Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 5
Background: A simple, portable measure of daytime sleepiness is the Oxford Sleep Resistance (OSLER-2) test; however its use is limited to those with good hand function. This study modified the OSLER-2 test to assess the measurement of daytime sleepiness using two alternative, non-hand-held response switches.
Methods: The unit was modified to accept the standard hand-held switch, a head-tap switch (“Jelly-bean”) and chin-tap switch (“Wand”). Participants were required to respond to a central LED light presented for one second every three seconds. It terminated following either seven consecutive missed responses (participant asleep) or forty minutes (maximum test length, “performance time”). Twenty-two able-bodied participants with no diagnosed sleep disorders were sleep restricted prior to three testing days where switch order was randomized. The test was performed four times over each day. Sleep latency, performance times and errors were recorded along with video of the switch use.
Results: Sleep latency was longer with the Wand (M=1265 sec (546)) than the Jelly-bean (M=1102 (544)) and hand-held switch (M=1037 sec (557), p<0.05). Performance times were longer with the Wand (M=1788 sec (695)) than the Jelly-bean (M=1530 sec (758); p<0.05) and hand-held switch (M=1459 sec (784); p<0.01). Sleep latency, performance times and errors did not differ significantly between the Jelly-bean and hand-held switches. Video suggested the Wand was occasionally activated erroneously by forward (drowsy) head-drops.
Conclusion: The Jelly-bean provides a possible alternative response switch to measure daytime sleepiness in those with limited hand function.
Keywords: Hand function; Performance; Sleep latency; Switches; Vigilance
Daytime sleepiness is a common, debilitating symptom for those suffering with a sleep disorder. It decreases work productivity [1], and impairs both mental health status [2] and the ability to perform daily activities [3]. Tests used to measure daytime sleepiness include the Multiple Sleep Latency Test (MSLT) and the Maintenance of Wakefulness Test (MWT) [4-6]. Both the MSLT and MWT are multi-nap approaches in which the ability to fall asleep and the ability to remain awake are tested respectively in the absence of alerting factors. Though simple tests, the use of Electro-encephalogram (EEG) monitoring to determine time of sleep onset makes these tests costly, labor intensive and typically confines their performance to specialized sleep units.
A behavioral equivalent called the Oxford Sleep Resistance (OSLER) test [7] was developed to reproduce many of the characteristics of the MWT [7,8]. Without the need for EEG monitoring or a trained technician, the OSLER test is a simple to use, less expensive and more portable method of measuring sleep latency than both the MSLT and MWT. The OSLER test requires a simple button response to a light flashed at pseudo-random intervals for one second every three seconds. Failure to respond to seven flashes is interpreted as sleep having occurred, otherwise the test continues for its complete duration of forty minutes. The test is limited in its present form however; it requires the participant to have adequate hand function to operate a response switch. Given that daytime sleepiness is a particularly common symptom amongst people with a spinal cord injury (SCI) [9,10], who have limited or no hand function, the inability to apply the portable, inexpensive benefits of the OSLER test to this population, in which travel to a sleep unit can be burdensome, is complexing. This study aimed to take the first steps in modifying the OSLER-2 test to incorporate switches that do not rely on hand function. This study performed an OSLER-2 switch comparison; it examined sleep latency measured on the OSLER-2 test using the modified switches compared to the standard hand-held one.
Study participants
Healthy, able-bodied people aged between 18 and 70 years, with no previous diagnosis of a sleep disorder were recruited from the community. Exclusion criteria included: visual problems not corrected by glasses or contact lenses; psychiatric or neurological disorders; addiction to nicotine; use of benzodiazepines; recent travel or planned travel across time zones during the study or shift work. Participants provided written informed consent and the study was approved by the Austin Health Human Research Ethics Committee. Participants who completed the study were remunerated for their time. The study is registered at www.anzctr.org.au (335819).
Procedure
Participants attended three days of testing at the Austin hospital sleep laboratory, each on the same weekday and separated by one week. One participant was unable to attend a day of testing due to illness and so completed the testing sessions over a four week period.
