Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 4
Since the FDA approved sorafenib use for thyroid cancer, administration of this medicine to thyroid-cancer patients had steadily increased. However, an appropriate starting dose for this treatment has not been established, which is problematic because the sorafenib discontinuation rate due to toxicity is higher among thyroid cancer patients than among patients with other solid tumors. We recently treated a papillary thyroid cancer patient who experienced a dramatic improvement after being treated with a 400-mg starting dose of sorafenib. Herein, we describe this case and discuss its implications for an appropriate sorafenib starting dose for thyroid cancer.
<Differentiated thyroid carcinomas (DTCs) are usually cured with surgery and adjuvant radioactive iodine (RAI) therapy. However, 7– 23% of DTC patients have distant metastases, and two-thirds of these carcinomas advance to RAI refractory disease [1,2]. There were no alternative treatment options for radioiodine refractory thyroid cancer until sorafenib was approved to treat advanced DTC.
Sorafenib is an oral Tyrosine-Kinase Inhibitor (TKI) with multiple targets, including RET, VEGFR2, VEGFR3, Flt3, c-kit, and BRAF. It has long been used to treat advanced hepatocellular and renal cell carcinomas. The DECISION trial, which investigated the efficacy of sorafenib for RAI refractory advanced or metastatic DTC, showed significantly prolonged progression-free survival in the sorafenib group compared to the placebo group (10.8 months vs. 5.8 months, Hazard Ratio (HR) 0.59, 95% Confidence Interval (CI) 0.45-0.76; p<0.0001) [3]. Based on these results, the United States Food and Drug Administration (US-FDA) approved sorafenib to treat advanced RAI refractory DTC.
The recommended starting dose of sorafenib is 800 mg/day. Despite the positive outcomes from sorafenib treatment for RAI refractory advanced DTC, a high proportion of patients discontinued therapy or reduced their dosage because of toxicity. In the DECISION trial, only 33.8% of patients in the sorafenib group did not experience a dose interruption. According to a systematic review of all phase-II sorafenib trials, 72% of patients could not tolerate an initial dosage of 800 mg and required a dose reduction. The most common reduced dose was 400mg/day [4].
Recently we treated a patient who experienced a dramatic improvement in her papillary thyroid cancer after receiving sorafenib at a 400 mg starting dose. Herein, we describe her case and offer a literature review of sorafenib starting doses for patients with DTC.
A 67-year-old female visited our outpatient clinic with a large anterior neck mass (Figure 1). Approximately 20 years prior, she underwent a right thyroid lobectomy at another hospital. Approximately 11 years prior, she visited our hospital for a left thyroid mass. At that time, total thyroidectomy was performed and she was lost to follow-up. Four years after her thyroidectomy, the patient underwent neck-mass excision and lymph-node dissection surgery two times in a single year. Another four years later, she underwent surgery one more time for a neck mass. Finally, three years after that, she visited our outpatient clinic as described in this case. After each admission, she did not follow-up with the hospital. She never received radioiodine therapy because of her poor compliance.
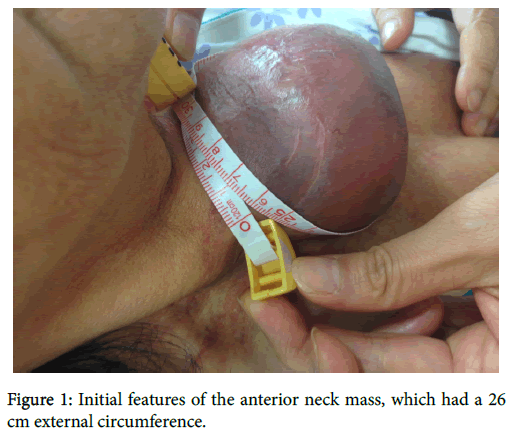
Figure 1: Initial features of the anterior neck mass, which had a 26 cm external circumference.
Initial neck and chest computed tomography (CT) images showed a large anterior neck mass and an extension at the mediastinum. The neck mass size at its largest dimensions was 9.2 cm × 7.8 cm. The mediastinal mass was 10 cm × 6.3 cm (Figure 2). Positron emission tomography–computed tomography (PET-CT) images revealed both neck and axillary lymph nodes (Figure 3). There were no other bone or lung metastases. The patient’s initial thyroglobulin (Tg) level was higher than 50000 ng/mL (reference range, 1.4-78). TSH and Free T4 were 0.025 μIU/ml (0.55-4.78) and 1.25 ng/dL (0.78-1.54), respectively.
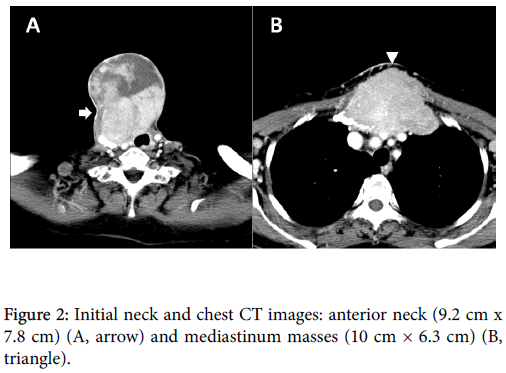
Figure 2: Initial neck and chest CT images: anterior neck (9.2 cm x 7.8 cm) (A, arrow) and mediastinum masses (10 cm × 6.3 cm) (B, triangle).
