Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Case Report - (2013) Volume 1, Issue 2
Neoplastic transformation of lymphocytes involves a multitude of genetic alterations that result in clonal expansion. Cognate activation of lymphocytes against foreign and self antigens similarly results in clonal expansion and there have been prior reports of simultaneous clinical presentations of lymphomas and autoimmune disorders. In this case report, we report a rare collision of an indolent B cell lymphoma with a MLH1- negative microsatellite unstable colon cancer. We present a hypothesis whereby repeated immune stimulation by tumor neopeptide antigens predisposes otherwise normal B cells to neoplastic transformation. We believe that this case provides hypothesis-generating clinical data for improving our understanding of the interplay between B cell activation and their potential to transform into lymphoma cells.
The synchronous presentation of two primary malignancies is rare, even more so when two malignancies coexist within the same location as in the case of a collision tumor. While collision tumors involving colonic adenocarcinomas have been reported [1-4], those involving an indolent B-cell lymphoma are somewhat rare. In addition, whereas defects in DNA repair pathways, in particular mismatch repair, are well described in colorectal adenocarcinoma, no prior reports that address this issue in collision tumors are present in the PubMed database. Defects in DNA mismatch repair occur in 10-15% of sporadic colorectal cancers and are the hallmark of Hereditary Nonpolyposis Colorectal Cancer (HNPCC)- associated malignancies [5]. Loss of a mismatch repair protein occurs via germline mutation in those with HNPCC or Lynch syndrome, and most commonly by promoter hypermethylation of the DNA mismatch repair gene MutL homolog 1 (MLH1) in sporadic cases, both of which result in microsatellite instability. Interestingly, these tumors exhibit a markedly intense lymphoid reaction, which can include peritumoral Crohn’s-like and/or intratumoral lymphocytic infiltration [6]. We report herein an interesting case of a MLH1-deficient adenocarcinoma of the colon in which an associated lymphoid infiltrate was diagnosed as an indolent B-cell lymphoma.
A 54 year-old male with epilepsy presented to the emergency department with several days of progressive abdominal pain and distension. CT imaging of the abdomen and pelvis revealed a colonic mass at the hepatic flexure with fat stranding and diffuse lymphadenopathy as well as marked splenomegaly (Figure 1). Physical exam was significant for a palpable spleen that extended below the level of the umbilicus. There was no palpable peripheral lymphadenopathy. Laboratory evaluation revealed pancytopenia with a white blood cell count of 3400/mm3, hemoglobin of 10.3 gm/dL, and a platelet count of 80,000/mm3. Colonoscopy demonstrated an ulcerated circumferential non-bleeding mass in the hepatic flexure, but no other obvious mucosal irregularities. Histopathological analyses of biopsied tissue confirmed colon adenocarcinoma. Bone marrow biopsy and aspiration demonstrated maturing trilineage hematopoiesis. However, within the aspirate cell clot, aggregates of small lymphocytes, occupying approximately 5% of the marrow cellularity, were identified. By flow cytometry, a monoclonal B-cell population comprising 1.1% of total cellular events was detected with the following immunophenotype: CD19+, CD20+, CD22+, CD79b+, CD5-, CD10-, CD43-, CD25-, and CD103-. Serum protein electrophoresis did not reveal the presence of a paraprotein. Taken together, these data indicated that the patient’s bone marrow contained a B cell lymphoproliferative disorder most consistent with splenic marginal zone lymphoma or MALT lymphoma.