The night prior to each testing day, participants restricted their sleep to between 02:00 and 05:00. Sleep restriction was confirmed by a Sense Wear Pro3 armband (BodyMedia, Pittsburgh, USA) which records movements and sleep habits. Participants wore the armband for the 14 hours prior to each testing day.
The OSLER-2 test was conducted four times on each testing day, at 09:30, 11:30, 13:30 and 15:30 hours. The test records participant responses made via response switch to a light-emitting diode (LED) illuminated for one second every three seconds. The OLSER-2 test lasts for forty minutes unless the participant fails to respond to seven consecutive LED illuminations (21 sec) which is interpreted as the participant falling asleep and the test subsequently stops. The OSLER-2 records the times at which the test terminates, which is considered the sleep latency (minutes and seconds), along with the number of missed responses (“errors”). If a participant does not fall asleep, then the total time of forty minutes is displayed.
Three different response switches were used in this study, the standard OSLER-2 hand-held switch and two modified, non-hand-held switches not currently used in the OSLER-2 test, but commonly used by people with disabilities. The modified switches are: the “Jelly-bean” and “Magic Wand-Pad” (“Wand”) switches which are activated using a single, light touch head tap and a chin tap respectively which can be audible (Figures 1 and 2; note written consent to publish these photographic images was obtained by the person presented in these images). A different switch was used on each of the three days of testing, the order of which was blocked and randomized.
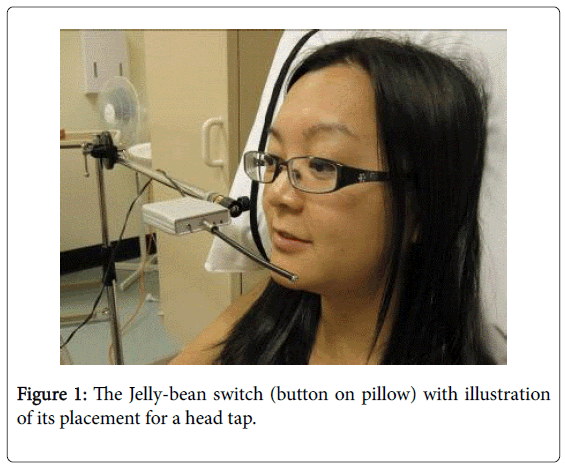
Figure 1: The Jelly-bean switch (button on pillow) with illustration of its placement for a head tap.
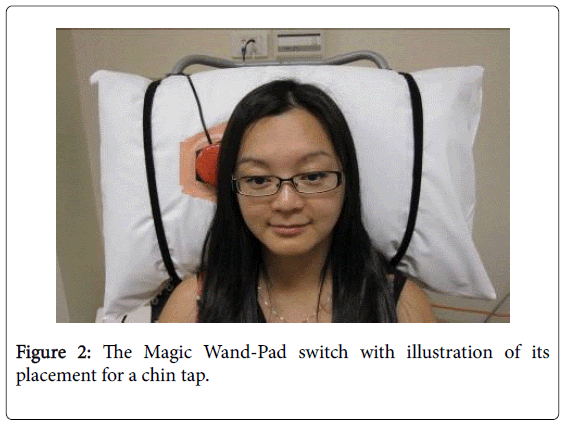
Figure 2: The Magic Wand-Pad switch with illustration of its placement for a chin tap.
During the OSLER-2 tests, participants sat in an isolated, noise proof room, darkened to approximately 0.1 Lux, with temperature between 21 and 24 degrees Celsius. The LED was placed at eye-level, two meters in front of the participant. The participant sat slightly reclined in a wheelchair to mimic the posture in which people with a motor disability, such as quadriplegia, would be expected to perform the test. Participants were asked to remain awake without using extraordinary measures to do so and to trigger the switch every time the LED illuminated. To help prevent the occurrence of deliberately terminated tests, participants were informed that test times may vary, but were not told that a failure to trigger the switch seven times consecutively would result in test termination. A video feed of the room was monitored during all tests to assess compliance to instructions.
