Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2014) Volume 2, Issue 2
Osteoporosis is a disease characterized by skeletal fragility and a consequent increase in fracture risk. Due to this, osteoporosis is one of the top five conditions causing disability and lengthening hospital stay in the elderly population. Thus, with the global increase in elderly population there will be an enormous rise not only in the economical burden, but also in morbidity and mortality. Therefore, osteoporosis has become a major worldwide public health concern. The key strategy for the prevention of osteoporosis is to maximise bone accrual during childhood and adolescence. Knowledge and health beliefs affect whether preventative behaviours are practiced. This study aimed to assess knowledge and health beliefs about osteoporosis in 16-18 year old students in Malé in the Maldives and to determine preferred sources of health information. A cross sectional questionnaire survey of full time secondary school students between the ages of 16-18 years attending four schools in Malé, the main island in the Maldives was undertaken. A previously validated self-administered questionnaire with minor modifications to suit the local population was distributed to 500 student volunteers. There was a 95% response rate (473/500) with one hundred and sixty four questionnaires (93%) (464/500) were suitable for analysis. Sixty per cent of the participants (n=281) had not heard or read anything about osteoporosis. The mean risk factor knowledge score was 7.05 out of a possible 19 points. More than 50% of the participants had a low level of concern about getting osteoporosis and 71% of the participants did not believe that they were susceptible to the disease. The preferred modes of education and sources of information included the internet and talks from health practitioners. The results suggest that 16-18 year old students in Malé have a low level of knowledge of osteoporosis and perceived the threat of osteoporosis as also low. This indicates that this population is unlikely to be practicing the healthy behaviours required to prevent osteoporosis. The results suggest that education programmes directed towards the health education needs is required. Consideration should be given to the use of the internet and face to face delivery.
<Keywords: Osteoporosis; Peak bone mass; Knowledge; Health beliefs; Risk factors; Health education; Asia
Osteoporosis is a common metabolic disease characterised by low bone mass and microarchitectural deterioration [1]. The microarchitectural deterioration coupled with reduced mineralisation leads to decreased mechanical strength, thus making the skeleton more likely to fracture [2]. It is estimated that by 2050 there will be approximately six million osteoporosis related hip fractures worldwide, with 50% of all hip fractures occurring in Asia [3]. Recently published research suggests that degenerative bone and joint conditions are expected to impose an increasing burden on community health services in the Maldives [4].
Previous research has identified that the current adolescent generation in the Maldives undertake a very low level of physical activity [4]. Additionally calcium intake has been found to be low [4]. The research also revealed that 50% of individuals aged 15-20 had a Body Mass Index (BMI) in the undernourished or borderline undernourished zone with a significant percentage of women in the Maldives having a relatively later age of menarche [4]. These findings indicate that people in the Maldives are vulnerable to osteoporosis, and strategies need to be implemented to promote physical activity and healthy eating amongst children in the Maldives.
Knowledge and health beliefs such as perceived susceptibility and seriousness of a disease are considered an important aspect of disease prevention as they are thought to affect behaviour [10]. Several studies have assessed knowledge, lifestyle and health beliefs of osteoporosis, yet much of this work has either been undertaken in the United States of America (USA) or the United Kingdom (UK) where knowledge and education may vary considerably from that in other parts of the world. Little is known in developing countries such as the Maldives where populations may be at risk [11-14].
The objectives of this study were to establish the baseline knowledge and perceptions of osteoporosis amongst 16-18 year old students in Malé, Maldives, and to compare the data with previously collated data from the UK and USA. A further objective was to determine preferred modes and sources of educational information.
Study Design
A cross sectional questionnaire survey was undertaken. Several questionnaires have been developed in order to explore knowledge and beliefs concerning osteoporosis. The Multiple Osteoporosis Prevention Survey (MOPS) developed by Kaspar and colleagues was selected as the most appropriate as it had been shown to be valid and reliable for a similar age group in the USA and has also been used for a study of 16-18 year old School students in the UK [11,14]. As the original questionnaire was designed for use with females in the USA in the early 1990s, minor modifications were necessary to make the questionnaire appropriate for a contemporary mixed gender, population growing up in the Maldives. The changes were:
Question 2: ‘buses or trains’ was removed from the possible list of sources of information, because these forms of transport are not used in the Maldives.
Question 3: ‘Alzheimer’s Disease’ was removed from the list of diseases, as the purpose of this question is to compare osteoporosis with diseases commonly talked about and Alzheimer’s disease is not well known in the Maldives.
