Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2013) Volume 1, Issue 2
Objective: Pulsed Electromagnetic Fields (PEMFs) were introduced in the clinical setting in the 1970s. Proven to be a successful method of treating non-union and delayed union of fractures, its effects on cartilage has remained ambiguous. PEMFs have demonstrated a pro-anabolic and anti-catabolic activity on cartilage metabolism. We hypothesized that the use of PEMFs in patients with symptomatic cartilage lesions of the knee would lead to improved clinical outcomes in an observational study to evaluate the results after 2-years.
Methods: 25 patients between the age of 30 and 60 years who underwent treatment with PEMFs for symptomatic cartilage lesions of the knee (grade 1-2 as per ICRS classification) were included in this prospective case series. Patients were evaluated pre-treatment, at 12 months and 24 months using Visual Analogue Scale (VAS) scale for pain, Tegner and KOOS scores.
Results: A significant improvement in all scores was observed at 1-year follow-up (p=0.003). At 2-year follow-up, results deteriorated but were still superior to pre-treatment levels (p=0.04). No adverse reactions were seen.
Conclusions: PEMFs in patients with symptomatic isolated cartilage lesions of the knee can cause improvement in symptoms, knee function and activity in the short term. Repetition of treatment annually may improve the long term results.
<Keywords: Cartilage lesions; Pulsed electromagnetic fields; Knee; Chondral injury; Osteoarthritis
Injuries to articular cartilage can lead to joint dysfunction and progressive joint degeneration with a considerable social impact for the high costs related to treatments and loss of work days. The exact incidence of cartilage injuries is still not well defined. Curl et al. in a retrospective review of 31,516 arthroscopies identified cartilage lesions in 63% of cases [1]. Cartilage has a poor intrinsic healing potential and when left untreated, cartilage lesions can progress rapidly and lead to early onset of Osteoarthritis (OA) [2]. Given that the average life span of man has increased, and a trend towards fitness and athleticism, we now must deal with a population which is either too young, or too fit to undergo metal resurfacing. Research has been directed toward preventive interventions and cost-effective treatments in order to find a way to improve clinical outcomes and retard the progression of OA. Many conservative treatment modalities, such as oral and topical Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), intra-articular corticosteroids injections, visco-supplementation or Platelet-Rich Plasma (PRP) injections, bracing, and physical therapy have a role in selected cases [3-6]. The decision-making is based on patient-related factors (intensity of symptoms, age and functional demand) and characteristics of the lesion (size, location, depth, chronicity).
The use of Pulsed Electromagnetic Fields (PEMFs) has received attention for the treatment of OA and symptomatic focal cartilage lesions of the knee after in vitro and in vivo studies have demonstrated their ability to influence cartilage metabolism through pro-anabolic and anti-catabolic activity [7-12]. PEMFs were introduced in the clinical setting in the 1970s as a successful method for treatment of non-union and delayed union of fractures; the effects on knee OA are equivocal, with few investigations reporting conflicting results [13-19]. The aim of this observational study is to evaluate the outcomes of the treatment with PEMFs in patients presenting with symptomatic cartilage lesion of the knee. We hypothesized that the treatment would lead to relief of symptoms and improved clinical outcomes.
Study group
This is a prospective case series begun in January 2009 until December 2010 with institutional review board approval. A written, informed consent was obtained from all the patients.
53 patients with symptomatic cartilage lesions of the knee were treated with PEMFs at our institute. 25 of them (12 male and 13 female) met our study inclusion criteria and were prospectively followed up for a minimum of 2-year post treatment (Table 1).
Inclusion criteria:
- age between 30 and 60 years;
- grade 2 or 3 cartilage lesion according to the ICRS classification, evaluated by MRI and previous arthroscopy;
- symptomatic with functional limitations.