To measure trait and state sleepiness and circadian rhythm type, participants completed the Epworth Sleepiness Scale (ESS) [11] and the Morningness-Eveningness Questionnaire (MEQ) [12] the morning of their first testing day and the Karolinska Sleepiness Scale (KSS) [13] immediately prior to and following each of the four testing sessions. The ESS asks participants to rate on a scale of 0-3 (0 being “would never doze”, 3 being “high chance of dozing”) how likely they would doze off or fall asleep in eight different situations and the scores are then totaled. The MEQ is a seven item questionnaire which measures the circadian rhythm type of a person, such as whether they are a “morning” person or an “evening” person. Three to four possible answers are given for each question, with each answer corresponding scores ranging from 0-6. These scores are totaled at the end of the questionnaire with results falling into one of six categories. The possible categories include “definitely morning type”, “moderately morning type”, “neither type”, “moderately evening type” and “definitely evening type”. The KSS is a nine-point Likert-type scale ranging in score from 1 (“very alert”) to 9 (“extremely sleepy, fighting sleep”). The KSS asks participants to indicate on the scale how sleepy they are feeling at that current time.
Between OSLER-2 tests, participants were encouraged to engage in sedentary activities such as reading and watching TV and were monitored to avoid falling asleep. A light lunch was provided following the 11:30 testing session and participants were not exposed to bright sunlight during their stay.
Participants completed a sleep diary for the duration of their involvement of the study to identify their typical sleep behavior. The diary recorded nightly sleep behaviour and caffeine and alcohol intake. Participants were asked not to smoke or consume alcohol, caffeine or energy drinks from the day before testing until the completion of their testing day.
Data analysis
Summary statistics are presented to describe the sample. Data collected from the OSLER-2 on each of the three testing days, which comprised four OSLER-2 test per day, was examined. Analyses were performed on two sets of data. The first was on the portion of the sample who fell asleep during the testing session and thus obtained a “sleep latency”. The second was on the entire sample, thus including those who did not fall asleep during the test, in order to examine switch “performance” times. Missed responses (“errors”) were also examined for the sleep latency and performance portions of the sample.
OSLER–2 Sleep latency and performance times
The proportion of the sample that fell asleep, thus obtaining a sleep latency across switch type and testing time of day was tabulated. Linear Mixed Model (LMM) analysis was used to examine fixed effects of switch type (Jelly-bean, Wand and hand-held), testing time over the day (09:30, 11:30, 13:30, and 15:30), and study week/switch order (week 1, 2, and 3) for both sleep latency and performance times. The participant was included in the model as a random intercept to allow for repeated test results, with a compound symmetric covariance structure to adjust for serial correlation across time within any given day (SPSS software, version 21.0; SPSS, Chicago, Illinois). Significant fixed effects from the LMM analyses were explored using pairwise comparisons. The reported effect size and confidence intervals from the significant fixed effects are from the LMM. This LMM approach was also used to compare state sleepiness (KSS) at the beginning of each testing time.
Error analyses
The LMM approach described was also used to examine the percentage of time corresponding to the appearance of errors during the OSLER-2 test. The calculation used to determine the percentage of time spent by each participant in making errors was: (3 seconds x number of errors/sleep latency duration in seconds) x100 [14].
For all LMM analyses made in this study, the initial model included a switch*time interaction in order to assess whether the effect of switch differed by testing time of day however as this was not statistically significant in any analysis, it was subsequently removed and the model re-analyzed without the interaction term. P values less than 0.05 were considered significant.
Participants
22 participants (15 female) were recruited into the study. Two failed to complete their third day of testing and one completed just one day of testing (three Wand and one hand-held switch testing days missed). The median (25th, 75th percentile ranges) age of the sample was 21 years (19.8, 26), BMI 22 kg/m2 (20.5, 24.0), abdominal circumference 75.5 cm (71.0, 86.0) and neck circumference 32.5 cm (30.0, 36.3).
