Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Review Article - (2014) Volume 2, Issue 6
Patients undergoing cardiac surgery with cardiopulmonary bypass are at risk of increased blood loss and transfusion requirements. Contact of blood with the surgical wound and the artificial surfaces of the extra-corporeal circuit results in a coagulopathy. Haemodilution during cardiopulmonary bypass also aggravates the reduction of haemostatic factors even further. On the other hand, systemic anticoagulation using high dose unfractionated heparin challenges the adequate anticoagulant monitoring. The most frequently used test to monitor systemic anticoagulation is the whole blood activated clotting time. This has, however, proven not be a reliable test. Other haemostatic assays have their own advantages and disadvantages, but tools to monitor anticoagulation and haemostasis adequately during and after cardiopulmonary bypass are to date lacking and/or show only a weak association with clinical bleeding. Viscoelastic whole blood techniques (TEG/ROTEM) have emerged as alternatives to the routine coagulation tests, and could be more suitable for providing information about the different phases of the blood clotting. Platelet function tests give more information about the presence of platelet dysfunction one, which is a major cause of bleeding after cardiac surgery. Likewise, thrombin generation tests reflect much, if not all, of the overall function of the blood clotting system. Further research of the applicability and added values of the viscoelastic whole blood tests and the thrombin generation tests in the cardiac surgical patient undergoing cardiopulmonary bypass is warranted. Simplicity in performing the test, preferably point-of-care, and rapid availability of the results, should thereby be the primary focus for targeted haemostatic interventions.
Keywords: Cardiopulmonary Bypass; Anticoagulation Monitoring; Blood Loss; Transfusion Requirements; Activated Clotting Time; Thromboelastometry; Platelet Function; Calibrated Automated Thrombography
ACT: Activated Clotting Time; ETP: Endogenous Thrombin Potential; aPTT: Activated Partial Thromboplastin Time; MCF: Maximum Clot Firmness; AT: Antithrombin; PT: Prothrombin Time; CAT: Calibrated Automated Thrombography; ROTEM: Rotational Thromboelastometry; CFT: Clot Formation Time; TEG: Thromboelastography; CPB: Cardiopulmonary Bypass; TFPI: Tissue Factor Pathway Inhibitor; CT: Clotting Time; TG: Thrombin Generation
During cardiopulmonary bypass (CPB) for cardiac surgery, contact of blood with the surgical wound and the artificial surfaces of the extra-corporeal circuit leads to haemostatic disturbances and triggers an angry defense reaction [1,2]. The resulting coagulopathy is caused by several factors: platelet dysfunction, low preoperative fibrinogen levels, hyperfibrinolysis, and continually produced thrombin [3-5]. In addition, haemodilution plays an important role. Patients undergoing CPB procedures are usually infused with crystalloids or colloids, used as pump prime and intra-venous fluids. These infusions lead to a state of dilution coagulopathy while there is a significant fall in clotting factors [3]. Secondly, excessive dilution could lead to an overestimation of the heparin effect, and a resulting overestimation of the required protamine neutralizing dose [6]. All these factors are predictive for an increased risk of excessive perioperative blood loss and subsequent transfusion requirements [7,8]. Other clinical consequences of coagulopathy are: mediastinal re-exploration, postoperative stroke due to hypercoagulability and increased mortality [2,9]. Furthermore, intensive care stay is prolonged and hospital costs are increased [7]. Haemostatic activation seems to be unavoidable in patients undergoing CPB, thereby upsetting their postoperative recovery.
Cardiac surgical patients undergoing CPB are typically anticoagulated using a very high dose of unfractionated heparin. This is the only anticoagulant that brings about an immediate effect and, that can be monitored bedside by a point-of-care test. Moreover, unfractionated heparin is easily neutralized by protamine at the end of the procedure [10]. The primary anticoagulant action of heparin appears to result from its binding with antithrombin (AT). The predominant action of AT is inactivation of factor IIa (thrombin) and factor Xa [11]. Following activation of AT, heparin is released and becomes available for interaction with other AT molecules. In contrast, AT is consumed and AT levels are progressively depleted [11]. Therefore, decreased heparin responsiveness is often attributed to AT deficiency. Besides binding with AT, heparin may bind thrombin directly or act through heparin-cofactor II. Heparin also exerts an anticoagulant effect by augmenting the activity of tissue factor pathway inhibitor (TFPI) [11]. Measuring the real anticoagulant effect of heparin is complicated and thus depends on many variables which determine the patients sensitivity to heparin, such as: 1) the availability of AT; 2) the binding of heparin to proteins (such as albumin and glycosamineglycans) in the bloodstream [12]; 3) the binding of heparin to endothelium [11]; and 4) platelets: both the release of platelet factor 4 and platelets themselves are heparin neutralizing [13].