Exclusion criteria:
- radiographic findings of knee OA (of grade 2-4 as per Kellgren- Lawrence classification) or degenerative changes involving hip and ankle in both lower extremities;
- malalignment of the lower limbs (varus-valgus greater than 8° from physiological);
- knee instability or patello-femoral maltracking;
- previous knee surgery for cartilage or ligaments in both lower extremities when performed within 6 months prior to treatment (including diagnostic arthroscopy, cartilage debridement and meniscectomy);
- previous intra-articular injections with corticosteroid, PRP or hyaluronic acid (within 6 months prior to the study);
| Variables | Data |
|---|---|
| Number of patients | 25 (12 male / 13 female) |
| Mean age | 48.1±2.6 (range: 30-60) |
| Mean follow-up (years) | 2.1 |
| Age ≥ 45 years | 14 |
| Age < 45 years | 11 |
| Single lesions | 20 (8 PAT, 8 MFC, 1 MTP, 1 LFC, 2 LTP) |
| Multiple lesions | 5 (3 LFC/LTP, 2 MFC/MTP) |
PAT: Patella; MFC: Medial Femoral Condyle; LFC: Lateral Femoral Condyle; LTP: Lateral Tibial Plateau; MTP: Medial Tibial Plateau.
Table 1: Patient demographics and localization of cartilage lesions.
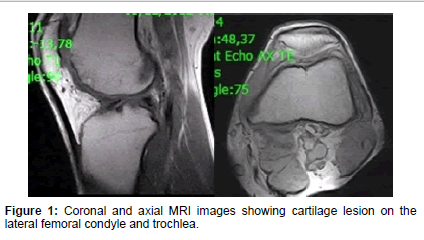
Figure 1:Coronal and axial MRI images showing cartilage lesion on the lateral femoral condyle and trochlea.
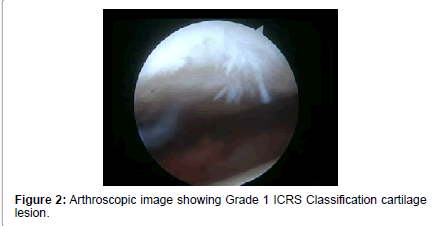
Figure 2:Arthroscopic image showing Grade 1 ICRS Classification cartilage lesion.
- inflammatory arthritis;
- smokers;
- severe cardiovascular disease.
Treatment protocol
All patients underwent biophysical treatment with PEMFs (I-ONE therapy, IGEA S.p.A., Carpi, Italy). The protocol included a 4-hour treatment per day, for a total of 45 days. The treatment could also be divided into 2 applications of 2 hours each, at different times of the day. The maximum intensity of magnetic field was 1.5 mT and frequency 75 Hz.
Data collection and analysis
The standard radiographic pre-operative evaluation included a standing anteroposterior long-leg radiograph (including hips and ankles), standing anteroposterior and 45° flexion views, lateral view of the knees, skyline patellofemoral view, and MR imaging. Visual Analogue Scale (VAS) for pain (0=no pain at all, 10=worst pain), International Knee Documentation Committee (IKDC) objective, Tegner, Knee Injury and Osteoarthritis Outcome Score (KOOS) scores were collected before treatment, and at 1 and 2 year follow-up and analyzed independently by another author. Primary outcomes of the study were Range of Motion (ROM), pain relief, improvement of symptoms and improvement of activity level. The level of patient satisfaction was also recorded.
Statistical analysis
SPSS software (SPSS 17.0, SPSS, Chicago, IL) was used for the statistical analysis. Mean values of KOOS, Tegner and VAS before treatment, at 1 and 2 year follow-up were compared and the statistical significance was calculated with the t-student test with a confidence interval of 95% and significance level of p<0.05.
25 patients were available at final follow-up. Mean age at the time of treatment was 48.1 ± 2.6 years (range, 30-60 years) and average followup was 25 months (range, 24-30 months).
20 presented with single cartilage lesions and 5 with multiple (patient demographics and localization of cartilage lesions are reported in Table 1). Both subgroups were homogenous with regard to OA changes (grade 0 and 1 as per Kellgren-Lawrence classification), number of lesions and previous surgeries.
All patients showed a significant improvement in all scores at 1-year follow-up (p=0.003). At 2 year follow-up, results deteriorated but were still superior to pre-treatment levels (p=0.04) (Figures 1,2 and 3). The mean values obtained in KOOS, VAS and Tegner scores before treatment, at 1 and 2 year follow-up are presented in Table 2. The analysis of IKDC objective score is seen in Figure 4. Average ROM was 7.5-120.0° ± 4.2° before treatment, 0-131.1° ± 2.5° at 1-year follow-up and 1.2-127.2° ± 5.1° at final follow-up.
