Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2014) Volume 2, Issue 1
Background: Activities generating relatively high ground-reaction forces produce greater gains in bone mass than low- to moderate-intensity forces, especially when imposed during early childhood. We investigated in a pediatric population the amount of time spent in Vigorous Physical Activity (VPA), that is currently used to estimate high-intensity forces beneficial to skeletal health. The objectives of this study were: 1) to quantify the proportion in a general pediatric population that do not accumulate at least 20 minutes of VPA daily, which is currently recommended for bone health; 2) and to identify any age and gender-based differences.
Methods: Physical activity wasrecorded during 10 days using an uniaxial accelerometer in 255 children and adolescents (117 females; 138 males). According to Ekelund et al.,VPA was defined as > 3000 counts.min-1. The time spent at VPA intensity was expressed as minutes per day, and the proportion of subjects who accumulated less than 20 minutes of VPA daily was assessed considering gender and age.
Results: Our cohort of healthy children and teenagers had a normal mean value of VPA. However, 31.8% of the participants (31.9% of males and 31.6% of females) did not accumulate at least 20 minutes of VPA daily. Vigorous PA was 31.7% lower in females compared to males.Finally, the time spent in VPA decreased significantly with age in the male group (t=-2.5, p=0.014), but not in the female group (t=-1.6, p=0.105).
Conclusions: Vigorous PA measured by accelerometer is a useful and valid tool to assess the amount of highintensity forces beneficial to skeletal health during growth. Around 30% of children and teenagers of both genders do not accumulate at least 20 minutes of VPA. We may hypothesise that the gender-related differences in BMD may be due partially to the difference in VPA observed in this study, females being less vigorously active. Further research is needed to establish the relationship between the VPA level and bone mineral accretion.
<Keywords: Bone health; Physical activity; Accelerometer; CSA; Vigorous; Ground-reaction force; Gender; Accretion
Weight bearing physical activity has beneficial effects on bone health across the age spectrum [1]. The skeleton needs continuous physical stimulation to maintain healthy bones, otherwise bone loss ensues [2]. In childhood, exercise exerts a positive effect on bone growth, especially if the activity has been initiated before puberty or in the early pubertal period [3-5]. Bone mineral mass is higher in children who are physically active than in those who are mildly active [6], particularly those who engage in activities that generate high impact forces [7-9]. Studies have shown that high-intensity forces, especially when applied during early childhood, produce greater gains in bone mass than low to moderate-intensity forces [3,10-13]. Based on this evidence, it is now recommended that physical activity (PA) for children should include activities generating relatively high ground-reaction forces, such as jumping, skipping, running, and possibly strengthening exercises [5].
Accurate and reliable accelerometers have been developed for quantifying PA level in children and adolescents. These devices provide an objective measure of PA which is not dependant on self report because they measure the intensity of PA, as well as the frequency. Many researchers have published threshold of activity counts equating to different intensities [14-18], and different PA intensity categories have thus been determined, i.e. sedentary behaviour, light PA, moderate PA, and vigorous PA. On this subject, the time spent in Vigorous PA (VPA) is currently recognized to reflect high-intensity forces beneficial to skeletal health.
To our current knowledge, measurement of VPA levels by accelerometers has been rarely explored in children and adolescents. The objectives of this study were: 1) to measure the level of VPA in a general paediatric population and to quantify the proportion of children who do not accumulate at least 20 minutes of VPA; 2) and to identify any age and gender-based differences.
Participants
We recruited 300 healthy children and adolescents for the study through an advertisement placed in the Child and Adolescent Department of University of Geneva Hospitals, Switzerland. Exclusion criteria were: prior history of bone fractures; chronic disease; congenital or acquired bone disease; any condition limiting physical activity; and hospitalization for more than 2 weeks in the previous 12 months. All participants and their parents provided written consent and the protocol was approved by the institutional ethics committee (protocol # 04-057, ped 04-002).
Anthropometric measurements
Standing height (m) was measured in bare or stocking feet using a precision mechanical stadiometer (Holtain Ltd, Dyfed, UK), and body weight (kg) by a mechanical Seca®calibratedeam scale (Seca, Reinach, Switzerland). Body Mass Index (BMI) was calculated as weight in kilograms (kg) divided by height in meters squared (m2).
Physical activity measurement
Objective measures of PA were obtained using an uniaxial accelerometer (Actigraph® 7164, MTI, Fort Walton Beach, FL, USA). The monitor was set on a 1-min cycle; at the end of each run, the sum was stored in the memory and the numerical integrator reset. Monitors were attached vertically above the iliac crest of the right hip. Accelerometers were programmed to start recording at 8 am on the first day of measurement and participants were asked to wear them continuously for 10 days. Recordings of physical activity started on Monday, Tuesday, or Wednesday to ensure measurement of two weekend days. Data collection was conducted during all seasons.
| Age, physical characteristics, and time spent in VPA of all participants | |
|---|---|
| Age (yrs) | 11.4 ± 3 |
| Height (cm) | 149 ± 17.8 |
| Weight (kg) | 41.9 ± 15.3 |
| BMI (kg/m2) | 18.2 ± 3.2 |
| VPA (min/day) | 32.9 ± 22.1 |
Table 1: Age, physical characteristics, and mean time spent in VPA of all
participants are presented.
