Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 1
Background: This research examined gender variations in depressive mood for high school students affected by emotional upset and how such depressive mood affect their sleep quality.
Methods: This research was conducted for 2 months from September 2015 to October 2015. Both males and females were divided into normal group and depressive group by Zung Self-rating Depression Scale (ZSDS). Each group adopted the Pittsburgh Sleep Quality Index (PSQI) to measure sleep quality. Chi-Square test and AVOVA analysis through SPSS-21 were used as statistics methods.
Results: Analysis was made on a total of 155 students (83 male, 72 female students) that submitted clear answers to the questionnaire. There were 86 students in the normal group and 69 students on the depressive group according to the ZSDS. More female students had depressive mood than male students with 52.8% and 37.3% respectively but without particular statistical meaning. The average ZSDS for all high school students was 43.38 and the average PSQI was 5.39. The number of male students in the normal and depressive group who were diagnosed with sleep disorder were 2 (3.8%) and 9 (29.0%) respectively. But the number of female students in the normal and depressive group who were diagnosed with sleep disorder were 11 (32.4%) and 33 (86.8%) respectively, which was quite meaningful result. Both males and females shared a meaningful result over sleep latency, sleep disturbance, use of sleep medication, and daytime functional disturbance among 7 items of PSQI for sleep quality, and female students had a significantly meaningful result over sleep duration, habitual sleep effects.
Conclusions: This research showed that sleep quality of all high school students was not too bad but it can be problematic for those with depressive mood. Especially, female students with hormone changes and emotional instability were diagnosed with sleep disorder more than male students.
Keywords: Depression; Sleep; Zung self-rating depression scale (ZSDS); Pittsburgh sleep quality index (PSQI); High school students
Sleep is one of important physiological processes, accounting for one third of biorhythm of entire life. According to studies conducted in the western countries, 25-40% of adolescents experience sleep disturbance [1,2]. Similar reports on Asian countries, a report on China states 16.9% of adolescents experience sleep disturbance [3]. Although a slight difference in prevalence appears to exist based on these numbers only, it is difficult to accurately determine the difference due to lack of comparative studies of Asian and western countries on the topic. However, it is clear that a significant number of adolescents experience sleep disturbance.
Adolescents’ normal sufficient sleep duration is defined as eight or more hours of sleep on an average school night [4]. Normal sleep is essential for student heath; however, they take sleep insufficient for their required amount of sleep due to various factors.
According to international studies, sleep duration decreases in students in higher grades [5,6]. According to National Sleep Foundation Sleep in American Poll, proportion of students who take 8 or less hours of sleep was 16% for 6th graders, whereas 75% for 12th graders [7]. In particular, there was a report that in Korea, among Asian countries with high level of academic stress, students’ average sleep hours is 4.9 hours [5]. Such insufficient sleep in the adolescent period results in negative impacts on mood, attention, and school performance.
Judith Owens stated that contributing factors of insufficient sleep include biologic processes such as hormonal change, electro-media, school start times, caffeine, medical illness, and mental health issues such as depressive mood [8]. The mood disorders among the factors have a bidirectional relationship with sleep disturbance where the former can worsen the latter and can result from the latter [9].
Depressive disorder in adolescence has become a serious issue as its prevalence is reportedly 12.3% in the U.S., and 41.3% in Korea [10,11]. In particular, the primary causes of high prevalence of adolescent depression include schools that exclude developmental features, overall societal pressure on academic performance, uncertainty of future, and anxiety about college entrance [12,13]. In particular, adolescence is a transitional period to adulthood, with instability due to emotional, cognitive and physical change.
Depressive symptoms shown in this period can lead to persistent sadness, failure in school performance, and reduced motivation, resulting in various problem behaviors. In addition, various physical problems such as loss of appetite, depressed mood, anxiety disorder, altered sleeping, and psychosomatic symptoms may be exhibited [14,15].
In particular, as untreated depression may continue to adulthood and develop into major depressive disorder, it is important to investigate the association between early depressive mood and sleep disturbance in adolescence.
Association between depressive state and sleep disturbance in adolescence has been demonstrated by several studies. Pigeon, et al. [16] reported that women experiencing sleep disturbance have low expectation of their own health and physical and mental health symptoms more frequently. In addition, adolescents with sleep disturbance develop depressive symptoms more often than adolescents without sleep disturbance, and the symptoms maintained [17,18].