Several laboratory methods are currently available for monitoring haemostasis and anticoagulation during cardiac surgery. Table 1 shows an overview of available haemostatic tests. Advantages and disadvantages are also listed.
| Test | Clinical indication | Outcome | P/WB | Pros | Cons |
| Clotting times | |||||
| ACT (activated clotting time) | To guide heparinization of CPB patients; to guide heparin neutralization with protamine sulphate as patients come off CPB | Time between activation of FXII by kaolin on the one hand, and the first bit of thrombin and/or fibrin at the other hand. | WB | Point-of-care in operating room; simple, safe, and cost-effective | ACT-based protocols do not avoid thrombin generation during CPB; ACT values during CPB do not correlate with heparin concentrations as a result of hypothermia and haemodilution; return of the ACT to baseline is not an absolute validation of complete heparin neutralization; ACT is technique-dependent |
| aPTT (activated partial thrombo-plastin time) |
To screen overall haemostasis, mainly the intrinsic pathway, to a lesser extent the com-mon pathway; to guide heparin dosing; also used to monitor hirudin, or argatroban |
Time between activation of FXII by kaolin on the one hand, and the first bit of thrombin and/or fibrin at the other hand (intrinsic). | P | Available almost 24 h/day in almost all hospital laboratories; cost-effective | High blood concentrations (over 1 IU/mL) cannot be accurately evaluated by aPTT; does not detect small variations in coagulation factors; not suitable to detect hypercoagulability; Gives only information about a small part of haemostasis |
| PT / INR (prothrombin time / international normalized ratio) |
To screen the integrity of the extrinsic (factor VII) and common (fibrinogen and factors II, V, and X) pathways of coagulation; to monitor warfarin anticoagulation | Time between activation of FVII by tissue factor on the one hand, and first bit of thrombin/fibrin at the other hand (extrinsic). | P | Available almost 24 h/day in almost all hospital laboratories; cost-effective | Does not detect small variations in coagulation factors; not suitable to detect hypercoagulability; Gives only information about a small part of haemostasis |
| Heparin concentration | |||||
| Hepcon HMS | To establish whole blood heparin concen-tration using heparin–protamine titration | Whole blood heparin level | WB | Point-of-care in operating room; simple, safe, and cost-effective | May over-estimate the heparin dose; inability to evaluate the anticoagulant properties of heparin, or to detect heparin resistance. |
| Anti-Xa assay | To monitor heparin therapy; a supplemental means to confirm adequate anticoagulation | Heparin concentration | P | The anti-Xa assay is not susceptible to interference from elevated concen- trations of factor VIII or fibrinogen that result from acute phase reactions; The anti-Xa assay is not influenced by factor deficiencies, with the possible exception of AT deficiency |
The anti-Factor Xa level may be a surrogate mea- surement of the overall anticoagulant activity of unfractionated heparin; An anti-Factor Xa level only assesses how much exogenous factor Xa is inhibited by the patient’s plasma; the presence of a specialized coagulation technologist is necessary |
| Blood factors and platelets | |||||
| Fibrinogen | To measure a haemo-static level (interpreted in the light of other tests like PT/ aPTT) | Fibrinogen level | P | Suggested high predictive value: low fibrinogen levels can be associated with bleeding | Gives only information about a small part of haemostasis; Test is time consuming; High concen- trations of unfractionated heparin (>0.8 IU/ml) may lead to an underestimate of the true fibrinogen level |
| Platelet count | To measure a haemostatic level | Platelet count | WB | Simple, safe, and cost-effective | Only suitable to detect crude abnormalities in haemostasis; not suitable to detect hypercoagulability; provides no information on platelet functionality and thus not highly reflective for bleeding |
| D-dimers | To detect hyperfibrino-lysis / hypercoagulability | D-dimer level | P | High sensitivity | Limited specificity; reflects only break down of fibrin at a specific moment, but does not reflect on-going coagulation activity; data obtained by different D-dimer assays are not interchangeable |
| Platelet function tests | |||||
| Multiplate | To determine platelet function | Platelet function | WB | Studies platelet function within anticoagulated whole blood without any sample processing; is sensitive for the monitoring of platelet function inhibitors; is sensitive for von Willebrand Disease | Highly dependent on platelet number and sample quality; does not simulate physiological primary haemostasis; abnormal results can easily be induced by antibiotics, some vitamins, spices and foods |
| PFA-100 | To detect pharma- cologic platelet dysfunction; may be able to accurately detect hypercoagulability; to identify von Willebrand’s disease, and other acquired and congenital platelet defects | Whole blood platelet function by measuring the closure time (CT) | WB | Simulates in vivo conditions by measuring platelet adhesion and aggregation under conditions of high shear); sensitive for von Willebrand disease and moderate to- severe platelet abnormalities; High negative predictive value; Relatively insensitive to clotting factor deficiencies | Low positive predictive value and thus not very useful in transfusion algorithms to direct transfusion therapy; less sensitive to the effect of anti-platelet medications; Closure times increase progressively with decreases in haematocrit and falls in platelet count below 100 x 109/L |
