Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2018) Volume 8, Issue 2
Pancreatic exocrine cancer (PEC) is a challenging disease with a very low of curability rate, even when disease is at early stage and surgically treated, with dismal 5-years survival rates. Advanced disease is always a fatal disease and case of long lasting survivors are very few and doubts on the faithfulness of the diagnosis are more than justifiable. There are some benign illness that can mimic radio-logically and clinically an advance pancreatic cancer? We describe a case of clinically and radio-logically advanced pancreatic cancer who had non diagnostic fine needle aspiration biopsy (FNAB) with a long lasting remission after a short course of therapy with gemcitabine. The atypical outcome after systemic therapy and doubts on reliability of the clinical diagnosis carry us to review literature in search of similar cases, under the point of view of positive outcome and misleading clinical presentation.
Keywords: Pancreatic; Exocrine; Pulmonary; Metastatic
PEC is a frequent cancer both in women and men representing in United States about the 3.1% of all cancer diagnosed [1]. Curability rate are very low even when disease is at an early resectable stage with a 5-years overall survival. The 5-year survival rate for people with stage IA pancreatic cancer is about 14%. For stage IB cancer, the 5-year survival rate is about 12%. For stage IIA pancreatic cancer, the 5-year survival rate is about 7%. For stage IIB cancer, the 5-year survival rate is about 5%. The 5-year survival rate for stage III pancreatic cancer is about 3%. Stage IV pancreatic cancer has a 5-year survival rate of about 1%. Still, there are often treatment options available for people with this stage of cancer [2].
Standard systemic therapy depends from patients performance status and the objective of therapy (neaodjuvant or palliative) and is usually based in the palliative setting on gemcitabine that in pivotal studies gave a benefit in quality of life (and a benefit in overall survival when combined with albumin bended paclitaxel [3,4]. A more aggressive combination is taken in consideration when a cytoreductive aim could carry out too radical surgery [5].
PEC survivors are very few in particular among those diagnosed with an unresectable disease, we report the case of a woman who had a clinical diagnosis of advanced PEC not histologically confirmed because of a negative/non-diagnostic FNAB and in remission after a short course of chemotherapy with gemcitabine.
The facts date back to the spring of 2014 when the female patient aged 69 was diagnosed with a mass of pancreas with loco regional adenopathy and pulmonary thickening at ground glass, general conditions fair, not pain, important weight loss in recent months. As Ca 19-9 was slightly higher than normal, eco-guided FNAB was thus recommended. Co-morbidity factors included bronchiectasies (20 cigarettes/day smokers) and prior cardiac infarction. The histological examination of the fragment from the mass of pancreatic head reported presence of single fragment of skin, minute fragments of pancreas exocrine without atypical elements and blood material. Patient was supposed to undergo a re sampling but after discussion with the clinician it was decided to start chemotherapy with gemcitabine due to the rapid worsening of clinical conditions. Ca 19-9 was 110 U/ml. The treatment started in our clinics on May 2014, from May to September 2014. The patient received 9 total doses of gemcitabine with various interruptions and suspensions for hematological toxicity. TC imaging showed a partial response in July 2014, as shown in Figure 1, and a further TC performed in November 2014 confirmed regression of pulmonary thickening with stable pancreatic pattern. However improvement was observed compared to the findings of April 2014. The patient then due to the bad chemotherapy tolerance entered follow-up which was regular. A TC performed in May 2015 showed no more evident disease and this condition was confirmed in a more recent TC control of November 2017, as shown in Figure 2, Ca 19-9 was table around values of 45-50 U/mL.