Research on the relationship between sleep disturbance and depressive symptoms have been conducted continuously because various factors affect the relationship. For example, demographics, family, school, intersexual relationships, and social factors may affect it [19]. In addition, gender difference may exist. While most studies reported prevalence of sleep disturbance was higher among female students than male students, the opposite results have also been reported [20,21].
The conflicting results may suggest that a variety of factors contribute to results in addition to sample size and location of studies. In the end, it was found that although sleep disturbance in adolescence occurs due to a variety of factors, studies show inconsistent results. However, these studies shared in common that their results were similar to the studies on sleep disturbance due to mental status.
In Korea, fact-finding surveys on high school students’ sleep disturbance are lacking, and research on gender difference in effect of depressive mood status on sleep disturbance are also yet to be done. This study was conducted with KIS students to investigate the effect of depressive mood on sleep disturbance, despite small sample size, under the assumption that, as excellent students from around Korea selected by rigorous testing, their variation in academic history can be minimized, and that, due to expensive tuition fees, parents’ economic level and biography based on peer review status can be minimized.
This study adopted a cross-sectional study design in which high school students’ depressive mental status was surveyed and its relationship with sleep disturbance was examined. Study participants consisted of 9th-12th male and female students from KIS, Jeju, Korea. Study period was two months from September to October, 2015. All students were included in the study, but the students who did not participate in the survey and who provided inadequate responses were excluded form analysis.
All survey participants participate in the survey after being informed on the purpose of the study and giving written informed consent. The survey was conducted using two types of questionnaires. First, the depressive mood was surveyed with Zung Self-rating Depression Scale (ZSDS), and sleep quality and disturbances was surveyed with the Korean version Pittsburgh Sleep Quality Index (PSQI).
Participants were classified into normal and depressive groups based on the results of ZSDS; then, each group’s association with PSQI was investigated. The ZSDS consists of 20 items with 4-point scale on selfreported symptoms, with a total score of 80 points. Depression items were scored as follows; 1=a little of the time, 2=some of the time, 3=a good part of the time, 4=most of the time [22,23]. The worst possible psychological status scores 80 points, and the best possible psychological status scores 20 points. Total ZSDS score may be associated with clinical relevance.
The ZSDS were interpreted as follows: normal range (20-44), mildly depressed (45-59), moderately depressed (60-69), and severely depressed (70 and above). In this study, ZSDS scores of 44 or less were classified into the normal group, and ZSDS scores of 45 or more were classified into the depressive group.
The PSQI is a self-administered questionnaire on overall status of sleep in the past 1 month, consisting of 19 items. It represents overall status of sleep using seven components: Subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime function [23].
Each component is scored on 0-3 point scale with a total of 21 points. The total scores of 6 points or more indicates poor sleep quality, and is defined as having sleep disturbance [24]. That is, high the PSQI scores indicate poor sleep quality.
Statistical analysis
In terms of statistical analyses, Chi-Square test and analysis of variance (ANOVA) were conducted using the Statistical Package for Social Sciences Software (SPSS-version 21). Descriptive analyses were performed to describe prevalence of depressive symptoms in male and female students as well as all participating students. To investigate the effect of depressive mental status on sleep quality by gender, two-way ANOVA was performed. To investigate if the depressive mental status varied in gender, Chi-Square test was performed.
More specifically, for symmetric measures, Pearson’s product moment correlation coefficient was used for interval scale, and Spearman rank-order correlation coefficient was used for ordinal scale. Means and standard deviations were calculated for sub-scale scores of each group. The p-value of <0.05 were considered the level of statistical significance difference.
Students who provided adequate responses on the survey were 83 male and 72 female students, and 155 students in total. The proportions of male and female participants were 53.6% and 46.4%, respectively. Students’ grades were well-distributed between 9th-12th grades. The mean age of all participants was 17.08 years; the mean age of male participants was 17.08 years; and the mean age of female participants was 17.07 years. The mean ZSDS score of all participants was 43.39, and the mean PSQI score was 5.38.
Does depressive mood state vary between genders?
Distribution in the ZSDS to investigate mood state of each group is shown in Figure 1. In the total student population, the normal group included 86 students (55.5%), and the depressive group included 69 students (44.5%).