| Platelet Mapping | To monitor the effect of clopidogrel and aspirin on platelets | Platelet function | WB | It has the potential to evaluate the function of different platelet receptors in the presence of coagulation factors and fibrinogen mimicking conditions |
It is not a true point-of-care instrument as it requires pipetting |
| Visco elastic tests | |||||
| TEG | To assess the global haemostatic function from a single blood sample; allow for diagnosis of hyperfibrinolysis in bleeding patients | Reflections of clotting time, clot strength, degree of fibrinolysis, influence of fibrinogen | WB | Is assessed in whole blood, allowing in vivo coagulation system interactions with platelets and red blood cells; reflects fibrinogen levels; clot development can be visually displayed in real-time; can identify if bleeding is due to residual heparin | Although physiological clot development is better depicted by analysing whole blood, these techniques measure haemostasis under static conditions in vitro, and results must be carefully interpreted; mainly dependent on fibrinogen levels and no information about thrombin generation |
| ROTEM | To assess the global haemostatic function from a single blood sample; allow for diagnosis of hyperfibrinolysis in bleeding patients | Reflections of clotting time, clot strength, degree of fibrinolysis, influence of fibrinogen | WB | Is assessed in whole blood, allowing in vivo interactions with platelets and red blood cells; fibrin-specific clot formation (FIBTEM) can be demonstrated; clot development can be visually displayed in real-time; can identify if bleeding is due to residual heparin | Inability to detect impairment in platelet function induced by anti-platelet agents; although physiological clot development is better depicted by analysing whole blood, these techniques measure haemostasis under static conditions in vitro, and results must be carefully interpreted; mainly dependent on fibrinogen levels and no information about thrombin generation |
| Thrombin generation | |||||
| CAT | To detect bleeding tendency and hypercoagulability; to monitor anticoagulants and procoagulant factors | Amount of thrombin formed by plasma after activation of coagulation in time, reflecting total haemostatic capacity | P/WB | Thrombin generation depends on almost all coagulation factors and anticoagulant proteins; it detects changes in platelet function by changing the sensitivity of the test –and adjust this for the target group-by varying the concentration of added tissue factor. | Lack of clinical and animal studies; not well validated; standardization is necessary before application in laboratories or operation room can take place. |
Table 1: Overview of the tests used for monitoring haemostasis and anticoagulation in cardiopulmonary bypass patients, P= Plasma, WB= whole blood.
Determination of Heparin Concentration
Heparinization is currently monitored by either measuring heparin concentration or by measuring its effect on clotting times. Chromogenic tests for measuring heparin concentration are less sensitive to interfering substances than the clotting tests are. Plasma heparin concentration is determined via its accelerating function in the inhibition of factor Xa or thrombin by AT. Although thrombin based tests are possible, the majority of the commercial heparin assays are performed using anti-factor Xa-activity (anti-Xa), in the haematology laboratory. There are two different designs of the anti-Xa assay. Some tests use a saturating concentration of AT in the reagent. This test determines the ‘total heparin’. The other design does not add AT and relies on the AT in the sample. This determines the AT/heparin complex (or the ‘active heparin’) [14]. Heparin concentration can also be measured bedside by a haemostasis management system (Hepcon HMS, Medtronic, Minneapolis MN). This is a multichannel clot-timing instrument that uses the principle of heparin-protamine titration to quantitatively determine the heparin concentration in whole blood. In each channel, a plastic rod is rapidly lifted and dropped by an oscillating metal bar. Whole blood is automatically placed into each channel by a 3 ml syringe inserted into the machine. The time for blood to clot is displayed for each channel [15]. Six levels of heparin can be determined by using discrete cut offs [16]. Excess protamine inhibits clot formation and insufficient protamine does not fully antagonize heparin, therefore the channel with the fastest clot formation will represent the protamine concentration that optimally neutralizes the existing heparin [17]. The imprecision of the Hepcon HMS could potentially be caused by the effects of release of TFPI by heparin in vivo but not ex vivo. In the absence of an endothelial source of TFPI, the contribution of TFPI to heparin responsiveness may be underestimated by the Hepcon HMS [16]. Heparin concentration monitoring has not uniformly been associated with less bleeding, as it may be associated with heparin rebound postoperatively [17]. Between the anti-Xa assay and the HMS assay there is a lack of agreement [18]. It can be postulated that the HMS assay is affected by factors like haemodilution, hypothermia and platelet dysfunction [18], while the anti-Xa assay only reflects the heparin concentration that inhibits factor Xa. The fraction of heparin that is responsible for anti-factor IIa activity is not measured, meaning that the anti-Xa assay will not give a real and complete reflection of heparin concentration [19]. Thus, monitoring of heparin concentration is only a surrogate for monitoring of anticoagulation, since there are important variations in the response of patients to heparin [20].