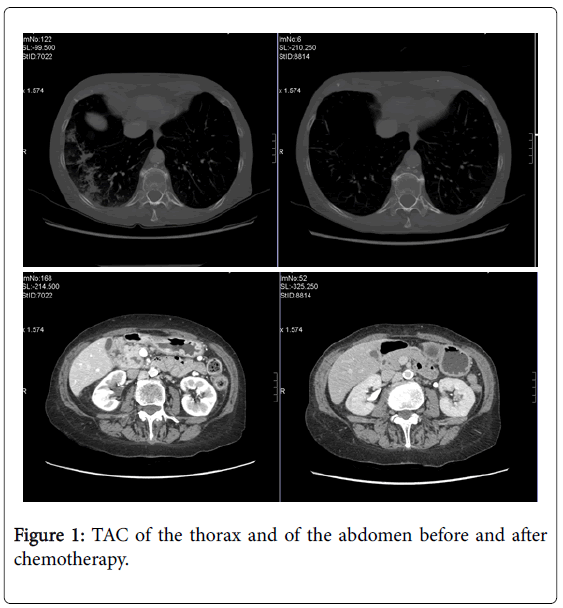
Figure 1: TAC of the thorax and of the abdomen before and after chemotherapy.
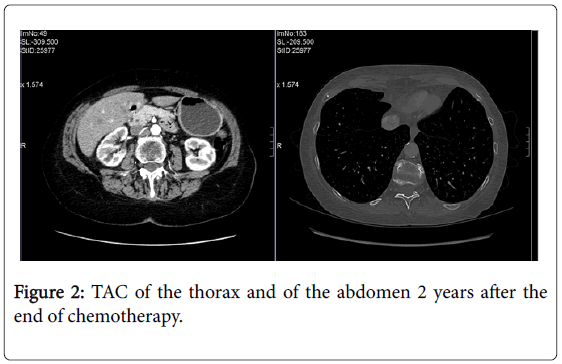
Figure 2: TAC of the thorax and of the abdomen 2 years after the end of chemotherapy.
Our patient is still alive and free of progressive disease after 42 months from the end of chemotherapy with a complete remission as best response. Despite the attempt to have a histological diagnosis that failed we decided to start treatment on the basis of clinical presentation and the presence of a heavy symptomatic disease not ameliorating with beast supportive care.
EUS or TC guided FNAB have generally a sensitivity, specificity and an accuracy ranging respectively from 64 to 94%, 71 to 100% and 78 to 95% [6], with the standard risk of a deep abdominal puncture as bleeding, bowel perforation and infection. Thus, in case of a negative or non-diagnostic FNAB, it is not always possible to repeat the exam due to the further loss of time to start therapy particularly in very symptomatic patients. Most of the oncologists are probably confident in starting a systemic therapy in presence of a likely clinical diagnosis of PEC especially in a heavy symptomatic patient. On the other hand the radiological imaging, even if PET is enhanced, are not able to give a reasonable certain diagnosis and the clinical decision when evidences are lacking are often left to the oncologist who manages the patient [7].
The analysis of a mono-institutional series of 544 patients with unresected PEC who underwent chemotherapy from 1995 to 2009 revealed a 5 years overall survival rate of 2%, with 11 patients still alive but dying sometime after of disease progression, mostly systemic. All these patients had histological diagnosis of PEC and a median CA 19-9 level at start of disease was of 72 U/ml [8]. Interestingly our patients had a low Ca 19-9 level on the onset of disease. The latter could serve as a good prognostic factor to be confirmed by analysis of bigger data sets. As previously reported, the levels of Ca 19-9 at the onset of the disease may represent an interesting prognostic factor [9]. Spinelli et al. reported a case of a long term survivor with more than 10 years after diagnosis of PEC with metastatic disease, but unfortunately there is no mention of Ca 19-9 levels [10]. Another published series of cases investigated the rate of long term survival of patients who underwent surgery. Out of 182 resected patients, 8 were alive at 5 years with one patient lining up to 9.5 years with a median overall survival of 6.4 years, and again no mention of median Ca 19-9 levels [11]. In conclusion rare long time survivors to metastatic PEC may exist. It is not always possible to obtain a histological diagnosis of PEC and PEC diagnosis is also uncertain only on the basis of radiological imaging. Our patient is still well and free from progression after 42 months from the end of therapy even if some doubts remain on the real cause of what underlies clinical condition and radiological imaging on the onset of the disease.