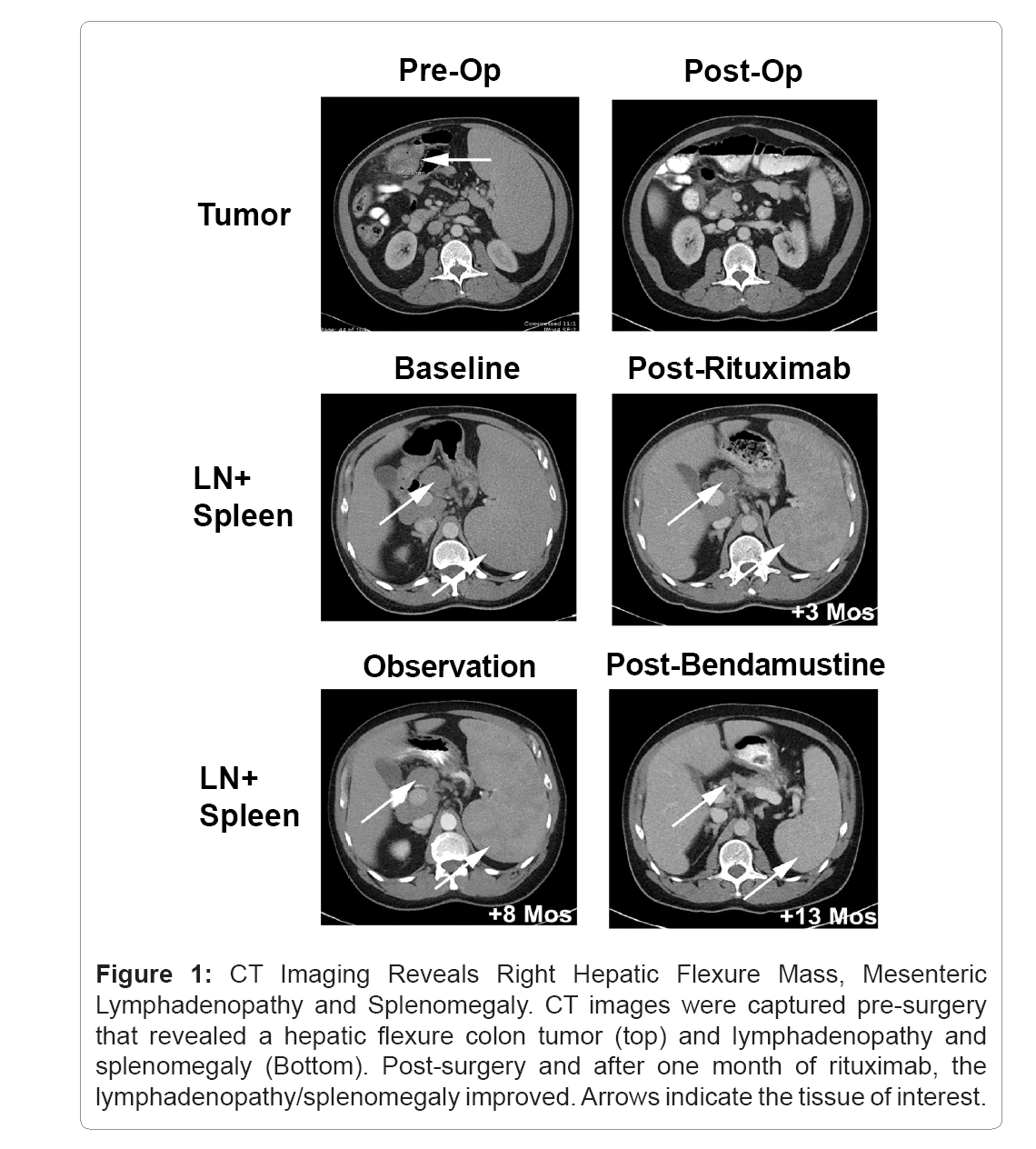
Figure 1: CT Imaging Reveals Right Hepatic Flexure Mass, Mesenteric Lymphadenopathy and Splenomegaly. CT images were captured pre-surgery that revealed a hepatic flexure colon tumor (top) and lymphadenopathy and splenomegaly (Bottom). Post-surgery and after one month of rituximab, the lymphadenopathy/splenomegaly improved. Arrows indicate the tissue of interest.
