Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2014) Volume 2, Issue 1
The incidence of vertebral fractures in patients with osteoporosis is frequent. In elderly patients, the presence of vertebral fracture without history of trauma may be present. In addition, previous diagnosis of tumor pathology raises the suspicion of metastatic disease. The presence of known or unknown primary tumor raises the need for a correct diagnosis to tailor the best treatment. Mechanical pain and neurological compression have been described in both cases. Imaging tests, x-rays, CT and MRI may help the diagnosis. The existence of prior known tumor may not require the need of previous biopsy. Treatment can range from conservative treatment with bracing and analgesia, reinforcement techniques or decompression and stabilization in deformity or neurological deficit.
<Keywords: Non-traumatic; Thoracics vertebral fractures; Malignant tumor
The occurrence of vertebral fractures is not rare in patients with osteoporosis. It increases in older patients with concurrent comorbilities such as neoplasms. A former diagnosis of neoplasia requires a differential diagnosis with vertebral osteoporotic fracture. The clinical onset, a positive previous trauma history, and the imaging studies can help to find a correct diagnosis. Occasionally, the biopsy could not be required. The selection of the appropriate therapy is determined by the clinical course, the age of the patient, the prognosis of the primary tumor and the associated vertebral instability. Numerous treatment options are feasible, grading from conservative therapy with analgesic and spinal orthosis, physical therapy, to spinal decompression and stabilization when neurological symptoms are present. This late option can be suitable in older patients with vertebral osteoporotic fractures or metastatic disease.
A seventy-eight year old woman presented with low back pain of three months of duration, without previous trauma history. On physical examination, she exhibited mechanical pain which exacerbates by standing and walking and improved with rest. She had no neurologic deficit on lower limbs. She was treated for the osteoporosis previously. On her medical records, she had a left hip fracture treated with total hip artrhoplasty and she was diagnosed of an endometroid ovarian tumor five years before, which required radical surgery and chemotherapy. During the follow up she developed pulmonary and hepatic metastasis that resolved with treatment.
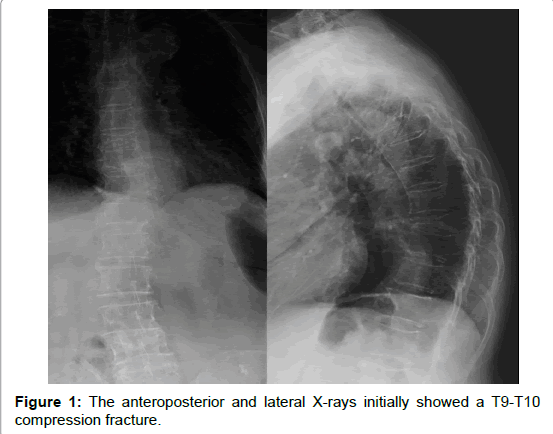
Figure 1:The anteroposterior and lateral X-rays initially showed a T9-T10 compression fracture.
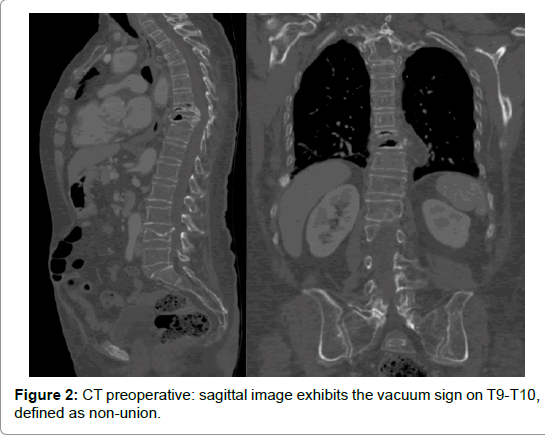
Figure 2:CT preoperative: sagittal image exhibits the vacuum sign on T9-T10, defined as non-union.
In plain AP and lateral radiographs of the thoracolumbar spine, loss of vertebral height in T9 and T10 was seen (Figure 1). The computed tomography demonstrated collapse of vertebral bodies, T9 sclerosis, vacuum sign in T10, and retropulsion of middle column with spinal canal occupation (Figure 2). The MR images were diffuse hypointense in T1 weighted in T9 and T10 vertebrae and confined hiperintense in T2 weighted, localized in T10. In STIR images the posterior ligamentous complex was not involved (Figures 3a-3c). Besides, there was an old compression fracture in L4 and T5 with normal signal.