| Gender differences in VPA | |||
|---|---|---|---|
| Gender | Females | Males | p |
| Nbr of cases | 117 | 138 | - |
| Age (yrs) | 11.1 ± 2.9 | 11.7 ± 3 | 0.090 |
| Height (cm) | 146.4 ± 16.5 | 151.2 ± 18.7 | 0.031 |
| Weight (kg) | 39.3 ± 13.9 | 44.1 ± 16.2 | 0.012 |
| BMI (kg/cm2) | 17.7 ± 3.1 | 18.6 ± 3.2 | 0.036 |
| VPA (min/day) | 26.3 ± 6.5 | 38.5 ± 24.6 | <0.001 |
| % of cases with VPA < 20 min/day | 31.6 | 31.9 | 0.065 |
Table 2: Age, physical characteristics, and mean time spent in VPA of female and male subjects.
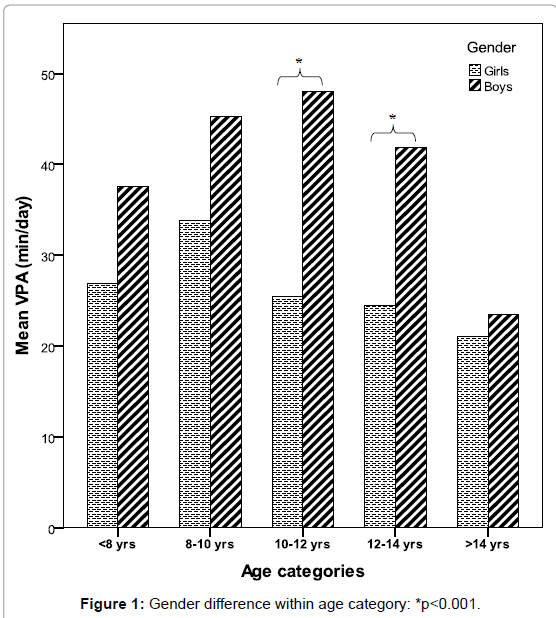
Figure 1:Gender difference within age category: *p<0.001.
PA data interpretation
Data reduction was based on criteria applied in previous publications [14,19-21]. Only periods between 8 am and 9 pm were analysed. Zero activity periods of 20 min or longer were interpreted as being due to unworn accelerometers and were removed from the activity totals [22]. Participants who did not manage to record more than 600 min d-1 of activity[20,21,23-25] for at least 5 days were excluded from further analysis [26]. Data were expressed as total activity counts per registered time (counts.min-1). We used the cut-offs of intensity levels described by Ekelund et al. where sedentary behaviour was defined as less than 500 counts.min-1, light PA from 500 to 1999 counts.min-1, moderate PA from 2000 to 2999 count.min-1, and vigorous PA over 3000 counts.min- 1[14]. Time spent at vigorous PA intensity category was then expressed for all participants as minutes per day.
Statistical methods
Data are expressed as mean and Standard Deviation (SD). A paired Student’s t test with an alpha threshold of 5% was used to analyze the variability of matching characteristics (age and gender) for male and female children participating to the study. A Shapiro Wilk test with an alpha threshold of 5% was used to test the normality of PA variables. As these variables did not have a normal distribution, a paired Wilcoxon test with an alpha threshold of 5% was used to assess differences of PA levels between female and male controls. Statistical differences between age categories were analyzed using Analysis Of Variance (ANOVA) with Bonferroni post-hoc test as well as and covariance (ANCOVA). We evaluated the relationships between dependent and independent variables using unilabiate and multivariate regression analysis. Independent t-test as well as data analyses was performed using STATA 9.2 (StataCorp LP, Texas, USA).
Measure of VPA’s levels
A total of 255 children and adolescents (male; 138; female, 117) with valid PA records were enrolled in the study, whereas 45 participants were excluded to the study for invalid records or device’s dysfunction (15%). Age, physical characteristics, and mean time spent in VPA of all participants are presented in Table 1. Interestingly, we noted that 31.8% of the participants did not accumulate at least 20 minutes of VPA daily, which is considered the minimal cut-off for bone health. When considering the VPA, the time spent in this intensity level decreased significantly with age (t=-2.4, p=0.018).
Determination of gender differences in VPA
Age, physical characteristics, and mean time spent in VPA of female and male subjects are presented in Table 2. There was no statistical difference between male and female groups for age, but males were taller, heavier and had higher BMI than girls. The time spent in VPA was significantly lower in the female group (-31.7%) than in the male group (p<0.001). A reduction in VPA related to age was also observed in males (t=-2.5, p=0.014), but not in females (t=-1.6, p=0.105) (Figure 1). When grouped by age category, male adolescents aged above 14 years (n=31) were significantly less active than younger boys, except the youngster (<8 yrs: n=24, p=0.284; 8-10 yrs: n=18, p=0.020; 10-12 yrs: n=24, p=0.002; 12-14 yrs: n=41, p=0.012). There was no difference among age categories for females (<8 yrs: n=20; 8-10 yrs: n=22; 10-12 yrs: n=27; 12-14 yrs: n=29; >14 yrs: n=19; p>0.05 for all) .Boys aged 10 to 14 years were significantly more active than girls of the same age (Figure 1).