Shortly thereafter, the patient underwent an uncomplicated open right hemicolectomy revealing a moderately differentiated adenocarcinoma arising from a tubulovillous adenoma. The tumor measured 6 cm, penetrating through the muscularis propria into the pericolonic fat. Immunohistochemical stains were consistent with loss of the mismatch repair proteins MLH1 and PMS2 but not of MSH2 and MSH6, which is consistent with a diagnosis of either Lynch syndrome or sporadic colorectal carcinoma with high microsatellite instability (Figure 2). Forty lymph nodes were negative for metastatic adenocarcinoma, although multiple enlarged lymph nodes were scattered throughout the pericolonic adipose tissue. In addition, several lymphoid aggregates intimately associated with the adenocarcinoma were noted. Morphologically, the lymphocytes present in the lymphoid aggregates and in the lymph nodes appeared similar to those identified in the bone marrow aspirate cell clot. Immunohistochemistry revealed these cells to express CD20 and Bcl-2 (Figure 3) but not CD3 (data not shown). B-cell gene rearrangement studies of the variable and joining regions of the immunoglobulin heavy chain gene confirmed that these cells represented a monoclonal population of B cells (data not shown). Viral hepatitis serologies were negative. Based on a presumed diagnosis of splenic marginal zone lymphoma, the patient received four weekly doses of rituximab, which resulted in only minimal improvement in the degree of splenomegaly and stable lymphadenopathy (Figure 1). On follow up five months later, the spleen had increased in size and bendamustine was added to his treatment regimen, resulting in marked improvement in splenomegaly (Figure 1).