An analysis of the results in patients under 45 years old revealed better outcomes in this sub-group compared to patients over 45 years of age (Table 3). The difference in Tegner score between the two subgroups was significant (p=0.03). As observed analyzing the overall results, a similar trend with a significant improvement in KOOS, Tegner and VAS scale at 1-year follow-up (p=0.01) and a decline at 2-year follow-up (p=0.04) was also seen in patients under 45 years of age (Figures 5 and 6). No adverse reactions or side effects were seen. At 2-year follow-up 80% of patients were satisfied and willing to repeat the treatment.
Our findings suggest that treatment of symptomatic grade 2 and 3 cartilage lesions of the knee with PEMFs can lead to improved clinical outcomes in the short term. The scores in this evaluation significantly declined at the 24 month follow-up; however, the values were still higher than pre-treatment levels. We believe this is related to a reduction of the anti-inflammatory and chondroprotective action over time and that if treatment were repeated annually sustained improvement could be possible. As a concomitant finding we observed superior outcomes in younger patients below 45 years. The average Tegner score at the 1-year follow-up was 6.1 and was significantly higher when compared to subjects over 45 (average Tegner score 2.9) (Figure 7). However, it can be speculated that this result might be related to the fact that the baseline knee function in patients younger than 45 is higher than patients over 45 years of age; this factor can certainly affect the final score.
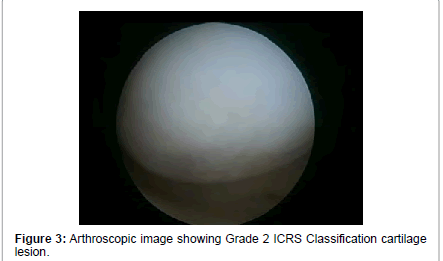
Figure 3:Arthroscopic image showing Grade 1 ICRS Classification cartilage lesion.
| Scale | Pre-treatment (mean ± SEM*) | 12-month follow-up (mean ± SEM*) | 24-month follow-up (mean ± SEM*) |
|---|---|---|---|
| KOOS Pain | 52.3 ± 4.8 | 89.7 ± 4.3 | 73.9 ± 3.4 |
| KOOS Symptoms | 55.4 ± 5.0 | 84.5 ± 3.6 | 72.2 ± 3.7 |
| KOOS ADL | 53.3 ± 5.6 | 90.8 ± 3.4 | 72.9 ± 3.9 |
| KOOS Sport | 28.0 ± 5.9 | 75.4 ± 6.2 | 60.3 ± 5.5 |
| KOOS QOL | 35.6 ± 4.5 | 81.3 ± 4.7 | 66.8 ± 6.1 |
| VAS | 5.5 ± 0.4 | 1.3 ± 0.4 | 2.2 ± 0.6 |
| Tegner | 2.5 ± 0.5 | 4.5 ± 0.5 | 3.8 ± 0.5 |
The variables are expressed as mean ± SEM (standard error of the mean). Abbreviations: VAS: Visual Analog Scale; KOOS: Knee Injury and Osteoarthritis Outcome Score; ADL: Activities of Daily Loving; QOL: Quality of Life.
Table 2: Clinical outcome: overall results.
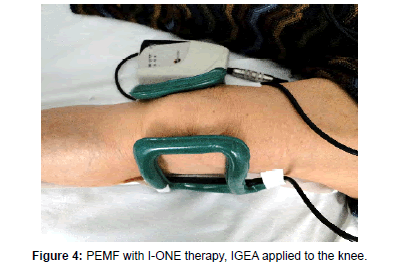
Figure 4:PEMF with I-ONE therapy, IGEA applied to the knee.