Sleep diary
On the nights prior to sleep restriction, participants reported having a median (25th, 75th percentile ranges) of 7.5 (7.0, 8.0) hours sleep per night and generally feeling refreshed most mornings. Ten participants reported alcohol intake during their participation in the study with 8.5 (2.7, 25.3) standard drinks over the three week study period. Fifteen participants reported caffeine intake during this time, with 9 (4.0, 20.0) cups during the study period.
Data from the BodyMedia SenseWear Pro3 Armband confirmed that participants had restricted their sleep on the night before testing with a median sleep time of 2.4 hours (1.9 hrs, 2.7 hrs).
Trait and state sleepiness and circadian type
The mean (SD) ESS was 6.3 (3.4) indicating that participants did not experience excessive daytime sleepiness. The Morningness-Eveningness Scale (MEQ) indicated that of the sample, there were two “moderate morning types”, six “moderate evening types”, three “definite evening types” and eleven being classified as “neither morning or evening types”. The mean KSS score was 5.8 (1.6), which is interpreted as between “neither alert nor sleepy” and “sleepy-but no difficulty remaining awake”. KSS scores did not differ significantly before each of the four testing times on each of the three testing days.
OSLER-2 sleep latency and performance times
The proportion of participants who fell asleep overall and at each testing time of the day for each switch type is presented in Table 1.
| Overall Time points | Hand-held Switch | Jelly-bean Switch | Wand switch | |||
|---|---|---|---|---|---|---|
| (n=21) | % | (n=22) | % | (n=19) | % | |
| 18 | 85.7 | 19 | 86.4 | 16 | 84.2 | |
| 09:30 | 15 | 71.4 | 13 | 59.1 | 11 | 57.9 |
| 11:30 | 15 | 71.4 | 15 | 68.2 | 8 | 42.1 |
| 13:30 | 16 | 76.2 | 18 | 81.8 | 13 | 68.4 |
| 15:30 | 12 | 57.1 | 13 | 59.1 | 9 | 47.4 |
Table 1: Count of participants who demonstrated a sleep latency (7- missed responses) overall and at each testing time of day for each switch type.
The mean sleep latency and performance times for each switch type at each testing time of day are shown in Figures 3 and 4 respectively. The mean (SD) sleep latency and performance times for each switch are presented in Table 2.
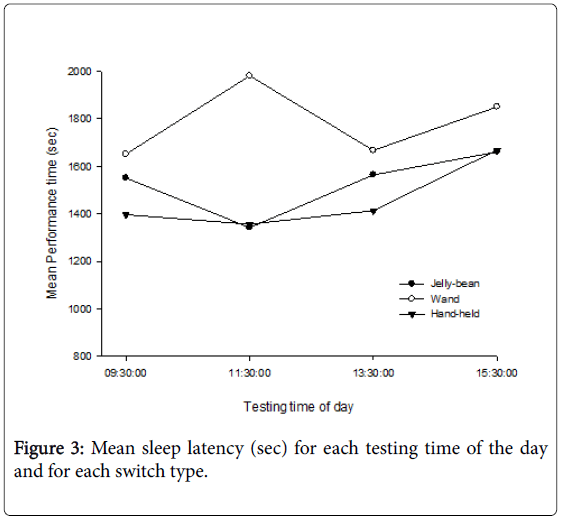
Figure 3: Mean sleep latency (sec) for each testing time of the day and for each switch type.
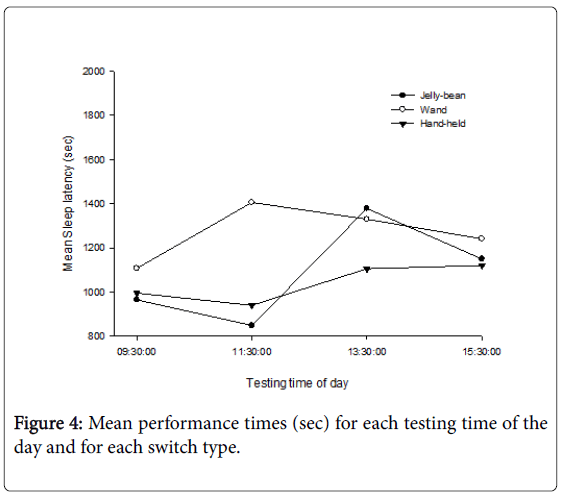
Figure 4: Mean performance times (sec) for each testing time of the day and for each switch type.
