Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2013) Volume 2, Issue 6
Study objectives: This study wanted to evaluate the correlations between haematic cortisol levels and the craniofacial morphology in children with Obstructive Sleep Apnoea Syndrome (OSAS) in comparison with healthy children.
Design/setting/patients. This is a case-control study. Children referring to the Paediatric Department, University of Insubria, Varese, in the period between 1st and 31st October 2011 for a history of disturbed sleep were evaluated and 28 children, compliant to our criteria, were enrolled in the study.
Interventions: All patients underwent a full-night polysomnographic evaluation. Haematic cortisol levels were measured using a radioimmunoassay technique. An orthodontic evaluation and a cranial lateral cephalometric analysis were performed.
Measurements and results: Haematic cortisol concentration at 2.00 am was found higher in OSAS patients than in controls (p<0.05). An increase in craniomandibular (p<0.05) and intermaxillar (p<0.01) angles indicated a high angle tendency in OSAS with a posterior rotation of the mandible. A retro-position of the mandible (p<0.05), an increased overjet (p<0.01) and a reduction of overbite (p<0.01) were also found.
Conclusions: The altered hypothalamic-pituitary-adrenal activity and the craniofacial modification found are not enough to state if these conditions are causes rather than consequences of OSAS. Moreover cortisol and sleep fragmentation can cause a reduction of growth hormone secretion so it is possible that the alteration of facial morphology may also have a metabolic cause.
Obstructive Sleep Apnoea Syndrome (OSAS) is a common problem in children [1]. The prevalence of OSAS in diagnostic studies ranges widely from 0.1 and 13%, even if great part of the literature converges on variations between 1 and 4% [1]. A difference in the prevalence based on age is not proven, even if several studies indicate a peak of incidence between 2 and 8 years, which is the age in which the tonsils and adenoids are the largest in relation to the underlying airway [2]. OSAS is defined by the American Academy of Pediatrics as ‘‘a disorder of breathing during sleep characterized by prolonged partial upper airway obstruction and/or intermittent complete obstruction (obstructive apnea) that disrupts normal ventilation during sleep and normal sleep patterns” [3].
Diagnosis of OSAS is based on medical history, physical examination and tests confirming the presence and severity of the upper airway obstruction, it is well known, however, that OSAS in children is not only associated with enlarged tonsils and adenoids, but also with the presence of abnormal airway collapsibility during sleep [4]. The gold standard for diagnosing OSAS is therefore the overnight polysomnography (PSG) [2,5]. Among the parameters measured with PSG, the Apnoea-Hypopnoea Index (AHI) is commonly used to evaluate the presence or absence of disease and to assess its severity; the AHI represents the number of obstructive apnoea and obstructive hypopne as observed per hour of Total Sleep Time (TST).
There is evidence suggesting that nocturnal awakenings in OSAS are associated with alterations in Hypothalamic-Pituitary-Adrenal (HPA) activity, specifically, increased pulsatile cortisol release [6]. Cortisol is the primary human glucocorticoid product of the HPA axis and major functions include metabolic (for example gluconeogenesis) and blood pressure regulation and immune suppression. Excess cortisol secretion is associated with numerous adverse systemic consequences, such as metabolic syndrome, diabetes, hypertension, depression and insomnia [7]. The circadian rhythm of secretion of cortisol is strongly related to sleep, an altered regulation of cortisol levels has been proposed as a mechanism through which sleep disorders manifest some of their pathologic effects [8]. In 1972, a study by Gillin et al. reported that glucocorticoids decreased REM sleep and increased time spent awake [9]. The human endogenous, SCN-controlled cortisol circadian rhythm is characterized by cortisol levels begin to rise about 2-3 h after sleep onset and a continuous arousal during the early waking hours. The peak, or acrophase, of the level of cortisol is indicated at about 09.00 h. As the day continues, there is a gradual decline in cortisol levels and as sleep ensues there is a continued decrease to the nadir [7].
In literature nocturnal awakenings has been associated with pulsatile cortisol release and autonomic activation leading to an increased release of catecholamine, Corticotropin-Releasing Hormone (CRH) and cortisol. OSAS seems to cause activation of the HPA axis through a similar mechanism of autonomic activation, awakening, and arousal [10,11]. HPA axis hyperactivity can have many negative effects on sleep. It can lead to sleep fragmentation, decreased Slow-Wave Sleep (SWS), and shortened sleep time. Likewise, OSAS can exacerbate HPA axis dysfunction, worsening the cycle [7].
In growing subjects, chronic obstructive airway disease is often associated with disorders of orthodontic interest [12-15]. In this field several studies has been conducted but the nature of the anatomical and functional relationships between respiratory and dental apparatuses makes it difficult to understand how the dysfunctions interact. It has been matter of discussion ascertain whether the craniofacial alterations are a cause or, rather, a consequence of increased resistance to oronasal airflow. Harvold et al. in 1981 showed the presence of cranial and muscle alteration in growing primates in which oral breathing was experimentally induced for an extended period of time [16].
