Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2014) Volume 2, Issue 2
Objective: The number of HIV-infected women experiencing menopause is rapidly increasing. The aim of this study was to compare the physical and psychological health profile of menopausal women with and without HIV.
Methods: Case-control study, assessing clinical manifestations of menopause in HIV infected cases and in uninfected controls. Determinants of physical (subclinical cardiovascular diseases, prevalence of diabetes mellitus, chronic kidney disease, hypothyroidism and risk of osteoporotic fractures) and psychological health (depression, quality of life in menopause and sexual dysfunction) were evaluated. The prevalence of poly-pathology (Pp) defined as the concurrent presence of 2 or more diseases was also assessed.
Results: 29 (47.5%) HIV-infected and 32 (52.5%) HIV-uninfected postmenopausal women infection were enrolled. On average, menopause occurred 3 years earlier in HIV-infected than in uninfected women (p= .01). In spite of a trend toward a greater prevalence of Pp (p=.22), the only physical indicators differing between cases and controls were a greater risk profile for osteoporotic fracture (p<0.001) and a significantly increased arterial stiffness (p=.007). In addition, cases exhibited a poorer psychological health profile with regard to depression (p=.005), sexual dysfunction (p=.02) and physical menopausal symptoms (p=.05).
Conclusion: In spite of a relatively similar physical health profile, menopause in HIV infected women is characterized by a poorer psychological profile compared to HIV uninfected women.
<Keywords: HIV; Menopause; Polypathology; Osteoporosis; Depression; Cardiovascular disease
Recently, the longer life expectancy of people living with HIV have led to a substantial change of HIV demography [1]. Indeed, it is estimated that more than half of all HIV- infected patients in the United States will be over the age of 50 by the year 2015 [2]. The number of women with HIV experiencing menopause is therefore increasing [3]. Moreover, as a result of the virus activity and of the antiretroviral therapy, the menopausal transition has some unique clinical features among HIV infected patients [3]. Despite of this, little is known about menopause in HIV patients.
The aim of this study was to compare the physical and psychological health profile of postmenopausal women with and without HIV infection.
This is a single center, case-control study, comparing postmenopausal women with and without HIV infection. HIV infected post-menopausal women (Cases) were recruited at the HIV University Clinic in Modena and HIV uninfected post-menopausal women (Controls) were recruited at a General Practice Clinic in the same health district in Modena.
Inclusion criteria were postmenopausal status according to WHO definition and Body Mass Index (BMI) less than 33. In order to obtain a comparable population, and given the confounding effect of age on our outcomes and the small sample size, we excluded from the control group women over the age of 60 [4]. Age at menopause was obtained adding 12 months to the last menstruation date reported. All patients were interviewed about parity, previous voluntary or spontaneous abortions and presence of prolonged amenorrhea lasting less than 12 months. Demographic, anthropometric and lifestyle data were collected at study entry.
Physical health determinants
The physical health assessment included estimates of cardiovascular disease (CVD) and osteoporotic fracture risk, measurements of subclinical CVD, as well as evaluation of comorbidities prevalence.
Among CVD risk factors, hypertension was defined as blood pressure >140-90 mmHg or current use of anti-hypertensive therapy and metabolic syndrome was defined according to the ATPIII criteria [5,6].
Ten-year risk of hard coronary heart disease was assessed using the Framingham algorithm (available at http://hp2010.nhlbihin.net/atpiii/ calculator.asp?usertype=prof) and ten-year fracture risk using the FRAX risk score validated for Italian women (available at http://www. shef.ac.uk/FRAX/tool.jsp?country=11).
Assessment for subclinical CVD was obtained through Pulse Wave Velocity (PWV, m/s) and common and internal carotid Intima Media Thickness (IMT, mm) measurements. Carotid-femoral PWV was estimated transcutaneously and non-invasively via a tonometric technique [7]. High resolution B-mode carotid artery ultrasound was used to measure the IMT [8]. The same sonographer performed each test.
Comorbidities ascertainment included a previous history of acute myocardial infarction, coronary artery disease, stroke, coronary artery bypass grafting, and angioplasty. Type 2 diabetes mellitus (T2DM) was defined as fasting glucose >126 mg/dL or use of any antidiabetic drugs [9]. Chronic kidney disease (CKD) was defined as glomerular filtration rate (estimated via the MDRD equation) below 60 ml/min/1.73m2 [10]. Hypothyroidism was diagnosed in case of increased levels of Thyroid Stimulating Hormone (TSH>5 mU/L) in two consecutive measurements or current use of T4 hormone replacement therapy [11]. Osteoporosis was defined as t-score<-2.5 Standard Deviations (SD) for either lumbar or femoral bone mineral density or clinical history of fragility fractures[12]. Finally, Polypatology (Pp) was defined by the concurrent presence of 2 or more comorbidities.