| SCALE | Pre-treatment(mean ± SEM*) | 1-year follow-up(mean ± SEM*) | 2-year follow-up(mean ± SEM*) | |||
|---|---|---|---|---|---|---|
| Under 45 | Over 45 | Under 45 | Over 45 | Under 45 | Over 45 | |
| KOOS Pain | 52.6 ± 4.8 | 52.9 ± 3.8 | 93.8 ± 5.3 | 86.2 ± 5 | 78.8 ± 3.4 | 77.3 ± 34.4 |
| KOOS Symptoms | 53.6 ± 4.8 | 54.3 ± 4.8 | 89.1 ± 4 | 85.1 ± 3 | 71.9 ± 4.5 | 76 ± 3.5 |
| KOOS ADL | 54.8 ± 6 | 56.7 ± 4 | 96.2 ± 3.5 | 94.6 ± 2.5 | 80.7 ± 3.1 | 76.8 ± 2.1 |
| KOOS Sport | 31.8 ± 4.8 | 24.2 ± 5.8 | 80.8 ± 7.2 | 78.1 ± 4.2 | 73.3 ± 4.2 | 64.2 ± 2.4 |
| KOOS QOL | 37.7 ± 4.6 | 31.8 ± 4.6 | 83.3 ± 5.5 | 82.9 ± 2.5 | 72.5 ± 6 | 69.6 ± 4 |
| VAS | 5.8 ± 0.5 | 5.4 ± 0.3 | 1.2 ± 0.5 | 1.4 ± 0.3 | 2.1 ± 0.7 | 2.3 ± 0.6 |
| Tegner | 2.9 ± 0.4 | 2.1 ± 0.6 | 6.1 ± 0.5 | 2.9 ± 0.5 | 4.4 ± 0.5 | 3 ± 0.3 |
The variables are expressed as mean ± SEM (standard error of the mean). Abbreviations: VAS: Visual Analog Scale; KOOS: Knee Injury and Osteoarthritis Outcome Score; ADL: Activities of Daily Loving; QOL: Quality of Life.
Table 3: Comparison of outcomes in patients under 45 years old versus over 45 years old: KOOS, VAS and Tegner.
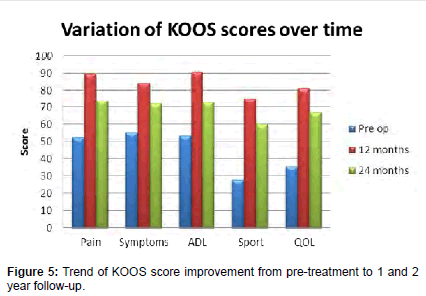
Figure 5:Trend of KOOS score improvement from pre-treatment to 1 and 2 year follow-up.
Prior studies demonstrating the use of PEMFs in patients with OA have reported conflicting results [20,21]. Thamsborg et al. conducted a Randomized Clinical Trial (RCT) (83 patients) and did not demonstrate significant differences in the outcome scores in the group treated with PEMFs compared to a placebo group; while Trock et al. in a RCT that included 86 patients treated with PEMFs versus placebo for knee OA reported significant improvements in symptoms and ADL in the PEMFs group [18,19]. A recent meta-analysis that included nine RCT’s with a total of 483 patients concluded that evidence of a beneficial effect of PEMFs on functional outcomes in patients with knee OA does exist [20]. PEMFs have also been applied in patients undergone knee arthroscopy for cartilage lesions. Zorzi et al. in a RCT evaluating the outcomes of arthroscopic chondro-abrasion or perforation followed by treatment with PEMF showed that the treatment with PEMFs aided patient recovery after arthroscopic surgery, reducing the use of NSAIDs. The use of PEMFs was associated with improved functional outcomes with a long-term effect [21]. These data are in accordance with our findings. However, in our investigation we excluded patients who had undergone knee arthroscopy within 6 months prior to the treatment as we aimed to study if a direct correlation between the use of PEMFs and improvement of clinical outcomes exists. Previous cartilage procedures may in facts present confounding factors and affect our interpretation (Figure 8).
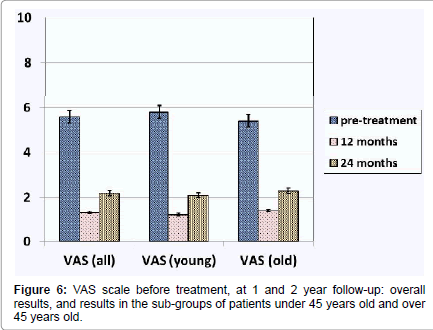
Figure 6:VAS scale before treatment, at 1 and 2 year follow-up: overall results, and results in the sub-groups of patients under 45 years old and over 45 years old.