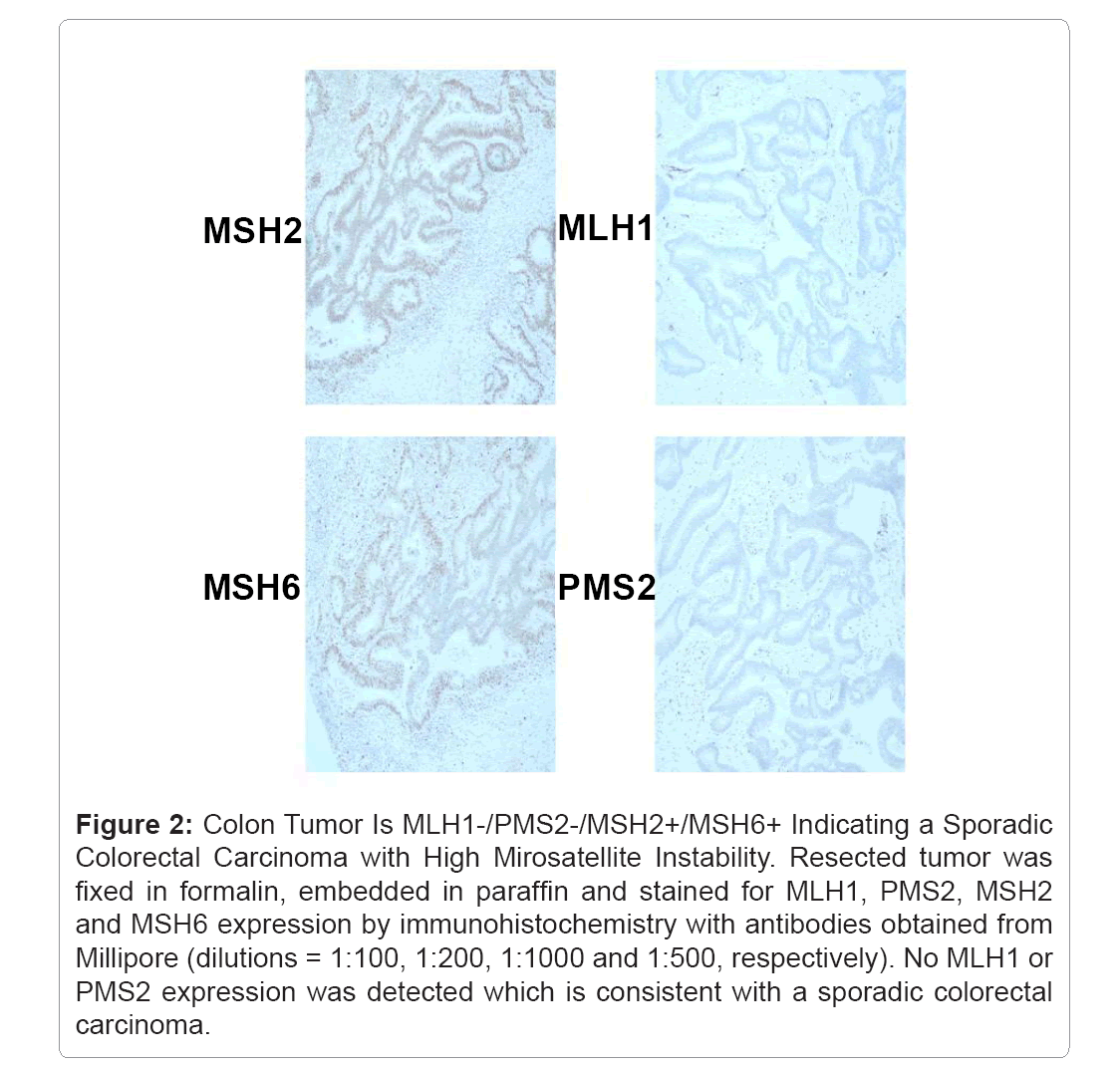
Figure 2: Colon Tumor Is MLH1-/PMS2-/MSH2+/MSH6+ Indicating a Sporadic Colorectal Carcinoma with High Mirosatellite Instability. Resected tumor was fixed in formalin, embedded in paraffin and stained for MLH1, PMS2, MSH2 and MSH6 expression by immunohistochemistry with antibodies obtained from Millipore (dilutions = 1:100, 1:200, 1:1000 and 1:500, respectively). No MLH1 or PMS2 expression was detected which is consistent with a sporadic colorectal carcinoma.
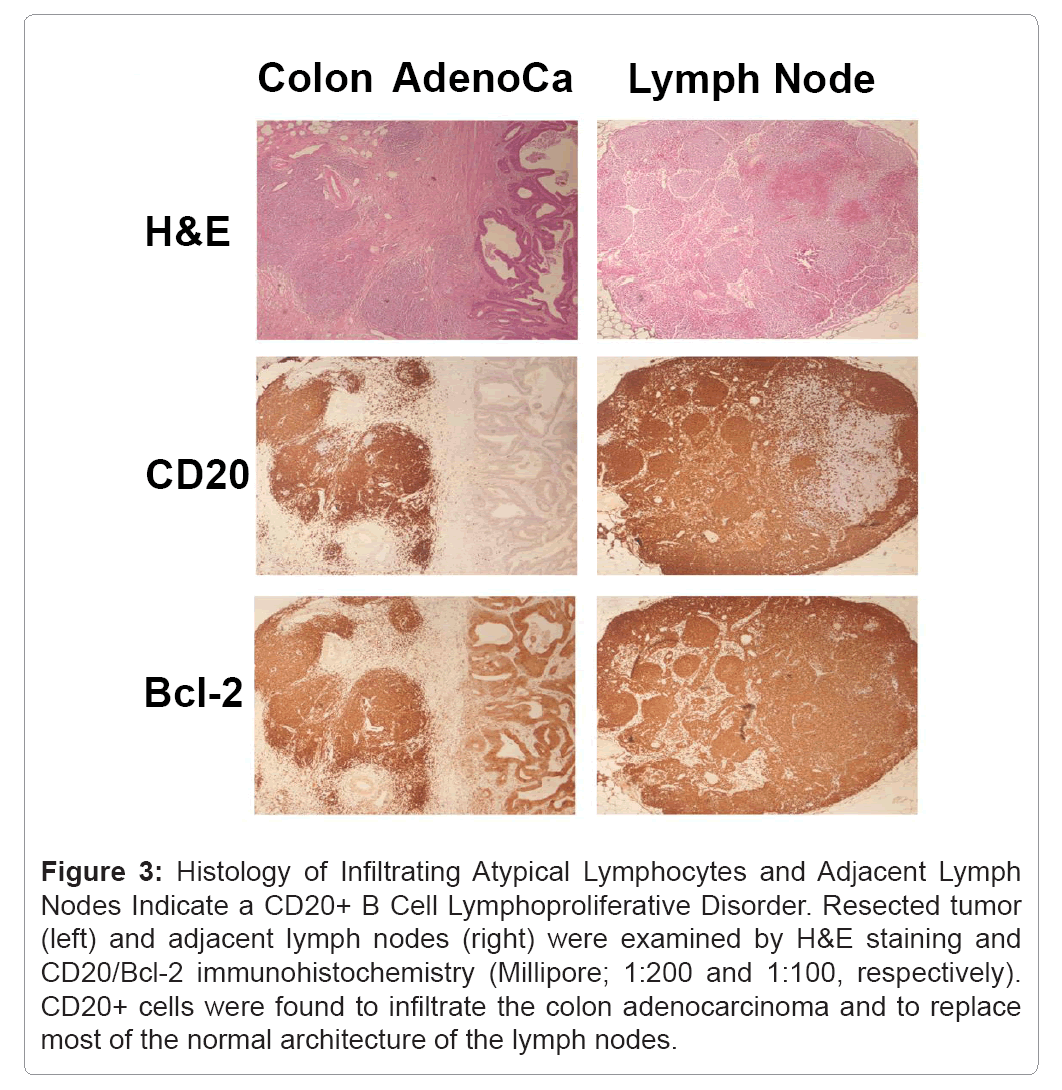
Figure 3: Histology of Infiltrating Atypical Lymphocytes and Adjacent Lymph Nodes Indicate a CD20+ B Cell Lymphoproliferative Disorder. Resected tumor (left) and adjacent lymph nodes (right) were examined by H&E staining and CD20/Bcl-2 immunohistochemistry (Millipore; 1:200 and 1:100, respectively). CD20+ cells were found to infiltrate the colon adenocarcinoma and to replace most of the normal architecture of the lymph nodes.
Although the flow cytometric (CD20+/CD79b+) and immunohistochemical (CD20+) analyses as well as clinical presentation (splenomegaly) suggested that the patient may have had splenic marginal zone lymphoma [7,8], the infiltration into colon was somewhat atypical for this type of lymphoma. Indeed, collision tumors can sometimes confound an otherwise straightforward diagnosis. In addition, the simultaneous diagnosis of a B cell lymphoma and a colon adenocarcinoma would typically pose a therapeutic dilemma. However, this was less of an issue in