Clotting-Time Based Methods
Although routine preoperative coagulation testing contributes little to patient care, this is justified in case of cardiac operations with CPB since patients will undergo an operation with major effects on haemostasis and many will require blood transfusions [21]. Prothrombin time (PT) and activated partial thromboplastin time (aPTT), performed in plasma, are by far the most common screening tests for coagulation abnormalities. These tests correspond respectively to the extrinsic and the intrinsic pathways of coagulation. PT monitoring is widely used as a preoperative screening test for patients receiving oral anticoagulation. The sensitivity for prothrombin and fibrinogen is less pronounced than for other factors. The international normalized ratio (INR) is the ratio of the PT of the patient and the normal PT standardized with the international sensitivity index (ISI). This is to correct for specific laboratory methods. The aPTT is used to guide unfractionated heparin (< 1 IU/ml) clinically. After heparin neutralizing, the aPTT could be measured to control heparin rebound. The PT and aPTT do not reflect the complexity of haemostasis in vivo. One disadvantage of the PT and aPTT is the impossibility to provide information about the interaction with platelets since it is measured in platelet poor plasma. Consequently, these tests will not reflect the extent of bleeding, as platelet count and function may vary [22]. It was clear that even though deficiencies of each of the factors in the intrinsic pathway could have equally long aPTT values, they had dramatically different risks of hemorrhage [23]. Hence the PT and aPTT, providing information on the ability to clot, are poor predictors of bleeding despite their widespread use [24-27]. Another disadvantage is that the PT and aPTT remain normal under hyperfibrinolytic conditions, meaning that bleeding caused by increased fibrin breakdown will not be detected [22]. Although there are many available coagulation assays, it is rather complicated to find the ideal test reflecting the clinical situation of the CPB patient.
During cardiac surgery the prolongation of the clotting time as a reflection of the anticoagulant status is measured. This is performed by the point-of-care activated clotting time (ACT). The principle of the ACT is adding whole blood to a tube containing a contact activator, such as kaolin, celite or silica. Clotting activation and fibrin formation will be initiated and detected. The ACT was first described by Hattersley in 1966 [28], and introduced into cardiac surgery by Bull in the 70’s [29]. The safe minimal level of the ACT was first proposed at 300 s. However, this was stepwise increased to 480 s, after observing visible clots in the extracorporeal circuit and because of a three to six fold variation in heparin effect and a fourfold variation in heparin-life. The most important cofactor that heparin requires for its anticoagulant effect is AT. Therefore, it is surprising that there is no relation between the ACT and AT level [30-32]. In the early 90’s variability between the different systems was noted, i.e. ACT analyzers differ by activators, detection systems, and use different sample volumes [33-35]. Consequently, the ACT value differs for each analyzer, suggesting that extrapolation between different systems would not be appropriate [36]. The ACT is also influenced by factors like the balance of coagulation factors and inhibitors, fibrinogen, platelets, plasma proteins which bind heparin, TFPI release from vasculature, increased haemodilution, and hypothermia of the patient. Nowadays, growing evidence suggests that coagulation is increasingly activated with time during CPB, even with ACT-based protocols [37]. This might lead to a progressive consumptive coagulopathy resulting in a prolonged ACT although heparin levels are decreased, resulting in an incorrect estimation of the anticoagulation status [38]. As a result, thrombin might be only partially suppressed and microscopic emboli are produced [2]. Further, the majority of thrombin generation is triggered via factor VIIa and tissue factor, whereas the ACT reflects inhibition of contact activation, which is not indicative for the amount and time of thrombin generation [39]. Additionally, it is questionable whether adequate heparin neutralization will be achieved postoperatively, since ACT is poorly sensitive to low heparin concentrations. This could result in over dosage of protamine, or incomplete heparin reversal [33]. Measuring the anticoagulant effect of heparin with the ACT, may have little or no relationship to what is clinically happening [11]. Therefore, when monitoring anticoagulation exclusively with the ACT, there are a lot of pitfalls to overcome.