Psychological health determinants
Psychological health was assessed with self-administered questionnaires. Depression was measured with the 10-item Center for Epidemiologic Studies Depression (CESD-10) Scale [13]. Quality of life during menopause was assessed via the Menopause-Specific Quality of Life (MEN-QoL) questionnaire [14]. Sexual dysfunction was explored with Female Sexual Function Index (FSFI) questionnaire [15]. All the final scores were considered as continuous variables.
Statistical analysis
Mann-Whitney-U and Fisher exact test were used to compare continuous and categorical variables in cases and controls. Logistic regression analysis was performed to evaluate the probability of presence of Pp in the two groups. Multivariable linear regression analysis was used to compare age adjusted PWV data. A P-value of <0.05 was considered statistically significant. Statistical analyses were performed using STATA 10.1 Intercooled version for Mac, StataCorp, Collage Station, TX, USA.
Ethics statement
The research has been approved by the authors’ local Institutional Review Board (IRB): Comitato Etico Provinciale of Modena.
Participants provided their verbal informed consent to participate in this study. Written consent was not obtained, according to the ethics committees consent procedure, because it was a retrospective observational study in which investigators offered the best clinical practice and only asked the partecipants to fill some self-administered questionnaires.
All clinical investigations have been conducted according to the principles expressed in the Declaration of Helsinki.
| HIV - (n =32) | HIV + (n=29) | p-value | |
|---|---|---|---|
| Demographic and anthropometric data | |||
| Age, mean ± SD | 57±2 | 55±6 | 0.109 |
| Age at menopause, mean ± SD | 50±6 | 47±6 | 0.010 |
| Children, median (range) | 1 (1-2) | 0 (0-1) | 0.007 |
| Abortions, median (range) | 0 (0-1) | 1 (1-1) | 0.002 |
| Irregular periods, number (%) | 8 (25) | 16 (57) | 0.143 |
| BMI, mean ± SD | 25 ± 3 | 24 ± 4 | 0.330 |
| Waist Circumference, median (range) cm | 86 (79-96) | 86 (78-91) | 0.551 |
| Diastolic Blood Pressure, median (range) mmHg | 80 (70-88) | 80 (70-90) | 0.758 |
| Systolic Blood Pressure, median (range) mmHg | 120 (120- 143) | 123 (110-130) | 0.285 |
| HCV co-infection , number (%) | 1 (3) | 8 (31) | 0.004 |
| Life style | |||
| Physical activity None, number (%) Moderate, number (%) Intense*, number (%) | 15(47%) 12(37%) 5 (16%) | 17(65%) 9 (35%) 0 (0%) | 0. 083 |
| Smoking, number (%) | 8 (25%) | 7 (27%) | 0.868 |
| Alcohol None, number (%) Moderate, number (%) Intense*, number (%) | 32 (100) 0 (0) 0 (0) | 47 (82) 10 (18) 0 (0) | <0.001 |
| HIV-specific data | |||
| Years of HIV, median (range) | 17 (11-20) | ||
| CD4+ cells count, median (range) cells/µL Nadir Current (number) Current (%) | 183 (117-285) 568 (439-790) 32 (24-37) | ||
| Undetectable viral load, number (%) | 21 (75) | ||
| Month of NRTI exposure median (range) | 118 (70-226) | ||
| Month of NNRTI exposure median (range) | 23 (0-92) | ||
| Month of IP exposure median (range) | 36 (10-61) | ||
*Alcohol intake: heavy > 20 g of ethanol, physical activity: intense>4 h/week
Table 1: Demographic, anthropometric and clinical data of the population.