Physiological breathing seems to play an active role in harmonious craniofacial development, therefore when external factors alter its mechanism functional and skeletal alterations can be observed. The most evident consequences of chronic nasal obstruction are represented by orofacial alterations related to an abnormal mandible displacement and a subsequent dysmorphism of the oral structures leading to a modified posture [13]. Under normal conditions tongue influence and regulate the upper jaw morphogenesis. Conversely, when breathing through the mouth, the tongue assumes a forward and downward position, moving its dorsum and the tonsillar tissue away from the posterior pharyngeal wall and does not perform its modelling function on the palate; for this reason the teeth and the maxilla are deprived of their natural support. The consequent “stretching” of the lips and the cheeks causes a centripetal force and inhibits a correct transverse maxillary growth predisposing lip incompetence [14]. It is interesting to note that, since the palate forms the basis of the nasal cavity, its contraction could represent a further cause to obstruction of the nasal flow, creating, also in this case, a vicious circle. The most frequent dysgnathia is represented by both dental and skeletal Class II, with reduction of the transverse diameter of the upper arch, ogival palate, mono- or bilateral posterior crossbite, and anterior open bite with buccally inclined upper incisors [13].
The aim of this preliminary study is to evaluate correlations between haematic cortisol levels and the craniofacial morphology in children diagnosed with OSAS, in comparison with a group of healthy children.
Subjects
Children referring to the Paediatric Department, University of Insubria, Varese, in the period between 1st and 31st October 2011 for a history of disturbed sleep were evaluated. 28 children, compliant to our inclusion and exclusion criteria, showed Table 1, were enrolled in the study. The present study was conducted in accordance with the Helsinki Declaration and informed consent was obtained from all participants.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age in the range 5-7 years BMI in the range 13.5*-17** History of disturbed sleep |
History of ENT surgery History of allergy Chronic illness Use of decongestant preparations Acute upper airway infections Acute otitis media Dysmorphic or craniofacial syndromes History of orthodontic treatment Primary adrenocortical hyperfunction |
Table 1: Inclusion and Exclusion Criteria of the sample.
All 28 patients underwent a full-night polysomnographic evaluation and were divided in two groups. The group of paediatric OSAS included 18 patients (8 males, 10 female), with a mean age of 6.1 ± 0.9 (mean ± SD). The control group was represented by 10 children (4 males, 6 females) with a mean age of 5.9 ± 1.0 (Table 2).
| Age (y) | Male | Female | Tot | |
|---|---|---|---|---|
| OSAS | 6.1 ± 0.9 | 8 | 10 | 18 |
| Not OSAS | 5.9 ± 1.0 | 4 | 6 | 10 |
Table 2: Age and gender of the sample.
Measurements
In the first phase of the study all patients underwent a overnight, 12 channels, polysomnographic evaluation (E-Series, Compumedics, Melbourne, Australia), performed in a sleep laboratory. The following parameters were analysed: nasal air flow, chest and abdominal movements, snoring, transcutaneous SaO2 saturation, electroencephalogram, electrooculogram, electromyogram, body position and heart rate with electrocardiography.
All recordings were scored manually by the same operator. An obstructive apnoea was defined as the cessation of airflow for at least 10 seconds with continuing abdominal and thoracic movements according to the American Academy of Sleep Medicine [17]. An obstructive hypopnoea was defined as a 50% reduction in airflow for at least 10 seconds, compared with baseline, accompanied by abdominal and thoracic movements in combination with an arousal or an oxygen desaturation of 3% or more [17].
The obstructive apnoea-hypopnoea index was defined as the mean number of obstructive apnoea and hypopnoea per hour of sleep. According to the American Academy of Paediatrics’ guidelines [3], we considered OSAS children showing AHI over 1.5.
Blood samples from the patients were collected and haematic parameters were evaluated.
Blood samples were collected at: 02.00 am and at 08.00 am with peripheral heparinized catheters and stored at 4°C.
Cortisol plasma levels were measured from each sample using a radioimmunoassay technique (Bridge Cortisol Kit, Adaltis, Roma, Italy) at the Section of Experimental and Clinical Pharmacology, Department of Clinical Medicine, University of Insubria, Varese.
In the second phase, the 18 patients of the OSAS group underwent also a specific clinical orthodontic evaluation and a cranial lateral cephalometry performed by the same specialist in orthodontics. The first phase’s controls children were not taken as controls in the second phase, because, even if they were not diagnosed OSAS, they complained disturbed sleep that could be associated with several conditions, such as oral breathing, so they couldn’t be considered representative of an healthy population. The mean cephalometric values in a 6 aged population of healthy children [18] were considered as controls.