| Hand-held Switch | Jelly-bean Switch | Wand Switch | ||||
|---|---|---|---|---|---|---|
| M (SD) | N | M (SD) | N | M (SD) | N | |
| Sleep latency (sec) | 1037 (557) | 58 | 1102 (544) | 59 | 1265 (546) | 41 |
| Performance time (sec) | 1459 (784) | 84 | 1530 (758) | 88 | 1788 (695) | 76 |
| Time spent making errors (SL) (%) | 15.1 (7.9) | 58 | 16.0 (9.2) | 59 | 13.5 (8.2) | 41 |
| Time spent making errors (Perf) (%) | 11.4 (9.1) | 84 | 11.6 (10.2) | 88 | 9.9 (8.9) | 76 |
Table 2: The mean (SD) sleep latency, performance times and time spent making errors for each switch type. (sec: second; Time spent making errors (SL): portion of sample who fell asleep as indicated by seven consecutive missed responses to the LED stimuli; Time spent making errors (Perf) is for the whole sample).
The LMM showed a statistically significant effect for switch type (p<0.05) for both sleep latency and performance times and a significant effect for switch order (p<0.05) for performance times. Participants fell asleep significantly faster when using the hand-held than the Wand switch (p<0.05; mean difference: 301.3; CI: -59.9, -542.7). Sleep latency times did not differ significantly between the Wand and Jelly-bean switches or between the Jelly-bean and hand-held switches.
Performance times were significantly longer when using the Wand compared to the Jelly-bean (p<0.05; mean difference: 330.5; CI: 71.6, 589.3) and hand-held switch (p<0.01; mean difference: 359.7; CI: 100.7, 618.8). There was no significant difference in performance time between the Jelly-bean and hand-held switches.
Mean performance times were significantly longer for the first (1778 sec (707)) presented switch compared to both the second (1509 sec (766)) presented switch (p<0.05; mean difference: -284.4: CI: 35.2, 533.6) and the third (1445 sec (770)) presented switch (p<0.05; mean difference: 282.1; CI: 25.2, 539.0). There was no significant difference in performance times between the second and third presented switches.
Error analysis
The mean (SD) percent of time spent making errors on each switch are presented in Table 2 for the portion of the sample who obtained sleep latency and also for performance times (whole sample).
The LMM examining the percent of time spent making errors showed that there was a significant effect for the time of day the test was conducted for both the sleep latency (p<0.01) and performance (p<0.01) portions of the group. For the sleep latency group, a higher mean (SD) percentage of time making errors was observed during the 11:30 testing session (18.7% (9.8)) than the 09:30 (14.5% (7.6); p<0.01; mean difference: 4.0; CI: 1.2, 6.7), 13:30 (12.4% (7.1); p<0.001; mean difference: 5.3; CI: 2.6, 8.0) and 15:30 (15.2% (8.3); p<0.05; mean difference: 3.5; CI: 0.6, 6.3) testing sessions.
Similarly, for the performance time portion of the sample, the mean percentage of time making errors was also significantly higher during the 11:30 testing session (13.2% (11.2)) than the 09:30 (10.0% (9.2); p<0.01; mean difference: 3.2; CI: 1.2, 5.2), 13:30 (10.7%, (8.0); p<0.05; mean difference: 2.5; CI: 0.48, 4.45) and the 15:30 (10.2% (9.1); p<0.01; mean difference: 3.0; CI: 1.0, 5.0) testing sessions. There was no significant difference between switch type in the time spent making errors for both the sleep latency and performance time groups.