| HIV- | HIV+ | p-value | |
|---|---|---|---|
| Physical health | |||
| Risk estimators | |||
| Metabolic syndrome, number (%) | 4 (12.5) | 5 (17.2) | 0.602 |
| Triglycerides, median (range) mg/dl | 86 (65-108) | 117 (86-128) | 0.017 |
| Total cholesterol, median (range) mg/dl | 209 (187-238) | 224 (168-257) | 0.993 |
| HDL cholesterol, median (range) mg/dl | 55 (44-70) | 59 (49-71) | 0.463 |
| LDL cholesterol, median (range) mg/dl | 137 (106-157) | 121 (91-144) | 0.120 |
| Fasting glucose, median (range) mg/dl | 89 (82-95) | 97 (89-102) | 0.007 |
| Framingham risk score, median (range) | 2 (1-4) | 1 (1-2) | 0.072 |
| FRAX score 10-year osteoporotic fracture risk, median (range) 10-years hip fracture risk, median (range) |
4.0 (3.6-4,7) 0.6 (0.5-1.0) |
5.8 (5.0-6.6) 1.2 (0.8-1.8) |
<0.001 <0.001 |
| Subclinical atherosclerosis | |||
| PWV, median (95% CI) m/s | 6.6 (6.2-7.0) | 7.4 (7.0-7.9) | 0.007 |
| IMT Right CCA, median (range) cm Left CCA, median (range) cm Right ICA, median (range) cm Left ICA, median (range) cm |
0.09 (.08 - .1) 0.09(.08-.1) 0.08(.07- .08) 0.08 (.07- .08) |
0.08 (.07- .1) 0.10 (.07- .1) 0.07(.07-. 08) 0.07 (.06- .1) |
0.236 0.810 0.294 0.737 |
| Clinical diseases | |||
| CVD, number (%) | 0 (0%) | 0 (0%) | |
| Osteoporotic fractures, number (%) | 0 (0%) | 0 (0%) | |
| Hypertension, number (%) | 11 (34%) | 11 (39%) | 0.694 |
| Hypothyroidism, number (%) | 4 (13%) | 9 (32%) | 0.065 |
| Chronic Kidney Disease, number (%) | 0 (0%) | 4 (15%) | 0.086 |
| Diabetes, number (%) | 3 (9) | 5 (18) | 0.335 |
| Osteoporosis, number (%) | 6 (19) | 10 (36) | 0.138 |
| Poly-pathology, number (%) | 1 (3%) | 5 (17%) | 0.088 |
| Psychological health | |||
| CESD-10, median (range) | 16 (15-18) | 18 (17-21) | 0.005 |
| MEN-QoL Vasomotor, median (range) Psychosocial, median (range) Physical, median (range) Sexual, median (range) |
9 (4-13) 22 (16-37) 40 (35-58) 8 (4-12) |
11 (6-15) 24 (17-36) 58 (39-73) 10 (6-17) |
0.158 0.412 0.057 0.240 |
| FSFI, median (range) | 28 (21-30) | 20 (3-26) | 0.029 |
CVD: cardiovascular disease; PWV: Pulse wave velocity; IMT: intima-media thickness; FRAX score: Fracture Risk Assessment Tool ; CESD-10: 10-item Center for Epidemiologic Studies Depression ; MEN-QoL: Menopause-Specific Quality of Life; FSFI: Female Sexual Function Index.
Table 2: Physical and psychological health data.
61 post-menopausal women were enrolled in the study, 29 (47.5%) were HIV-infected and 32 (52,5%) were HIV-uninfected. Table 1 shows demographic and anthropometric data of the two groups. Mean age was similar in the two populations (55 vs. 57 years respectively, p= 0.10) and all women included in the study were Caucasian. On average, menopause occurred about 3 years earlier in HIV-infected than in non-infected women (47 ± 6 vs. 50 ± 6 years; p=0.01). A lower number of children (0 vs. 1, p=0.007), a higher number of abortions (1 vs. 0, p=0.002) a greater alcohol and smoking consumption (p<0,001) were observed in HIV infected women (Table 1).
As summarized in Table 2, we noted a similar metabolic profile in the two populations with the exception of a higher median fasting glucose and triglycerides levels observed in cases (89 vs. 97 mg/dl, p=0.007 and 86 vs. 117 mg/dl respectively, p=0.01). The metabolic syndrome prevalence (12.5% of cases vs. 17.2% of controls; p=0.60) and the ten-year risk prediction of CVD did not differ in the two study groups. To the contrary, the ten-year risk prediction of both major osteoporotic (5.8 vs. 4.0, p<0.001) and hip fracture (1.2 vs. 0.6, p<0.001) was higher in cases compared to controls.
Arterial stiffness but not the atherosclerotic burden was different in the two study groups. Indeed, the age-adjusted PWV was on average about 1 m/sec higher in cases than controls [7.4 (95% CI: 7.0-7.9) m/s, vs. 6.6 (95% CI: 6.2-7.0) m/s; p=0.007] whereas both common and internal carotid artery IMT appeared similar in the two study groups (Table 2). Similarly, no difference in the prevalence of CVD, hypothyroidism, CKD, type 2 diabetes mellitus or osteoporotic fractures was noted in the two study populations. A suggestive trend toward a higher prevalence of any co-morbidities and Polipatology (Pp) was found in HIV infected compared to uninfected women (17% vs. 3%, p=0.08). Notably, time from menopause (years) was associated with a trend toward increased risk of developing Pp in cases but not controls (p=0.11) (Figure 1).
