Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Short Communication - (2016) Volume 5, Issue 3
The prevalence of both obstructive sleep apnoea (OSA) and chronic kidney disease (CKD) has increased significantly over the past two decades and OSA has been identified as a frequent condition among patients with advanced CKD [1,2], suggesting a direct association between the two diseases.
CKD is defined as evidence of structural or functional kidney abnormalities that persist for at least three months [3]. It affects about 10% of the adult population worldwide, and is associated with increased cardiovascular morbidity and mortality.
Moreover, the progression of CKD to end-stage renal disease requiring renal replacement therapy represents an enormous medical and economic burden [4]. Currently, many efforts are made to improve the early recognition of CKD and to retard its progression, working on conventional risk factors such as hypertension, diabetes and obesity [4]. Yet several other factors may contribute to the progression of renal diseases including inflammation, hormonal factors and renal hypoxia.
Despite the identification of new mechanisms leading to renal function decline and despite the possibility to interfere pharmacologically with some of them (for example, blockade of the renin-angiotensin-aldosterone system (RAS) to reduce hyper filtration and proteinuria), CKD generally continues to progress over time.
This is probably due to unrecognized factors which play a role in the disease progression. The role of hypoxia in the progression of renal diseases has been intensively studied in recent years. In animal models, hypoxia appears to play a role in CKD progression, but results in humans are more controversial [5].
Recently, retrospective studies have suggested that intermittent nocturnal hypoxia, a hallmark of OSA together with recurrent respiratory events during sleep, not only increases several folds the risk of developing a cardiovascular event (stroke, myocardial infarction…), but may also contribute to the progression of CKD [6,7]. Yet, the real impact of OSA on CKD progression remains poorly investigated, and the mechanisms linking OSA and CKD progression are incompletely understood, but may include oxidative stress, inflammation, endothelial cell dysfunction and direct stimulation of the sympathetic nervous system and the renin-angiotensin-aldosterone system.
In epidemiological studies, an association between OSA and advanced CKD has been found and persists after correction for potential confounding factors such as diabetes, hypertension and obesity, suggesting a direct association between the two diseases [1,8].
On the other hand, a general population based study focusing on early CKD showed an impaired sleep quality of CKD patients, but no association between OSA and kidney function after correction for confounders [9]. This suggests that the increased prevalence of OSA in patients with advanced CKD may be due to factors appearing only late in the course of kidney function decline.
Accordingly, OSA may play a greater role in the decline of kidney function once CKD is present, than in the initiation of the kidney disease.
In the meantime, there is some evidence that kidney failure may promote the development of OSA and nocturnal hypoxia.
One possible mechanism of this reverse causality relationship could be the CKD-induced fluid overload, with upper airways collapse being amplified by overnight fluid displacement to the neck soft tissues. Indeed, movements of fluid towards the neck have been documented in end-stage renal disease patients with OSA [10].
Nevertheless, it is less certain whether fluid shifts occur in the earlier stages of CKD. In addition, earlier works have shown that some therapeutic options of kidney failure, like nocturnal haemodialysis [11] or nocturnal peritoneal dialysis [12], improve the severity of OSA, suggesting that factors originating from the decline of renal function may participate in the increased prevalence of OSA in end-stage renal disease patients.
Taken together, available data strongly suggest the existence of an association between CKD and OSA, without addressing the direction of neither the causal link nor the underlying pathophysiological mechanisms in satisfactory way.
In fact, OSA may be a consequence of CKD as well as an aggravating factor of CKD progression. We propose a bidirectional relationship between OSA and CKD (Figure 1), and we estimate that a better understanding of the causal relationship between OSA and renal function is of great clinical interest: if OSA confirms to be a risk factor for the progression of CKD, identification and treatment of OSA may provide a potential disease-modifying intervention that could delay the progression of kidney disease.
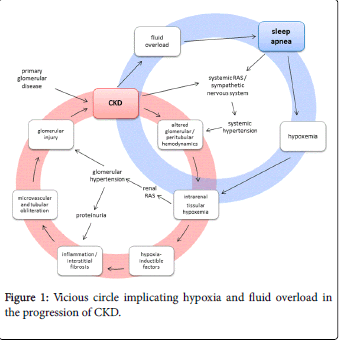
Figure 1: Vicious circle implicating hypoxia and fluid overload in the progression of CKD.
Such observations may be of particular interest in the light of the actual development of drugs interfering with renal oxygen-sensing mechanisms and interstitial fibrosis.
On the reverse side, demonstrating that CKD-related factors like water retention contribute to the development of OSA could result in the study of specific strategies to treat CKD-related complications (e.g. a better management of fluid overload), allowing to break the vicious circle of nocturnal hypoxia. Moreover, an adequate screening and management of OSA in CKD patients may help to reduce their very high cardiovascular risk.