Exploration of the time spent in VPA is relevant as it is currently recognized to reflect high-intensity forces beneficial to skeletal health. The International Consensus Conference on Physical Activity Guidelines for Adolescents recommends that they should be physically active daily and participate in vigorous physical activity three or more times a week for at least twenty minutes[27]. To our current knowledge, there are few studies that have reported VPA measures in a representative sample of healthy children and teenagers. The present project mainly revealed that almost one third of the participants of both genders do not achieve the VPA minimal cut-off for bone health. Although 60 to 80% of the contribution to peak bone mass (PBM) is thought to be genetically determined [28], this finding outlines the fact that many children and adolescents do not reach the optimal level of VPA for maximal bone accretion during childhood and adolescence.
A recent study showed that VPA was related to greater tibial size and thickness, with bone size being 7 mm greater in active subjects than in those with lower VPA level [29]. These same researchers demonstrated also that light to moderate PA was not associated with increased bone mass [29]. Another study comparing BMD in young athletes of different disciplines has demonstrated that that dynamic sports including short, high and multidimensional loads have strong effects on bone formation, independently of training quantity [30]. The current evidence suggests that physical activity should be promoted for bone accretion during childhood and adolescence as well as future skeletal health, but it is beneficial only if children participate in highimpact, vigorous activities [10,13,29-32].
A second interesting result emerged from this study, as this investigation aimed to assess the difference between both genders for VPA. The female participants in our study exhibited a 31.7% lower VPA level in comparison with the males, and this especially for subjects aged between 10 and 14 years. The decrease in physical activity in girls is indeed one of the most persistent findings in the literature concerning the disadvantaged status of females, and gender differences are even larger when considering participation in strenuous sports and vigorous physical activities [10,33,34]. The factors that influence skeletal development and determine gender differences in peak bone mass have been assumed to be related primarily to sex steroid action. For instance, androgens have been reported to increase bone formation particularly incortical areas[35], and the absence of androgen action has been related to lower bone mass and smaller size (5). Androgens also may influence weight and muscle mass, thereby indirectly affecting skeletal development [36]. We may hypothesize that the gender-related differences in bone size and mass are partially related to different types of physical activity, or muscle mass acting on bone mass and geometry. The 30% difference in VPA level observed in our study is significant and could bring, to our opinion, a partial explanation to the difference in bone mineral content that is usually present between both genders.
Finally, our results confirmed that participation in vigorous PA began to decrease at increasingly younger ages, and that the phenomenon probably extents into adulthood. In fact, males were found to begin their decline in VPA after age 12, whereas female began their decline at age 10 even if this difference was not statistically significant. It is also worthy to note that after age of 14, there was no more difference in VPA between both genders. Although other studies have conflicting results as to the age at which VPA levels begin to decline [37,38], results have indicated that VPA rates begin to decrease during early adolescence. Thus, it is particularly important to identify the age at which VPA declines because special intervention programs may be trageted for children of these ages.
There are also some limitations to be considered when interpreting the findings of this study. Firstly, recording the VPA only during 10 days constitutes an instantaneous view of the PA level that could conduct to over- or underestimation of PA in healthy children. Secondly, our recruitment was relatively heterogeneous, in particular in regard to the practice of sport. Even if we are unable to completely rule out the possibility of selection bias, there is no clear reason to believe that children with markedly different PA profiles would have chosen to participate in the study. Thirdly, there are activities during which accelerometers have to be removed (e.g., swimming) or do not accurately measure the intensity level (e.g., cycling). These “unmonitored” activities may result in an underestimation of PA in healthy children. Nevertheless, Trost et al. reported that children’s self-reported periods of “unmonitored” activity added to the registered accelerometer data led to no significant changes in calculated PA levels [36]. In addition, these “unmonitored” activities are not recognized to generate high-intensity forces. Fourthly, to obtain 10 days of measurement recording, activity counts were averaged using a 1-min epoch to ensure that the accelerometer memory capacity was not exceeded. However, this method underestimates VPA as such activity is rarely sustained for longer than 1 min [25]. Although previous studies have demonstrated that VPA may be substantially underestimated [37], this is unlikely to be of importance in this study when analysing age and gender differences in the same cohort.
Vigorous PA measured by accelerometer is a useful and valid tool to assess activities that generate high impact forces in order to induce optimal bone mineral accretion during growth. Firstly, this study provided normative values of vigorous PA in healthy children and teenagers. Secondly, we demonstrated that around 30% of children and adolescents do not accumulate at least 20 minutes of VPA recommended for bone health, suggesting a sedentary lifestyle. We also showed a 30% difference in VPA level between males and females, the latest having less vigorous PA, suggesting that it should be promoted in this high risk group. These findings constitute a starting point for new investigations and further research is needed to establish the relationship between the VPA amount and bone mineral accretion during growth.