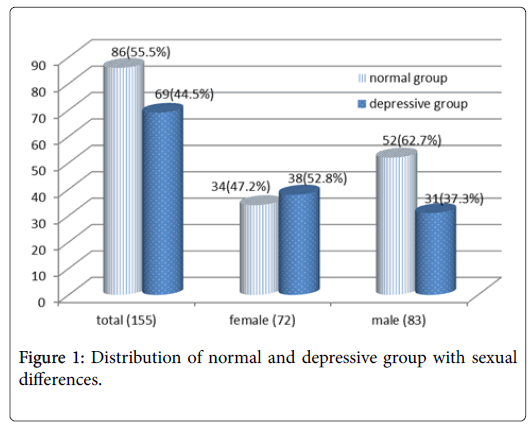
Figure 1: Distribution of normal and depressive group with sexual differences.
In terms of gender, the normal and the depressive groups included 52 (62.7%), 31 (37.3%) male students, and 34 (47.2%), 38 (52.8%) female students, respectively, showing higher proportion of depressive mood in female students. The mean ZSDS score also was also found to be higher in female students, with 41.92 for male and 45.08 for female students (P<0.05) (Figure 1).
It was investigated if the mean ZSDS score varied among the total student group, male student group, and female student group. First, the mean ages of the normal and the depressive group in the total student group were 17.12/17.03 years, and the mean ZSDS score were 37.58/50.62. The mean ages of the normal and the depressive group in the male student group were 17.0/17.23 years, and the mean ZSDS score were 37.27/49.71. The mean ages of the normal and the depressive group in the female student group were 17.30/16.86 years, and the mean ZSDS score were 38.06/51.37, respectively.
Does depressive mood state including gender influence poor sleep?
Distribution of normal sleep and sleep disturbance based on the PSQI of each group is shown in Figure 2. It was found that in the total student group, the numbers of students with normal sleep and sleep disturbance were 87 (56.1%)/68 (43.9%) respectively, with the mean PSQI score of 5.38. In the normal mood state based on the ZSDS, the numbers of students with normal sleep and sleep disturbance were 73 (84.9%)/13(15.1%) respectively, with the mean PSQI score of 3.84, and in the depressive group, the numbers were 14 (20.3%)/55 (79.7%) respectively, with the mean PSQI score of 7.32, suggesting depressive mood state have greater impact on poor sleep (p<0.05). However, in the comparison of the normal and depressive group by gender showed slight different results. First, among male students, in the normal group, the numbers of students with normal sleep and sleep disturbance were 50(96.2%)/2(2%) respectively, with the mean PSQI score of 3.40, and also in the depressive group, the numbers were 22(71.0%)/9(29.0%) respectively, with the mean PSQI score of 6.92.
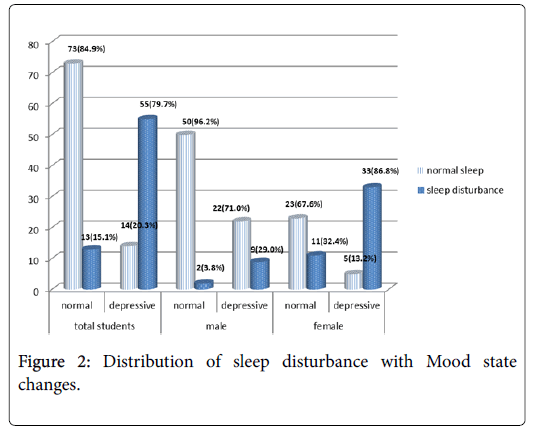
Figure 2: Distribution of sleep disturbance with Mood state changes.
The standard deviation of the PSQI scores was large at 6.92 ± 3.22, while mean scores were high. This suggests that sleep disturbance did not vary significantly among male students (p>0.05). However, among female students, in the normal group, the number of students with normal sleep and sleep disturbance were 23 (67.6%)/11(32.4%) respectivey, with the mean PSQI score of 4.50, and in the depressive group, the numbers were 5(13.2%)/33(86.8%) respectively, with the mean PSQI score of 7.47, suggesting significant impact of mood on poor sleep (p<0.05) (Table 1).
| Normalgroup | Depressivegroup | ||
|---|---|---|---|
| Total | Age(years) | 17.12 | 17.03 |
| Highschoolstudents | ZSDS | 37.58 | 50.62 |
| PSQI | 3.84 | 7.32 | |
| Malestudents | Age(years) | 17.3 | 16.86 |
| ZSDS | 38.06 | 51.37 | |
| PSQI | 4.5 | 7.47 | |
| Female students | Age(years) | 17 | 17.23 |
| ZSDS | 37.27 | 49.71 | |
| PSQI | 3.4 | 6.92 | |
Table 1: Mean values of age, ZSDS, PSQI in normal and depressive groups.
What is the effect of depressive mood state on sleep quality subscales?