this patient as fluorouracilbased chemotherapy regimens do not benefit patients with stage II microsatellite unstable colon cancers [9]. Accordingly, the patient’s only treatment for his colon cancer consisted of surgical resection and the choice of chemotherapy was based solely on his lymphoma.
Aside from treatment considerations, there is the question of if and how these two cancers might affect one another’s natural history? The relative rarity of collision tumors would seem to suggest that the coexistence of two malignancies in the same location is only by chance. Although the influence of one cancer on the other is largely unknown, certain pro-neoplastic cytokines that are released by tumor cells have paracrine activities. For example, the immunosuppressive cytokine transforming growth factor (TGF) - promotes tumor growth through the inhibition of the proliferation and activity of tumor antigenspecific CD8+ T cells which normally function to lyse tumor cells [10]. Certainly, one could envision a situation whereby one tumor type is secreting TGF-, not only cloaking the source tumors but also any adjacent disparate tumors (Figure 4). Another possible mechanism by which one tumor type might benefit from its collision counterpart is via the stimulation of angiogenesis. Oncogenic Ras signaling enhances the expression of the pro-angiogenic cytokine vascular endothelial growth factor (VEGF) [11,12] and one tumor type might gain the ability to secrete VEGF via genetic alterations that activate Ras signaling which could promote neo-vascularization to support an adjacent disparate tumor (Figure 4).