Ethical approval and access
Ethical approval for the research was sought and obtained from the University of Hertfordshire School of Health and Emergency Professions Ethics Committee, UK. The Ministry of Education, Maldives, was contacted to obtain access to approach the schools and the official process required for contacting students. The Head Teachers of the appropriate schools were contacted to seek access to the students and to distribute the questionnaires. Access was granted from the 4 largest schools in Malé, Maldives.
Sampling and sample size
There were 3219 enrolled fulltime students in the Maldives between the ages of 16 and 18 in both public and private schools. A sample for the research was drawn from the capital of Maldives, Malé, where 57% of the student population is aged between 16-18 years [12]. Inclusion criteria were that the participants were in fulltime education, aged between 16-18 years and able to read and write English. A sample size of 500 was used in the study. This represents 26.82% of all students within this age group. Stratified sampling was used to ensure appropriate representation from each school was achieved, as the total number of students was different in each of the schools.
Questionnaire distribution
The questionnaire was distributed to the students in class either by the chief investigator (UN) or by an advocate teacher. Students were given 10-15 minutes to complete and post their questionnaires in a box which was collected later by the chief investigator. Questionnaires were anonymous, identifiable only by school attended and gender. The questionnaires were distributed in the participating schools within a one month time frame.
Data management and analysis
Data was entered into Microsoft Excel and later transferred to the Statistical Package for Social Science (SPSS), version 17 where further descriptive statistics were undertaken. In light of the multiple comparisons being made tests were considered significant when the P value was 0.01 or <0.01.
A 95% response rate was achieved 473 out of 500 questionnaires. Non respondents were not followed up. Nine questionnaires were incomplete and therefore were discarded which left 464 suitable for analysis. The age range of the participants was 16-18 years with a mean age of the 17.2 years. One hundred and ninety males and 274 females completed the questionnaire.
Sixty percent of the participants (n=281) had not heard or read anything about osteoporosis (Question 1). Of the 183 participants who reported that they had heard or read some information about osteoporosis, 131 participants answered an open question ‘what do you understand by it?’ The answers were post coded using the enumeration process and thematically analysed into categories for descriptive analysis. Of those students that knew something about osteoporosis, 40% thought it was diet related, 21% and 16% thought it related to fracture and age; while just 3% thought it was related to being female and the menopause and 2% thought it was genetic.
Participants indicated from a list, the sources of their knowledge of osteoporosis (Question 2). The most frequently identified source were ‘School’, ‘Television’, ‘Relative, friend or neighbour’ by female participants while ‘Television’, ‘School’ and’ Internet’ were most frequently cited by the males.
Questions 3 asked, ‘How concerned is the participant of getting osteoporosis and other pathologies?’ Responses to this question were grouped into 2 categories. Those who responded 1 or 2 indicating they felt little or no concern about a particular pathology and those who responded 3 to 5 indicating they were at least moderately concerned. The mean level of concern of the participants for getting osteoporosis was 2.49 for males and 2.31 for females and the median level was 2 for both genders (Table 1). The Wilcoxon signed-rank test was used to test for statistically significant differences between levels of concern about getting osteoporosis and other diseases (Table 2). Significance levels were set at p=0.001. Males were significantly more concerned about being affected by heart disease than developing osteoporosis. Females were significantly more concerned about developing heart disease, cancer, HIV/AIDS and the common cold when compared to osteoporosis.
Seventy one per cent of participants (n=32) did not believe that they were susceptible to the disease (question 4), although 86% (n=389) of participants felt osteoporosis to be a serious disease (question 5). Cross tabulation was used to identify associations between levels of concern, perceived susceptibility and perceived seriousness (Table 3).
| Pathology | Median | Mean | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Osteoporosis | 2 | 2 | 2.49 | 2.31 |
| Heart Disease | 3 | 3 | 2.86 | 2.86 |
| Cancer | 2 | 3 | 2.56 | 3.00 |
| HIV/AIDS | 3 | 3 | 2.84 | 2.90 |
| Common Cold | 3 | 3 | 2.96 | 3.03 |
Table 1: Mean and median scores for concern for developing common pathologies.