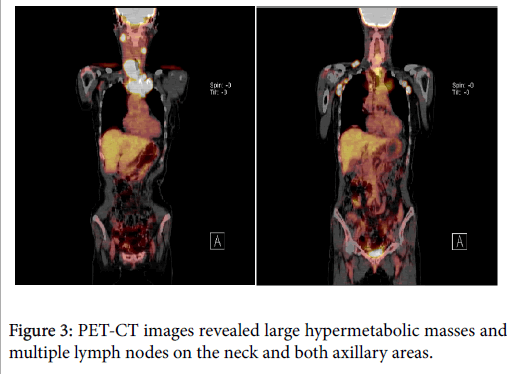
Figure 3: PET-CT images revealed large hypermetabolic masses and multiple lymph nodes on the neck and both axillary areas.
We initiated a sorafenib regimen of 400 mg/day (200 mg twice a daily), with the original intention of controlling cost: At that time, the Korean National Health Insurance did not cover targeted therapy for DTC. After starting the patient on sorafenib therapy, her anterior neck mass gradually decreased for up to 9 months (Figure 4). Seven months after initiating treatment, her serum Tg level had decreased to 248.7 ng/mL and the patient did not experience any severe adverse effects. She did experience a mild case of hand-foot syndrome, but it resolved rapidly.
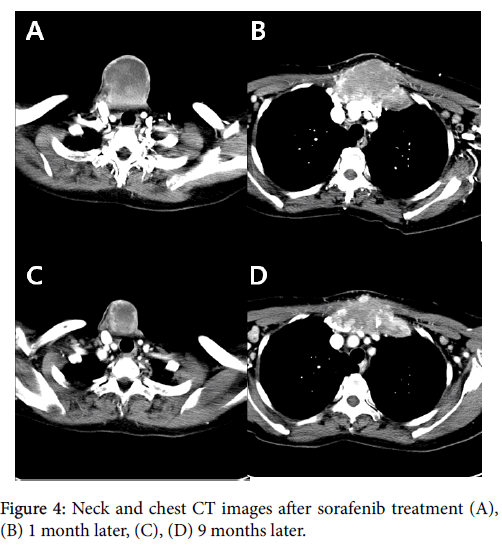
Figure 4: Neck and chest CT images after sorafenib treatment (A), (B) 1 month later, (C), (D) 9 months later.
Four months after initiating sorafenib at 400 mg/day, the Korean government approved coverage of this targeted therapy, so we increased her sorafenib dose to 800 mg/day for 2 months. During this period, the patient suffered from severe diarrhea, alopecia, anorexia and generalized weakness. Thus, after 2 months, the patient chose to decrease her sorafenib dose back to 400 mg/day. She continues to manage her disease, which has remained stable, with a daily sorafenib dose of 400 mg.
Sorafenib was recently approved by the FDA for DTC patients with RAI-resistant distant metastases. The National Comprehensive Cancer Network and the American Thyroid Association guidelines also recommend targeted therapy for patients with RAI refractory metastatic DTC [5]. The Korean National Health Insurance has covered sorafenib for DTC since November 2014 and, since this time, the number of patients who are taking sorafenib for DTC has steadily increased. However, the appropriate sorafenib starting dose for thyroid cancer patients has not been evaluated. The starting dose for solid tumors is 800 mg daily (400 mg twice daily), which was based on recommendations from phase I trials [6-8] that included no thyroid cancer patients.
Tolerability of sorafenib in patients with thyroid cancer is very poor. In a phase II trial of sorafenib, dose reduction and drug discontinuation occurred in 56% and 16% of patients, respectively [4]. In a phase III trial, higher numbers of patients required dose reduction (64%) or discontinuation (19%) [3]. These numbers are much higher than those for other solid tumors that are typically treated with sorafenib. In patients with renal cell carcinoma, the discontinuation, dose-reduction, and drug interruption rates were 10%, 13%, and 21%, respectively [9]. Similar rates were shown in patients with hepatocellular carcinoma (11%, 26%, and 44%, respectively) [10].
Recently, two studies on low-dose sorafenib for thyroid cancer were published. One was a small study of nine Asian patients who were taking a 400-mg daily dose of sorafenib for DTC. The efficacy was comparable to the phase II and phase III trials described above. The response rate was 77% (7/9 patients, 3 patients had a Partial Response (PR) and 4 patients had Stable Disease (SD) by RECIST). Mean Progression-Free Survival (PFS) was 42 weeks, which was shorter than those seen in other trials. However no patients discontinued the drug or adjusted their drug dose because of drug-related toxicity [11]. The other study was a retrospective study of 75 patients receiving sorafenib for thyroid cancer. Twenty-four patients were started on a dose <800mg and 51 patients were started with a 800 mg dose of sorafenib. No significant differences in PFS were noted between the two groups (8 months vs. 10 months), however, the rate at which patients chose to discontinue sorafenib use due to intolerable toxicity was lower in the low-dose group than in the full-dose group (9% and 21%, respectively) [12].
Based on these studies, we concluded that a low starting dose of sorafenib is probably the best approach for treating thyroid carcinoma. Almost no patients in these studies had serious symptoms, despite having metastasized disease or a very large mass. In the case discussed here, the patient had no critical symptoms associated with her cancer, with the exception of a cosmetic problem. Patients with metastatic DTC may not be able to tolerate the adverse side effects of sorafenib treatment because their cancer is associated with fewer uncomfortable symptoms compared to other malignancies, such as renal cell or hepatocellular carcinomas.
Therefore, we suggest that a lower starting dose is the better approach for treating thyroid cancer with sorafenib; if well tolerated, the dose can be increased. Although this case is not unusual, it provides the opportunity to discuss the important issue of sorafenib starting doses for DTC; nevertheless, a prospective randomized controlled trial is needed to establish clearer conclusions.