This is the first study to examine the use of non-hand-held response switches to perform the OSLER-2 test as a measure of daytime sleepiness. The aim of this study was to examine sleep latency measured on the OSLER-2 test using modified non hand-held switches compared to the standard hand-held one. Comparable findings were observed between the Jelly-bean and hand-held switches. In contrast, the modified Wand switch presented longer sleep latency and performance times, and fewer errors.
The differences in response requirements along with design characteristics may account for the varying findings observed between the non-hand-held and hand-held switches. These include: the presence of audible feedback noise, the required muscle response (“button push”) movement and the varying placement of the switch for response. Both modified switches provide an audible feedback noise when pushed and require a larger movement to respond to the LED light than the hand-held switch. The larger bodily movements with the head and chin taps were observed via the video link during the testing sessions, however not so for the simple finger response of the hand-held switch. The larger movements require slightly more response time and may heighten attention. The presence of audible feedback may have increased alertness and may also have increased participant’s motivation which has been shown to effect sleep latency in similar tests [15]. Our results suggest that auditory feedback and greater bodily movement may have contributed to the poorer overall performance of the Wand.
The video feed also highlighted that the placement of the modified switches for response to the LED possibly contributed to the different results between the switches. When becoming drowsy during the test, the participants’ head tended to move away from the Jelly-bean, and their finger away from the hand-held switch. In contrast, when using the Wand, drowsiness resulted in the head slumping forward and into the switch. Subsequently, participants who appeared to be close to falling asleep whilst using the Wand ultimately activated the switch and prevented the occurrence of a missed response. Fewer participants were then registered as having fallen asleep and less errors overall observed whilst using the Wand due to the switch being erroneously activated.
A significant effect of switch presentation order was observed when examining the performance times of the switches. Performance times were significantly longer for the switch which was first used by participants than the performance times of the second or third presented switches. This finding is likely reflective of the participants becoming familiar with the task requirements, experimental environment and protocol. Once becoming familiar after the first testing day, participants may have become more comfortable and less cautious about what was required and thus faster at completing the tests for the second and third testing days. As the switch order was randomised and counterbalanced, this effect of switch presentation order would be expected to have equalled out across switches.
It was also observed that there was an increase in errors during the 11:30 testing session which could be reflective of a “post-lunch dip” in performance which has been observed regardless of an individual having had lunch or not [16]. The dip in performance is believed to be related to an increased propensity towards sleep at this time of the day, driven by the homeostatic sleep drive and the circadian rhythm [16]. The longer a person remains awake, the greater the desire to sleep. Naturally this sleep drive peaks prior to night sleep, however it is also higher in the afternoon than the morning. Whilst the post-lunch dip is more often observed in the midafternoon hours, the fact that the participants in this study were sleep deprived the night before testing, may have potentially pushed this dip in performance to occur earlier.
Future research
The present study sought to compare the performance of the different switch types on the OSLER test. The logical proceeding research would administer the OSLER-2 test with modified non hand-held switches to a population with limited hand function. This would allow the determination of whether such modified switches, in particular the Jelly-bean, could in fact be used by people with inadequate hand function who may be exhibiting symptoms of a sleep disorder. Future research could also apply EEG whilst the OSLER test with modified switches was being performed to provide normative values for this modified test in order to understand what length of sleep latency is indicative of daytime sleepiness.
The findings from this study suggest that sleep latency as measured by the Jelly-bean switch is more comparable to sleep latency as measured with the standard hand-held OSLER-2 switch. The Wand switch appears to be unreliable for use with the OSLER-2 test. The Wand may result in misleading daytime sleepiness information and potentially contribute to a missed diagnosis of a sleep disorder. The alternative Jelly-bean switch, may provide a simple, inexpensive, portable means for people with limited or no hand function to have their daytime sleepiness examined in the assessment of an underlying sleep disorder.
We acknowledge the generous support of the participants and Steven Vander Hoorn for his statistical advice. This project is proudly supported by the Transport Accident Commission (TAC). This funding source had no involvement in the conduct or publication of this study.
This project is proudly supported by the Transport Accident Commission (TAC). This funding source had no involvement in the conduct or publication of this study.