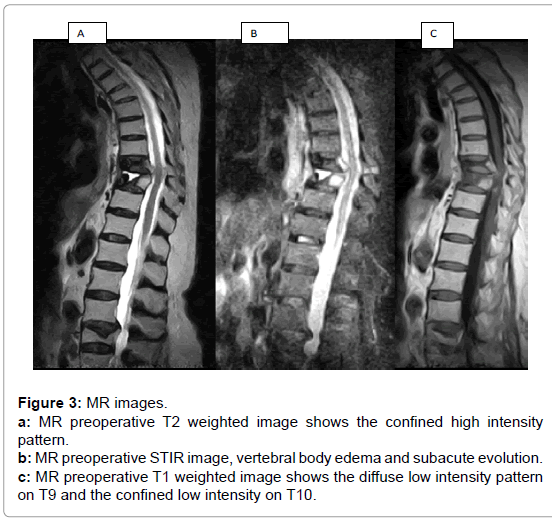
Figure 3:MR images.
a: MR preoperative T2 weighted image shows the confined high intensity pattern.
b: MR preoperative STIR image, vertebral body edema and subacute evolution.
c: MR preoperative T1 weighted image shows the diffuse low intensity pattern on T9 and the confined low intensity on T10.
With the previous diagnose, the patient is informed of the different treatment options, conservative or surgical approach, as well as the complications like progression of metastatic disease or non-responding osteoporotic fracture.
Despite conservative therapy with analgesic, the clinical response was unsuccessfull and surgical treatment is decided. Under general anesthesia, with somatosensitive and motor evoked potentials, and antibiotic prophylaxis the pacient had surgery. The patient lies with lower limbs in extension on a radiolucent table. Posterior approach and instrumentation with fenestrated screws (Expedium, Cortical Fix, Depuy Synthes) and cemented (PMMA, Confidence, DePuy Synthes) from T4 to L1. A right rod was used to prevent from collapse.
A posterolateral left transpedicular decompression was performed. Three centimeter margin of the ribs, facet joints and transverse apophysis were resected at levels affected with T9 and T10 sectioned roots. T9- T10 disc and vertebral bodies were removed. The intraoperatory blood loss was controlled with haemostatic matrix and thrombin. The anterior stabilization was performed with titanium mesh filled with bone allograft, and a bilateral posterolateral arthrodesis was completed. Two grams of Vancomicin were added to the surgical wound. There were no intraoperatory changes on neurophysiologic records. The bony tissue obtained was referred to the pathologist, and was informed as absent of malignant cells.
Osteoporosis is a health problem in the world and a major cause of vertebral fracture in the population. The prevalence of vertebral fractures has been reported to range between 15 and 35% among postmenopausal women [1]. Most patients with such injuries might sustain a low-energy trauma due to poor bone quality. The most of these fractures heals uneventfully with conservative treatment. Surgical treatment of the osteoporotic spine is a treatment of last resort, when all less invasive options have failed. Otherwise, is not uncommon in elderly patients the existence of previous neoplasias [2]. The vertebral localization is the most frecuent osseous involvement. In more than 20% of the cases it is the first clinical manifestation. Breast cancer is the most frecuent cause.
Kaneda et al. have revealed an increase in the incidence of the late appearance of collapse in vertebral fractures. They showed that vertebral collapse is preceded by the necrosis of vertebral bodies caused by changes in microcirculation [3]. Severe lumbar pain gradually diminishes over time due to bone consolidation and an increase in stability. However, the untreatable intense pain associated with neurological symptoms is present in a limited number of cases and can cause severe disability.
Imaging studies should be initiated by anteroposterior and lateral radiographs. The lesion analysis should be completed with CT and/or MR in order to identify the fracture features, explore the stability and rule out other fractures. In this case, we finded vertebral fractures in T5 and L4, with normal signal in MR, that suggests bone consolidation. T5 and L4 vertebral fracture were observed with normal MRI signal indicating bone healing. In some instances a scintigraph and total body CT could be necesary to discard.
Some signs help to predict a poor evolution. On the CT, the affected vertebra showed the cleft sign accompanied by the intravertebral vacuum sign. These two findings are synonymous with the vertebral body osteonecrosis secondary to trauma in patients with osteoporosis or Kummel disease. Furthermore, we can indentify in MR signs that predict a poor progress of the condition, i.e. the T2-weighted images (confined high intensity and diffuse low intensity patterns) which showed a high probability of pseudoarthrosis [4].