The complex process of haemostasis can be broken down into four components: platelet activation, thrombin generation, clot formation/stabilization, and fibrinolysis [40]. To get a better understanding of these processes during and after CPB, it would be desirable to have a coagulation test that provides information about all these phases. However, such a tool to monitor haemostasis adequately is lacking [2,8,41,42]. Standard coagulation tests do not reflect the activity of both the coagulation factors and the natural anticoagulant proteins, and the interaction with platelets [8,22]. In addition, tests are often time consuming and the results not rapidly available, so they do not reflect the current state of the coagulation system and could lead to inappropriate treatment [43]. At present a combination of haemostatic assays may provide more effective diagnostic information than the use of any single test [44], because the current tests are on its own often limited in utility.
Standard Haemostatic Assays
Platelet count is only a quantitative measurement and, does not give any information about the platelet functionality, therefore it is less reflective for bleeding [45]. However, in studies by Karkouti et al. [46] and Coakley et al. [47] it was shown that loss of platelets reflected by both pre- and post- CPB platelet count was associated with increased blood loss. Fibrinogen on the other hand is only a single factor, excluding the influence of other blood cells. Large decreases in fibrinogen and subsequent low fibrinogen levels both pre- and post- CPB, are shown to be predictive for increasing blood loss [46,48]. Though, Coakley et al. did not find postoperative measured fibrinogen to be associated with blood loss. Similarly, low plasma concentrations of fibrinogen were not significantly associated with increased homologous blood usage [49].
D-dimer levels are split products of F-XIII crosslinked fibrin and are determined with monoclonal antibody assays. An increase of D-dimer over the baseline value indicates excessive fibrin formation, stabilization by F-XIIIa and subsequent fibrinolysis [50], that is measured at a specific moment, but which does not reflect on-going coagulation activity. D-dimer levels do increase during cardiac surgery, but there is no association with blood loss [51]. Kuepper et al. concluded that the D-dimer assay has a relatively high negative predictive value (measured 15 minutes after protamine administration), which might be useful to identify patients who are unlikely to have an excessive postoperative bleeding [50]. This could be helpful to avoid unnecessary transfusions after cardiac surgery. One should be critical to interpret the results of D-dimer assays, because there is a known variability among different assays due to heterogeneity of fibrin degradation products in patient samples, reactivity of antibodies, different calibrators and different assay formats [50].
Viscoelastic Whole Blood Techniques
Viscoelastic whole blood techniques seem to be more suitable for reflecting the complex coagulation system. Thromboelastography (TEG) was first described by Hartert in 1948 [52]. Using this assay, whole blood is added to a cup in which a pin is suspended connected to a detector system. The cup initiates the movement and the viscoelastic changes that occur during coagulation are measured and recorded in a graphical representation of the fibrin polymerization process. This technique was very sensitive to vibrations with the resultant unstable reproducibility. Over the years, the technique was refined, and nowadays there are two systems available: the TEG (Haemoscope Corporation, IL, USA) using the original principle, and the rotational thromboelastometry (ROTEM, TEM International GmbH, Munich, Germany), which uses a modified principle where the pin inside a standing cuvette is moving. The TEG device has two independent measuring channels, which includes a platelet mapping assay. The latter provides information about a patients’ response to anti-platelet therapy. ROTEM is also performed in whole blood, and it provides therefore information on the contribution of fibrinogen and platelets to clot formation. The rate of fibrin polymerization as well as the overall clot strength is assessed. During the clotting process (conversion of fibrinogen to fibrin), the clot increasingly restricts the rotation of the pin with rising clot firmness. This is detected and converted in a graph of clot formation and subsequent lysis. ROTEM is suitable for a more timely assessment of fibrinogen levels (<15-20 minutes). The following different measurements can be performed in four independent channels:
EXTEM: extrinsically activated coagulation, by tissue factor
INTEM: intrinsically activated coagulation, by ellagic acid
FIBTEM: extrinsically activated coagulation, by tissue factor; any contribution of platelets to clot formation is eliminated by cytochalasin D, allowing detection of fibrinogen deficiency or fibrin polymerization disorders.