| Pathology | Wilcoxon Signed Rank Test (p values) | |
|---|---|---|
| Male | Female | |
| Heart Disease | 0.003 | < 0.001 |
| Cancer | 0.777 | < 0.001 |
| HIV/AIDS | 0.096 | 0.012 |
| Common Cold | 0.154 | 0.004 |
Table 2: Concern about getting osteoporosis when compared to other common pathologies.
| Concern for Osteoporosis | |||||
|---|---|---|---|---|---|
| Low concern | High concern | ||||
| Likelihood of getting Osteoporosis | Likelihood of getting Osteoporosis | ||||
| Low | High | Low | High | ||
| Seriousness | Low | 42 (10%) | 166 (37%) | 8 (2%) | 3 (1%) |
| High | 11 (2%) | 33 (7%) | 100 (23%) | 81 (18%) | |
Table 3: Cross tab analyses of participants concern, likelihood and seriousness of osteoporosis.
| a. Drinking alcohol in excess b. Being Caucasian c. Infrequent or skipped menstrual periods d. Drinking caffeine in excess e. A family history of osteoporosis f. Eating a diet high in animal fat g. Lack of physical exercise h. Being Black i. A diet low in dairy products j. Taking steroids or thyroid medication k. Having a thin or small frame l. Worry or anxiety m. Being Asian n. Being postmenopausal o. Having high blood cholesterol p. An early or surgically induced menopause q. Getting sunburn r. Smoking cigarettes |
Table 4: List of risk factors for osteoporosis.
Question 6 asked participants ‘How responsible do the subjects feel one is for getting osteoporosis and other pathologies?’ Sixty four per cent of the participants reported a moderate to high level of responsibility for developing osteoporosis. This was only surpassed by their reported responsibility for developing HIV/AIDS and heart disease, 88% and 80% respectively.
Question 7 assessed the participant’s knowledge of risk factors (Table 4). The average score for males was 6.63 and 7.34 for females out of a possible 19. The combined male/female score was 7.5. Fifty seven per cent of participants highlighted that a diet low in dairy products or other sources of calcium were a risk factor. However, only 43% (199/464) identified that a lack of physical activity was a risk factor. Just 16% (74/464) identified being Asian as a risk factor. Three risk factors related to menstruation and the menopause. One hundred and ninety eight (198/274) (83%) of the females did not identify infrequent or skipped menstrual periods as a risk factor for osteoporosis. One hundred and sixty four of the 198 females who answered the question (83%) did not identify being post-menopausal as being a risk factor for osteoporosis while 141 of the 164 females who answered (86%) did not identify early or surgically induced menopause as being a risk factor.
The final question asked participants to s elect and rank from a list the sources which they would most likely use to learn about osteoporosis. The most likely source of information to be used by both males and females were the computer/internet and talks by health practitioners. Internet examples included Facebook, Google and WHO website (Figure 1).
The majority of the participants (60%) reported they had heard or read nothing about the Osteoporosis. Amongst the females, 34% reported that they had read or heard nothing about osteoporosis. This finding was similar to that found amongst adolescents in Egypt very recently whereby 38% of the studied sample didn’t know the meaning of osteoporosis [15]. Conversely this finding was far greater than the 10% reported in the USA by Kasper and colleagues and 12% reported by reported by Gurney and Simmonds in the UK and may reflect a general lack of osteoporosis health promotion in Malé and the Middle East [12,14].
Both male and female participants reported a low level of concern for developing osteoporosis. Males were no more concerned about developing osteoporosis than a common cold, testicular cancer or HIV/AIDS. They were however significantly more concerned about getting heart disease than osteoporosis. The results obtained from the males are similar to the findings of Gurney and Simmonds [14]. The female participants in this study showed that they were significantly more concerned about getting breast cancer, HIV/AIDS, heart disease and the common cold compared to osteoporosis. This is different to the findings in the UK and in the USA where female participants were only more concerned about getting breast cancer than osteoporosis [12,14]. The low levels of knowledge and concern about developing osteoporosis may reflect a lack of available information about osteoporosis and health education.
Seventy one per cent of both males and females rated their likelihood of developing osteoporosis as low. Males did not perceive their likelihood of developing osteoporosis as being significantly greater than that of heart disease. The World Health Organisation (WHO), estimates 17.1 million people around the globe die of cardiovascular disease annually, while osteoporosis is estimated to effect 75 million people in Europe, USA and Japan combined [16,17]. Both genders also thought they were no more likely to develop osteoporosis compared to either testicular or breast cancer. It is estimated that the lifetime risk of experiencing an osteoporotic fracture in men is similar to that of developing prostate cancer which is representative of their perception. However, the life time risk of osteoporotic hip fractures in women is 1 in 6, compared with 1 in 9 of a diagnosis of breast cancer [18]. Hence, some of the results of perceived susceptibility do not concur with statistics of actual incidence. This is in agreement with previous research in the UK [14].