Although it was found that sleep disturbance vary between males and females in their mood states, it is also important to examine which sleep quality is affected. In each group, the effect on seven subscales of PSQI was examined.
First, the total student group showed a significant difference in five subscales among normal and depressive group PSQI subscales: Sleep latency (0.47 ± 0.077/1.13 ± 0.107), sleep duration (1.09 ± 0.090, 1.62 ± 0.113), sleep disturbance (0.77 ± 0.049, 1.29 ± 0.066), use of sleep medication (0.27 ± 0.061/0.90 ± 0.134), and daytime dysfunction (1.07 ± 0.075/1.77 ± 0.088) (p<0.05) (Table 2).
| Normal(52) | Depressive(31) | p-value | |
|---|---|---|---|
| Subjectivesleepquality | 0.06±0.025 | 0.10±0.055 | 0.478 |
| Sleeplatency | 0.47±0.077 | 1.13±0.107 | 0 |
| Sleepduration | 1.09±0.090 | 1.62±0.113 | 0 |
| HabitualSleepefficiency | 0.12±0.035 | 0.33±0.092 | 0.029 |
| Sleepdisturbance | 0.77±0.049 | 1.29±0.066 | 0 |
| Useofsleepmedication | 0.27±0.061 | 0.90±0.134 | 0 |
| Daytimedysfunction | 1.07±0.075 | 1.77±0.088 | 0 |
Table 2: PSQI difference between total normal and depressive students
Male students showed a significant difference in four subscales among normal and depressive group the PSQI subscales: Sleep latency (0.50 ± 0.097/1.19 ± 0.170), sleep disturbance (0.71 ± 0.069, 1.39 ± 0.110), use of sleep medication (0.21 ± 0.074/1.03 ± 0.205), and daytime dysfunction (0.94 ± 0.084/1.61 ± 0.152) (p<0.05) (Table 3).
| Normal | Depressive | p-value | |
|---|---|---|---|
| Subjectivesleepquality | 0.04±0.027 | 0.23±0.120 | 0.138 |
| Sleeplatency | 0.50±0.097 | 1.19±0.170 | 0.001 |
| Sleepduration | 0.87±0.110 | 1.23±0.178 | 0.091 |
| HabitualSleepefficiency | 0.13±0.048 | 0.45±0.166 | 0.075 |
| Sleepdisturbance | 0.71±0.069 | 1.39±0.110 | 0 |
| Useofsleepmedication | 0.21±0.074 | 1.03±0.205 | 0.001 |
| Daytimedysfunction | 0.94±0.084 | 1.61±0.152 | 0 |
Table 3: PSQI difference between normal and depressive male students.
Female students showed a significant difference in five subscales among normal and depressive group PSQI subscales: Sleep latency (0.41 ± 0.127/1.08 ± 0.138), sleep duration (1.44 ± 0.135/1.95 ± 0.125), sleep disturbance (0.85 ± 0.062/1.21 ± 0.077), use of sleep medication (0.35 ± 0.102/0.79 ± 0.178), and daytime dysfunction (1.26 ± 0.136/1.89 ± 0.098) (p<0.05) (Table 4). These results suggest that both male and female students in the depressive state have difficulty with sleep induction. This insomnia pattern results in daytime dysfunction due to insufficient hours of sleep when the focus on study is required, making it difficult for students to engage in school life. In addition, as frequency of taking drugs to solve this pattern increases, students may develop drug dependency, and vicious cycle of poor sleep and quality of school life may occur.
| Normal | Depressive | p-value | |
|---|---|---|---|
| Subjectivesleepquality | 0.09±0.049 | 0.00±0.00 | 0.083 |
| Sleeplatency | 0.41±0.127 | 1.08±0.138 | 0.001 |
| Sleepduration | 1.44±0.135 | 1.95±0.125 | 0.007 |
| HabitualSleepefficiency | 0.09±0.049 | 0.24±0.096 | 0.173 |
| Sleepdisturbance | 0.85±0.062 | 1.21±0.077 | 0.001 |
| Useofsleepmedication | 0.35±0.102 | 0.79±0.178 | 0.037 |
| Daytimedysfunction | 1.26±0.136 | 1.89±0.098 | 0 |
Table 4: PSQI difference between normal and depressive female group.