APTEM: extrinsically activated coagulation, by tissue factor; aprotinin is added in order to block fibrinolysis; this reveals hyperfibrinolysis when compared with the EXTEM.
HEPTEM: intrinsically activated coagulation, by ellagic acid, contains heparinase to eliminate any heparin effect. Compared with the INTEM assay, it specifically confirms the presence of residual heparin.
The nomenclature used for the TEG and the ROTEM are presented in Table 2, and the graphical representation of the ROTEM is shown in Figure 1. The curve of the TEG is comparable with the curve of the ROTEM.
| Definition | TEG | ROTEM |
| Time between addition of the activator and start of clot formation | r value | coagulation time (CT) |
| Time between start of clot formation and reaching an amplitude of 20 mm | k value | clot formation time (CFT) |
| Steepness of curve | alpha angle | alpha angle |
| Greatest amplitude | maximum amplitude | maximum clot firmness |
| Amplitude measured 60 minutes after onset of clotting, as a percentage of the greatest amplitude | lysis index | lysis index |
Table 2: Nomenclature used for TEG and ROTEM.
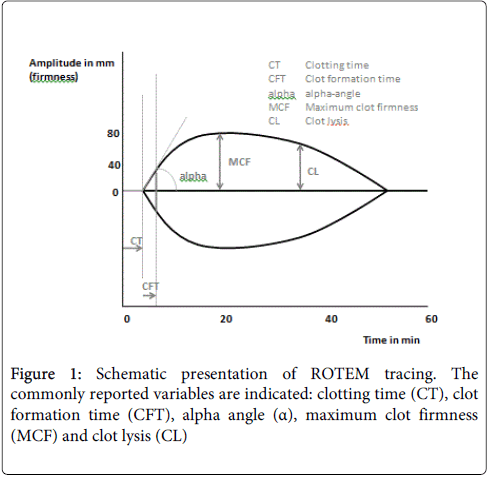
Figure 1: Schematic presentation of ROTEM tracing. The commonly reported variables are indicated: clotting time (CT), clot formation time (CFT), alpha angle (α), maximum clot firmness (MCF) and clot lysis (CL)
A disturbed activation of coagulation is indicated by a prolonged clotting time. An abnormal clot formation is indicated by a prolonged clot formation time and/or reduced clot firmness. Fibrinolysis is detected by lysis of the clot (> 15%) or, in case of ROTEM, by finding of a better clot formation (shorter CFT, greater MCF) in APTEM as compared to EXTEM. The clot formation time is used as a guide for fresh frozen plasma, the clot strength to judge platelet infusion. The degree of lysis is used to indicate the need for antifibrinolytic therapy.
Besides the primary difference of the movement of the cup and the pin, a second difference between the TEG and the ROTEM assay is the detector system, which is a torsion wire in the TEG, and an optical detector in the ROTEM [53]. Thirdly, the TEG system uses a kaolin/phospholipid mixture as activator, whereas in the ROTEM either ellagic acid or tissue factor is used. Lastly, the TEG uses a larger and less diluted blood volume in the cuvette [54]. Results in viscoelastic whole blood measurement using either TEG or ROTEM are therefore not completely interchangeable and clinical interpretation should be used with caution [54]. Wasowicz et al. [55] concluded in an observational study comprising 434 CPB patients that on-CPB thromboelastography could improve risk stratification for excessive blood loss postoperatively. In contrast, Coakley et al concluded that thromboelastometry was not predictive for postoperative bleeding in cardiac surgical patients undergoing CPB [47]. Consumption of allogenic blood products tends to decrease in case viscoelastic tests are used [56-58]. However, viscoelastic clot-based assays are mainly dependent on fibrinogen levels [47,59,60]. A great deal of haemostasis is not captured by the fibrin clotting endpoints used [61]. Only 5% of thrombin is formed when clotting-based assays terminated. This is not directly related to haemostasis and thrombosis, like thrombin concentrations are, but a covariable of one of the effects of thrombin formation, i.e. fibrin (-monomer) polymerization [62].