The cross tabulation analysis which explored concern, perceived susceptibility and perceived seriousness of osteoporosis showed that the majority of the participants had low levels of concern and perceived susceptibility, but had a high level of perceived seriousness with regards to osteoporosis (Figure 1). On the basis of the Health Belief Model [9], where the individual’s perception of the threat caused by a health problem is thought to affect behaviour, it follows that this population is unlikely to practice healthy behaviour required to prevent osteoporosis.
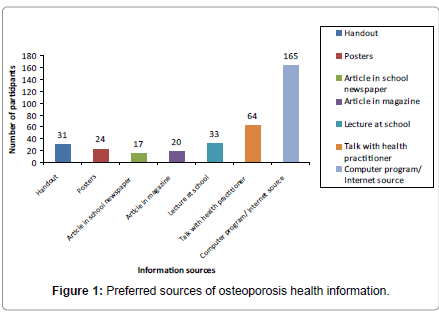
Figure 1:Preferred sources of osteoporosis health information.
According to Orem’s Self Care Theory, knowledge is a necessary element in encouraging healthy lifestyle behaviours [19]. Overall the level of knowledge about osteoporosis and associated risk factors was low. Interestingly, a diet low in calcium was identified correctly by 57% of participants which may reflect a positive impact of health related milk product campaigns [20]. Lack of physical activity was identified by just over 50% of the participants as a risk factor, which was very much lower than the 82% reported in the UK, where physical activity campaigns have been running for several years [14]. Eighty six per cent of the female participants did not recognize any of the risk factors related to menstruation and the menopause. This is concerning, as a significant proportion of individuals in the Maldives have been shown to experience a later age of menarche [4], which can impact on a person’s ability to achieve optimal peak bone mass and subsequent increased risk of developing osteoporosis. Furthermore, just 16% of the participants identified being Asian as a risk factor. Moreover very few participants identified links with genetics and being female. These results strongly indicate that this population do not possess adequate knowledge about the modifiable risk factors to make informed decisions about healthy behaviours to improve bone health [21,22]. As this population has been identified as a high risk group, the results of this study suggest that there is a need for the implementation of health education for the primary prevention of osteoporosis.
A computer program and the internet were the most popular information sources (Figure 1). There is research supporting the desirability of tailored interactive web site as a method of providing education and awareness on osteoporosis [23]. The suggestions given by the participants who marked internet sources included Facebook, Google and WHO website. Social media websites such as Facebook, MySpace and Twitter have been identified as popular sources of health information, as social media marketing has the advantage of rapid transmission through a wide community [24]. Hence, techniques such as attaching links of the authorized websites to the social media websites could be a useful health promoting method and would be worthy of further research. A 5 minute talk with health care practitioners or educators and a lecture at school was also one of the most popular information sources reported by participants and should be considered in health promotion strategies. A recent project entitled ‘The Best Bones Forever’ conducted in three community sites in the United States and targeted for children and adolescents showed significant improvements in most measures of bone health knowledge, attitudes, self-efficacy, behaviours, and intentions [25]. These findings suggest that incorporating bone health messages into related health promotion efforts around healthful eating and physical activity was both feasible and effective and could be considered in communities such as Male´.
The sample frame was relatively small and included only the main island Malé, therefore caution should be taken with regard to generalizing the results to the whole population of 16-18 year olds in Male and the Maldives. Although the participants were fluent in English the spoken language is Dhivehi and there may have been some ambiguity regarding the meaning of Osteoporosis which may have impacted on the results.
This research suggests that 16-18 year old students in Malé Maldives have a low level of knowledge of osteoporosis and have little awareness of associated risk factors. Furthermore they reported little concern about developing the disease, despite perceiving it to be a serious disease. This indicates that at present this population is unlikely to be practicing the healthy behaviours required to prevent osteoporosis. The results imply that education programmes specifically directed towards the health education needs of this population is required. Consideration should be given to the use of the internet and face to face delivery. Appropriately trained health professionals such as physiotherapists, dieticians and nurses working alongside school teachers may be ideally placed to develop and provide such programmes.