High school students are in the adolescence transitioning from childhood to adulthood with rapidly occurring major changes in physical, emotional, and social aspects. The students develop selfidentity by overcoming this period [25]. Many students experience difficulty in adjusting to these changes, and a variety of stresses including academic performance and relationship building. If they are exposed to chronic stress, depression is likely to develop through interaction with various factors such as genetic diathesis [26]. When the depression is not properly addressed and continues into adulthood, drug overuse, sexually reckless behavior, sense of alienation, and suicidal thoughts and behaviors may occur frequently or worsen [27]. Therefore, it is imperative to facilitate normal school life and pee relations through proper assessment of depression and reducing maladjustment in the early adolescence. First, epidemiology of adolescent depression needs to be understood. In the total population, the depressive mood rate is fairly high at 44.5%. This result may result from a lack of emotional support as the KIS is a private dormitory school and located in a rural area, and therefore, they are cut off from family. As a related study result, Liu et al. reported that results vary according to student age and grade, and students from incomplete families with little peer review experience sleep disturbance [28]. Regarding reports on separate results for male and female, there is a report that depression prevalence rate is higher for women than men [29], and there is a report of opposite result [30]. In our study, female students’ depression prevalence rate was 52.8%, higher than male students’ 37.3%. For such higher prevalence of depression in women, both biological cause of hormonal change such as menstruation and social cause such as psychological conflict experienced as they realize male-dominant society have been presented as explanations [15].
The sleep deprivation, the most important aspect of life, is the most important aspect of adolescence in the developmental process because it interferes with daily life due to unpleasant mood, reduced concentration, and excessive daytime sleepiness, and results in memory loss and dissatisfaction with interpersonal relationships [8]. Therefore, research efforts on role of sleep are needed as part of efforts to improve quality of life and enhance sense of happiness in adolescence. As a result, many reports have been produced on correlation between depressive mood and sleep in adolescence, a mentally immature stage. In terms of physiological aspect, although sleep appears to be a passive state due to reduced cognition and response to what is happening around, active state due to high level of interaction in central nervous system (CNS) is maintained during sleep. Because of the CNS stimulation, people are affected by many hormones during sleep. Sleep propensity and sleep architecture are in turn controlled by the interaction of two time-keeping mechanisms in the central nervous system, circadian rhythm and sleep-wake homeostasis [31]. In particular, thyroid hormone secreted during sleep modulates loss of appetite and weight loss; luteinizing hormone modulates nervousness; and corticosteroid hormone modulates stress. Unstable sleep in adolescence cause disturbance in the hormones. In addition, when women begin to have menstruation, sleep disturbance is more frequently observed in female students who are affected by follicular hormone and luteinizing hormone imbalance [31,32]. In our study, the proportion of the students who experience sleep disturbance was found to be 43.9%, and in the depressive mood state, the proportion of sleep disturbance was 15.1% for male, and 79.7% for female, showing higher sleep disturbance rate in female students.
In our study, both male and female students showed the problem of sleep induction of sleep latency and sleep disturbance among seven sleep quality subscales of PSQI. In proportion to this result, in the next day, both male and female students complained of daytime dysfunction. In contrast, Seblewngel Lemma, et al. [33] with universal students as study participants reported that those who complained low sleep latency also showed low daytime dysfunction rate. This results demonstrate that poor sleep quality indicate worsening poor daytime dysfunction. In particular, KIS students in our study are under severe pressure on academic performance as the school is a prestigious private school. These students have strong perfectionism. Perfectionism shows the personality of having a high and rigid standard with regard to performance, fear of failure and excessive selfcriticism [34]. The perfectionism has been reported to have a direct negative impact on sleep and psychological functioning [34]. Most students with high academic achievement seek perfectionism. Lan Guo, et al. [29] reported that the students with below-average academic pressure complains sleep disturbance less. This suggests that academic pressure serves as a stressor that influences sleep disturbance. Due to this aspect, prevalence of depression and sleep disturbance was found to be higher in our study than in other studies on relationship between sleep and mood.
In conclusion, this study demonstrated that depressive mood is closely associated with sleep disturbance in adolescence. Also, our research showed that sleep quality of all high school students was not too bad but it can be problematic for those with depressive mood. Especially, female students with hormone changes and emotional instability were diagnosed with sleep disorder more than male students. Such results imply that mental state of high school students can disturb their healthy sleep and can affect general well-being state negatively. Adolescence is when the conflict between needs for sleep and social life occurs. There is no way to prevent sleep deprivation due to academic aspect of preparation for future. However, it would be possible to provide careful attention and sufficient care to the students in an early stage of depressive state, since sleep and depression are in a mutually dependent relationship as discussed earlier. This is expected to contribute to good sleep by minimizing at least the effect on mood change among various factors of poor sleep.