Platelet function tests
Although thrombocytopenia occurs during cardiac surgery, this alone infrequently leads to increased blood loss if the platelet function is normal [17]. Platelet dysfunction, is one of the most important causes of non-surgical bleeding after CPB, and is not assessed by standard haematology laboratory assays [15]. Nowadays, several platelet function tests are available. We will discuss a test based on aggregation, one based on shear stress, and the last based on platelet contribution to clot strength.
Classical light transmission aggregometry performed in platelet-rich plasma is the “gold standard” for platelet function testing [63,64], but data showing correlation with blood loss are lacking [64]. The Multiplate analyser is an instrument with five channels for parallel aggregometry measurements in whole blood. Blood and reagents were pipetted into test cells containing four electrodes that formed two independent sensor units. The ability of platelets to adhere to the metal sensors was measured by the change of electrical resistance between two sensor wires. This impedance change is plotted against time and the area under the aggregation curve was used to measure the aggregation response, quantified in arbitrary aggregation units (U). Whole blood platelet aggregometry is likely affected by a reduced haematocrit and become unreliable at platelet counts < 50*109/l [63,65]. The Multiplate device will produce a result in 10 min after sampling, except when adenosine diphosphate is used as an agonist [63]. Unfortunately, it does not reflect the complex interaction interaction between thrombin, fibrinogen and platelets, and the end result of the coagulation process, the formation of the clot.
The PFA-100 platelet function analyser is an in vitro system that provides a measure of platelet function in citrated whole blood. The PFA-100 assesses the time taken for a platelet plug to occlude a microscopic aperture within a membrane coated with platelet agonists, collagen and, depending on the cartridge, epinephrine or adenosine diphosphate (ADP). The time from the start of the test until the occlusion of the aperture by a platelet plug was reported as the PFA-100 closure time (s). The test can be performed in 5-8 minutes. The PFA-100 system provides automated assessment for inherited, acquired (CPB), or drug-induced platelet dysfunction.
The Platelet-Mapping assay is a modification of the TEG, measuring percentage platelet aggregation in the presence of ADP or arachidonic acid (AA). It was designed to monitor the effect of clopidogrel and aspirin on platelets and in decision-making for timing of cardiac surgery or other invasive procedures after discontinuation of antiplatelet therapy. This assay uses a viscoelastic test in whole blood to measure the clot strength (maximum amplitude) and detects the percentage of platelets inhibited by aspirin and clopidogrel. TEG platelet-mapping tracing shows the strength of coagulation formed by activated platelets [66]. In general, platelet function analyzers are sensitive enough to detect the effects of antiplatelet drugs on platelet function in cardiac surgical patients [15,63,64]. There is evidence that platelet function analyzers were able to predict patients at risk for increased postoperative blood loss [66-69] when performed in either the pre- or post-CPB setting. However, after correcting for haematocrit and platelet count there were no differences anymore between bleeders and non-bleeders measured by the PFA-100 [69], what led to the conclusion that PFA-100 is not useful for routine use after cardiac surgery [69]. Rahe-Meyer et al. found no correlation between decreased peri-operative platelet aggregometry measured by Multiplate and blood loss in the 24-h period after surgery [65]. Although both low pre- and post-operative platelet function tests defined groups of patients with significantly higher transfusion of platelet concentrates [65,66], there is no consensus to conclude that measuring platelet function is useful in transfusion algorithms [15,37].
Calibrated Automated Thrombography (CAT)
Thrombin is the most important enzyme in the thrombotic portion of the haemostatic reaction during CPB. Therefore, monitoring thrombin generation (TG) is of utmost importance. TG reflects much - if not all - of the overall function of the blood clotting system [62] and plays several roles such as modulating the cleavage of fibrinogen to fibrin, activating platelets and the process of fibrinolysis [61,70]. It extends from coagulation activator and inhibitor to cellular regulator. In 1953 the thrombin generation test was described by Macfarlane and Biggs [71], as to be a valid function test of the clotting system. Later, the calibrated automated thrombography (CAT) test, following triggering of plasma with tissue factor, was developed by Hemker and co-workers [62,72,73] for monitoring of the rate and extent of TG by the continuous measurement of the fluorescent split-product of the fluorogenic substrate. The course of TG is graphically represented in a thrombogram. TG is measured in a fluorometer equipped with 96 wells. In one well a calibrator has been added. In a second well TG is triggered with tissue factor and phospholipids in platelet poor plasma (PPP), and only with tissue factor in PRP. A fresh mixture of fluorogenic substrate (Z-Gly-Gly-Arg-AMC) and CaCl2 (called FluCa) is dispensed to all the wells to be measured. The readings from the TG are compared to the readings of the calibrator well, thrombin concentration is calculated and thrombin concentration in time is displayed. CAT parameters are: 1) lag time (min): the initiation phase of clotting, that equals the clotting time; 2) peak height (nM): the maximal amount of thrombin formed; 3) endogenous thrombin potential (ETP) (nM*min): the area under the TG curve, representing thrombin generation and decay in time; and 4) time to peak (min): the time needed to achieve the peak height (Figure 2). The total time course of CAT to provide the required clinical relevant information could be less than 30 minutes (depending on the haemostatic condition of the patient). The first parameters are already known within 5 minutes.