The correlation between the fluid sign and the likelihood of osteonecrosis of the vertebral body, in the first 5 months after the trauma, has been described recently. This sign is more especific than the vacuum sign in elderly patients. Other causes of vertebral fracture pathology such as metastasis, infection and multiple myeloma should be ruled out [5]. Recent publications consider MR the best method to distinguish compression vertebral fracture and metastatic involvement. In this case, the absence of paraspinal mass, posterior element and pedicle involvement, complete replacement of marrow, epidural mass, and posterior vertebral border diffuse convexity in the MR are in favor of a benign lesion [6].
Most osteoporotic vertebral fractures can be treated conservatively with analgesic therapy and orthosis. In acute and subacute fractures with persistent pain, vertebral augmentation techniques such as vertebroplasty or kyphoplasty are commonly used, providing fast pain relief with a simple procedure in the early six weeks [7-10].
Nevertheless, in subacute or cronic fractures, the involvement of two adjacent vertebral bodies, the presence of vacuum sign and MR images that suggests fair evolution, as well as neurologic risk could be an indication of surgery. The principles of surgery treatment include decompression of neural elements, deformity correction and stabilization.
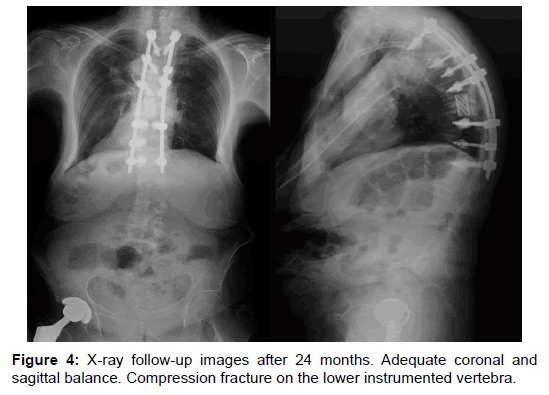
Figure 4:X-ray follow-up images after 24 months. Adequate coronal and sagittal balance. Compression fracture on the lower instrumented vertebra.
Several treatment options have been reported such as anterior decompression and stabilization, posterolateral decompression combined anterior and posterior procedure [11]. In recent years, subtotal corpectomy, decompression, and anterior support with titanium fixed mesh, expandable cage or PMMA reconstruction can be completed through the posterior approach thus avoiding the morbidity of an anterior or combined approach. Several reports have demonstrated the effectiveness and success of this procedure in patients with primary spinal tumors, metastasis, trauma and infection [12-16]. Multiple anchor points distribute corrective forces over a greater number of segments associated with cemented screws minimize risk of loosening and pull out of conventional pedicle screw [17-19]. We noticed a previously non reported complication: a vertebral collapse in T12 without clinical relevance.
The short fixation has been suggested for posterior fusion, but it is important a proper reconstruction of sagittal and coronal profiles, as long as many patients with osteoporosis have already a posttraumatic regional kyphosis secondary to a previous vertebral fracture. In our case, the patient had an old T5 fracture.
Within the literature, the incidence of surgical site infection after adult spine surgery knows a wide variety from 0.7% to 12.0% [15]. Sweet et al. in a retrospective cohort study were able to reduce infection rates at 2.6-0.2% by local application of vancomycin powder [20]. However, in the last years, Enterococcus spp. have become an important cause of nosocomial infections. They are responsible for almost 10% of healthcare related infections and Enterococcus is mainly related to infections of surgical location (14.5%) [21]. In particular we can emphasize Vancomycin-Resistant Enterococci (VRE) or Glycopeptide resistance in Enterococcus spp. It is a clinical problem because of the rapid dissemination of these microorganisms, possible transfer of vancomycin resistance to more virulent pathogens, such as Staphylococcus aureus, and the limited therapeutic possibilities for the infections they cause. Thus, VRE have become a major clinical problem [22].
At two year follow up, the patient keeps excellent clinical and radiologic scores (Figure 4). She walks without aids and doesn´t need analgesics. She has started an bone resorption inhibitor treatment.
Although the osteoporotic vertebral fracture has a benign clinical course, is important to determine when it has not. The persistence of pain and the alteration in clinical images are suggestive of fair outcomes. In absence of contraindications, the surgical treatment in selected patients, can be an approppiate option.