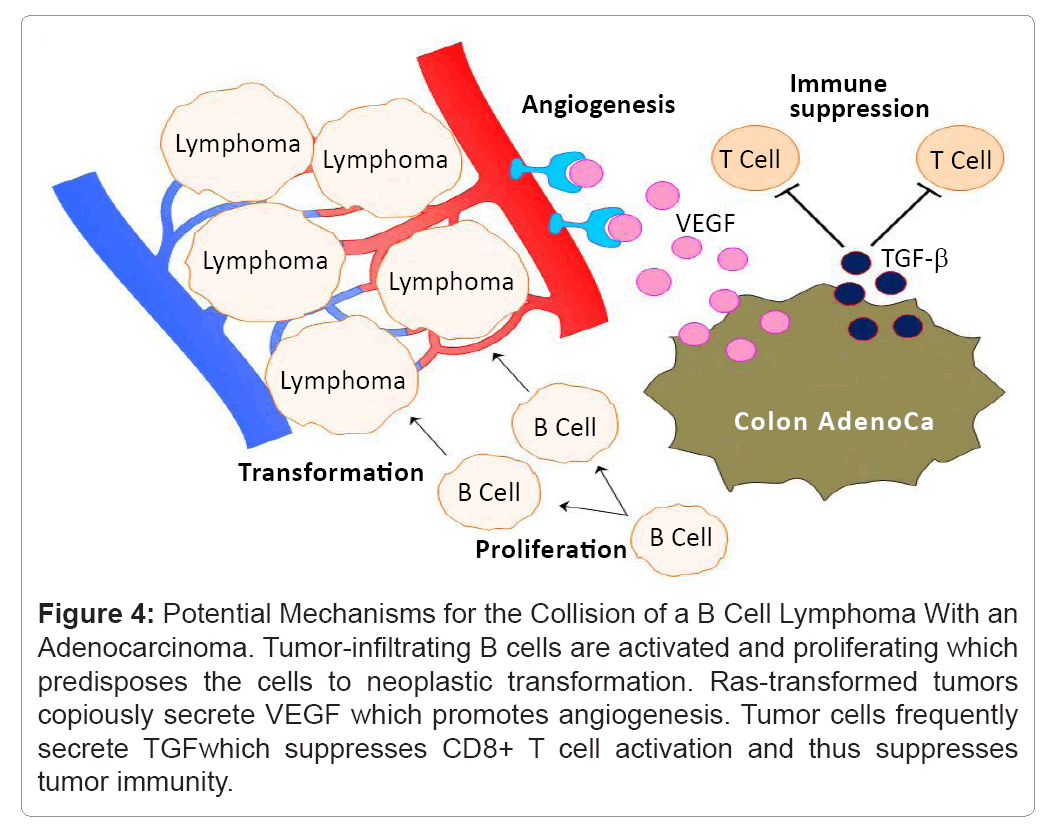
Figure 4: Potential Mechanisms for the Collision of a B Cell Lymphoma With an Adenocarcinoma. Tumor-infiltrating B cells are activated and proliferating which predisposes the cells to neoplastic transformation. Ras-transformed tumors copiously secrete VEGF which promotes angiogenesis. Tumor cells frequently secrete TGFwhich suppresses CD8+ T cell activation and thus suppresses tumor immunity.
Microsatellite unstable colon tumors display a major lymphocyte infiltration and it has been hypothesized that this is due to immune priming by neopeptide antigens created through frameshift and insertion/deletion mutations [13,14]. Matched stage for stage, patients with colon cancer displaying microsatellite instability have a better prognosis than their counterparts with microsatellite stable tumors and are less likely to have metastatic disease at the time of presentation [15]. This improvement in clinical prognosis may result from the expansion of these neopeptide-specific T and B cells and resultant immunebased control of the colon adenocarcinoma proliferative capacity and invasiveness. Neoplastic transformation of normal B cells into B cell lymphoma cells is a multi-step process that requires the loss of cell cycle checkpoints and resistance to apoptosis. We speculate that, in the case of our patient, infiltrating and activated normal B cells were predisposed to transformation via increased activation of proproliferative and mutagenic regulatory proteins such as cyclin dependent kinases. In other words, this pre-disposition may have “set the stage” for a normal B cell clone to more readily transform into an atypical B cell lymphoma. In support of this hypothesis, splenic marginal zone lymphomas have been reported to occur during the course of autoimmunities that are characterized by normal B cell activation and proliferation [8]. Although an alternative explanation could involve the simultaneous loss of MLH1 and resultant microsatellite instability in the infiltrating B cells, microsatellite instability is exceedingly rare in B cell lymphomas [15].
In conclusion, we have reported the rare collision of an indolent B cell lymphoma and a MLH1-negative microsatellite unstable colon cancer. We believe this clinical case may provide insight into the interplay between B cell activation and their potential for neoplastic transformation.