HIV infected women showed a poorer psychological health profile compared to uninfected women. In particular depression, evaluated with CESD-10 score, was more prevalent in this first group (median score 18 vs. 16, p=0.005), as well as sexual dysfunction, evaluated with FSFI score (median score 28 vs. 20; p=0.02) and physical menopausal symptoms, evaluated with MEN-QoL (median score 58 vs. 40; p=0.05).
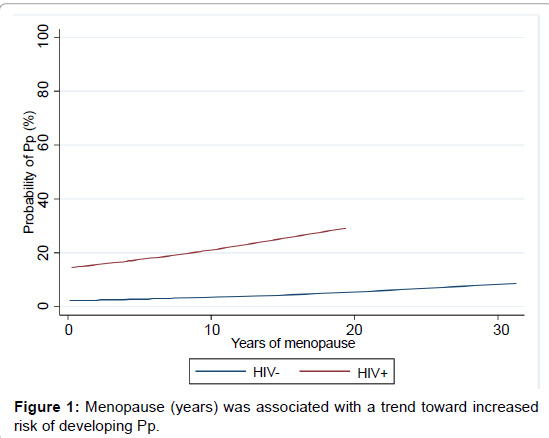
Figure 1:Menopause (years) was associated with a trend toward increased risk of developing Pp.
In this study we found that HIV-infected women experiment earlier menopause onset compared to HIV-uninfected controls. While a poorer psychological health profile was observed in cases compared to controls, the physical health assessment resulted similar in the two groups.
Despite the growing number of HIV infected women entering menopause, very little is known about the characteristics of this physiological transition in this population. Previous studies have focused on specific aspects of menopause in HIV patients [16-20]. In this study we used a comprehensive approach to describe menopause in HIV, assessing its impact on physical, as well as psychological women’s health.
We confirmed, and expanded to the post-menopausal population, the higher prevalence of depressive symptoms and sexual dysfunction previously documented in the general HIV infected population [21-26]. As suggested in previous literature, some of the typical HIVrelated psychological stressors, such as body image alteration, reactive depression, fear of HIV transmission to partner and HIV stigma, might contribute to explain these findings. Previous studies showed that HIV infected women report more menopausal symptoms than HIV uninfected controls [16,17]. Interestingly, in our sample the quality of life measured through the MEN-QoL questionnaire, was impacted more by physical symptoms than by vasomotor or psychological symptoms. This finding is in contrast with previous studies, reporting higher prevalence of hot flushes and psychological menopausal symptoms (e.g. irritability) among HIV infected women [16-20]. This might be due to the fact that our population had already completed the menopausal transition, and was therefore less likely to experience such symptoms. In addition, HIV infected women may experience more general physical symptoms (e.g. pain) due their higher number of comorbidities and depressive symptoms.
In our study, women with HIV presented a higher risk of hip and vertebral injure compared to uninfected controls. Postmenopausal status is a well-known risk factor for osteoporotic fractures; in addition, previous studies reported a higher prevalence of osteoporosis and fragility fractures among individuals with HIV [27-29].
Among subclinical cardiovascular outcomes, a significant increase in PWV, but not IMT in HIV infected postmenopausal women compared to controls was detected. The lack of association with IMT might be due to the small sample size, or to the early stage of the atherosclerotic disease, which is likely considering the relatively young age of our population. As PWV is closely associated with arterial aging, the increased arterial stiffness can be considered a marker of accelerated vascular senescence among HIV infected women [30]. However, this hypothesis needs to be tested in larger and prospective studies.
Despite an increasing trend in the prevalence of comorbidities among HIV infected individuals, we were unable to demonstrate a significant difference between the two study groups neither considering these pathologies separately nor clustered in Pp. Nonetheless, in keeping with previous results, our study describes an overall poorer health profile in postmenopausal woman with HIV compared to controls.
The cross-sectional nature of the study as well as the small sample size greatly limits the interpretation of current results. However, the holistic approach including physical and psychological assessment of menopause related aspects is, in the authors’ opinion, the major strengths of the present study as it allows a comprehensive evaluation and description of this important hallmark of women’s life. In addition, given the young age of our population and the consequent low prevalence of clinically documented diseases, we assessed risk prediction algorithms and sub-clinical outcomes in order to compare the physical health of HIV-infected and uninfected individuals.
In conclusion, we found that women with HIV are prone to develop earlier and more severe concerns during this physiological transition, compared to HIV negative controls. A careful and comprehensive evaluation of these patients is needed in order to address the specific features of menopause in HIV infected women.