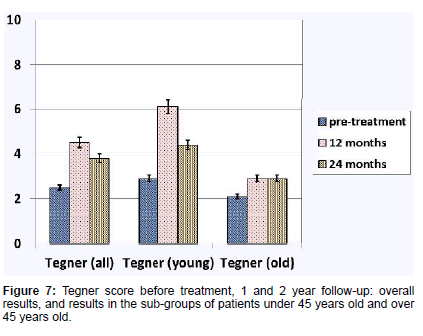
Figure 7:Tegner score before treatment, 1 and 2 year follow-up: overall results, and results in the sub-groups of patients under 45 years old and over 45 years old.
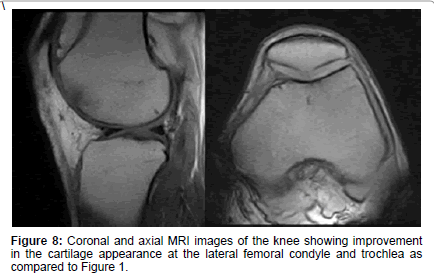
Figure 8:Coronal and axial MRI images of the knee showing improvement in the cartilage appearance at the lateral femoral condyle and trochlea as compared to Figure 1.
The mechanism of action of PEMF’s has been described in several in vitro and in vivo studies [7-12,22]. The anti-inflammatory effect of PEMFs is associated with the modulation of adenosine A2A receptors through up-regulation, as demonstrated in both bovine and human chondrocytes and synovial fibroblast [11,22]. The modulation of these receptors having anti-inflammatory activity is considered to be one of the mechanisms by which the PEMF counteracts the effect of proinflammatory cytokines in explants of cartilage and synovial fibroblasts and prevents the progression of OA [7,11,12]. On the other hand, PEMFs through the synergy with insulin-like growth factor 1 (IGF-1) exerts a pro-anabolic activity enhancing chondrogenic differentiation and synthesis of extra-cellular matrix component, as shown in both human and bovine models [9,10,23]. In vivo studies conducted on Dunkin Hartley guinea pigs showed that PEMFs was able to reduce tissue fibrillation, preserve cartilage thickness and prevent the sclerosis of the sub-chondral bone in lateral and medial compartment of the knee [20,24].
The above-mentioned pre-clinical data represent the rationale for the clinical application of PEMFs as an alternative to the use of NSAIDs or intra-articular injections (steroids, hyaluronic acid, PRP) in the symptomatic treatment of isolated cartilage lesions. In our experience, the use PEMFs is a valid and cost-effective therapeutic approach. It has advantages over the chronic use of NSAIDs or cortisone injections related to the absence of potential side effects [25,26]. Moreover, it is a non-invasive treatment, free of complications, and it is well accepted by the patients. However, there are varieties of PEMFs protocols available, which differ for device characteristics (intensity and frequency of the magnetic field), application intervals and duration of treatment.
A long-term follow-up represents a point of strength in this investigation. All the published articles that investigated the use of PEMF in the treatment of knee OA have a shorter follow-up (between 6 and 12 weeks) [14-19]. Moreover, we used several validated scoring systems in order to obtain information about all aspects of daily living and sport participation. This study has a few limitations - the first being the relatively small sample size; the second is the absence of randomization and a control group. However, we limited the risk of bias by performing a systematic prospective data collection while an independent author reviewed and analyzed the data.
In particular, it will be useful to compare the outcomes of the treatment with PEMFs with other conservative therapeutic approaches such as oral medication (NSAIDs, glucosamine, chondroitin sulfate) or intra-articular injections (steroids, hyaluronic acid, PRP plateletrich plasma). Also, an MRI study comparing pre-treatment and posttreatment findings would be useful in order to investigate if changes occur on a macroscopic level.
PEMF is a valid and useful conservative modality for the treatment of early OA in a young population. Annual repetition of treatment may demonstrate sustained long term benefits.