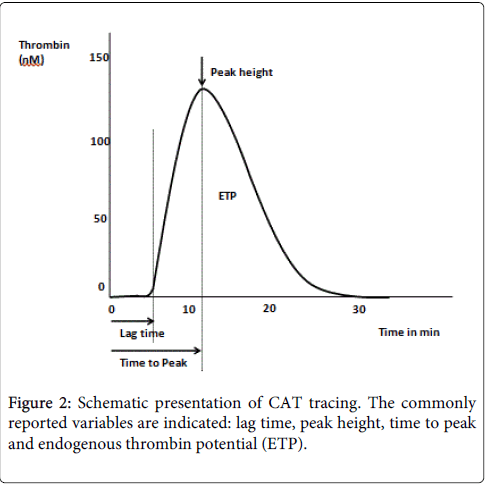
Figure 2: Schematic presentation of CAT tracing. The commonly reported variables are indicated: lag time, peak height, time to peak and endogenous thrombin potential (ETP).
Recently, it became possible to measure TG in whole blood instead of plasma. This is an important development as it is approaching the in vivo conditions more closely. No centrifugation step is required, which could lead to uncontrolled variations in cell counts and activation of blood cells. The whole blood CAT assay is described elsewhere [74].
CAT can be used for detection and quantification of bleeding tendency, for detecting hyper coagulability, and assessing substitution and antithrombotic treatments. There is already evidence that thrombin generation measured by CAT is predictive for increased bleeding risk after cardiac surgery [47,75-77], however, further research involving the clinical benefits is warranted.
The ideal way to monitor haemostasis and anticoagulation during CPB, should be a test that includes all factors that interact to create haemostasis at a specific moment: blood cells, plasma proteins, contributions of the vessel wall, flow conditions, and the influence of anticoagulants. Including all these aspects into one assay will reflect closer the in vivo circumstances. Measuring of thrombin generation in whole blood could be such a test. Besides the most ideal test conditions, the test should also be clinically useful. The clinical utility of coagulation tests is the likelihood that a test result will lead to an improved health outcome. In cardiac surgery this means to get more control over individual blood loss and to facilitate optimal, targeted administration of pharmacological agents and blood components in case of excessive bleeding [78]. The clinical consequences of a disturbed haemostatic condition could be reduced with more accurate control of heparin anticoagulation and its reversal. Novel pharmacological approaches have resulted in the introduction of new oral anticoagulants (NOACs) into the adult clinical setting. These, direct thrombin and factor Xa, inhibitors have been developed to reduce the well-established drawbacks of currently available anticoagulants (vitamin K antagonists and heparins). They are currently administered at fixed doses without control of their effect on the clotting system. However, measurement of their anticoagulant effect may be desirable in situations like bleeding and emergent surgery particularly when patients did not quit intake of NOACs. Whether NOACs require routine monitoring cannot be answered at present, as relevant data are lacking and monitoring is inadequate. Another practical aspect of running the ideal test is the simplicity, and results should be rapidly available. Point-of-care, preferably at the patient’s bedside, would be the goal of haemostatic monitoring, where interventions could be done immediately. Obviously, development of coagulation monitors in cardiac surgery starts with understanding the process of coagulation, the disturbances of coagulation, but also the snags and pitfalls. The clinical utility, especially prediction of bleeding postoperatively, is the next step in investigating available tests. The most ideal goal is to create an optimal test from bench to bedside in the near future.
Earlier diagnosis of haemostatic abnormalities and risk of bleeding in cardiac surgical patients undergoing cardiopulmonary bypass is warranted. Viscoelastic whole blood tests could improve timely identification of haemostatic disturbances. However, CAT gives a more complete reflection of the overall blood coagulation system. Further research of the clinical applicability of viscoelastic tests and CAT, preferable in whole blood, is required. Finally, several improvements such as simplicity in running the test, and a short turnaround time would be highly desirable.