possible to raise plasma ADAMTS13 activity immediately and predictably irrespective of the ADAMTS13 inhibitor levels. Furthermore, intermittent administration of such proteases should be as effective as is presently achieved with periodic plasma infusion for patients with hereditary TTP. ADAMTS13 variants with amino acid substitutions at the residues Arg660, Tyr661, or Tyr665 of the spacer domain are also non-suppressible by TTP inhibitors [62]. However, concerns of immunogenicity with rADAMTS13 variants will need to be addressed before further development of this approach can be pursued.
Some of the works described in this article were performed with the supported of a grant (R01 HL062136) from the National Heart Lung and Blood Institute of the National Institutes of Health, USA.
The author does not have conflicts of interest to declare in preparing this manuscript. He did receive honorarium from Alexion Canada for lectures.