All 18 cephalograms were digitally traced (NemoStudio 8.7.5 UV 10, Software Nemotec S.L., Madrid, Spain) by the same operator. For the cephalometric evaluation the Italian Board of Orthodontics’ cephalometric analysis (IBO) was used [19]. The parameter considered were: angle sella - nasion - subspinale point (SNA), angle sella - nasion - pogonion point (SNPg), difference between SNA and SNPg (ANPg), inclination of the maxilla (SN-ANS.PNS), intermaxillar angle (ANS. PNS–GoMe), inclination of the mandible (SN-GoMe), upper incisor’s inclination (1.1-ANS.PNS), lower incisor’s inclination (4.1-GoMe), lower incisor’s compensation (4.1-APg), overjet (OVJ), overbite (OVB), interincisal angle (1.1-4.1) (Figure 1).
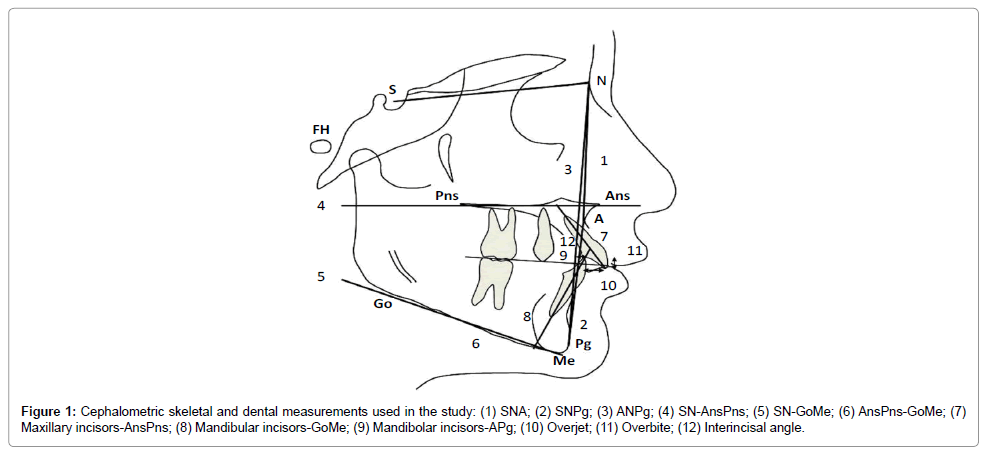
Figure 1: Cephalometric skeletal and dental measurements used in the study: (1) SNA; (2) SNPg; (3) ANPg; (4) SN-AnsPns; (5) SN-GoMe; (6) AnsPns-GoMe; (7) Maxillary incisors-AnsPns; (8) Mandibular incisors-GoMe; (9) Mandibolar incisors-APg; (10) Overjet; (11) Overbite; (12) Interincisal angle.
Statistical analysis
Both cortisol data samples of OSAS and controls groups were found normally distributed by using Shapiro-Wilk test. Difference in haematic cortisol levels between the two groups was evaluated using Independent Samples t-test (MedCalc version 12.3.0.0, Mariakerke, Belgium).
For all OSAS subjects the cephalograms were traced twice by the same observer in two different moments to exclude method errors. No significant mean differences between the two series of records were found by employing paired t-tests. Dalhberg’s formula was used to establish the method error [20]. Method error for the linear measurements was smaller than 0.5 mm while for the angular measurements it was smaller than 1 degree. Cephalometric data were found normally distributed by using Shapiro-Wilk test. The mean values of SNA, SNPg, ANPg, SNANS. PNS, ANS.PNS–GoMe, SN-GoMe, 1.1-ANS.PNS, 4.1-GoMe, 4.1- APg and 1.1-4.1 in a 6 aged population of healthy children [18] were taken as controls to evaluate the presence of significant differences in cephalometric parameters using One Sample t-test (MedCalc version 12.3.0.0, Mariakerke, Belgium). As the mean values of OVJ and OVB were not available in the control’s source (18), we considered as control values the OVJ and OVB normal values indicated by the IBO [19].
Among all the children recruited, 18 fulfilled the OSAS criteria according to the American Academy of Paediatrics [3]. There were no significant differences in age and gender between the groups (Table 2). Data obtained from polysomnographic monitoring underwent manual and instrumental reworking that allowed us to obtain the average percentage O2 saturation (96.0 ± 2.8 in OSAS; 98.1 ± 0.6 in not OSAS), the minimum percentage of O2 saturation (79.9 ± 14.3 in OSAS; 93.4 ± 2.2 in not OSAS) and the Apnoea-Hypopnoea Index (AHI=9.6 ± 5.0 in OSAS; AHI=0.8 ± 0.3 in not OSAS). The Sleep Efficiency and the Sleep Architecture were considered preserved in all subjects (Table 3).
| OSAS | Not OSAS | |
|---|---|---|
| AHI | 9.6 ± 5.0 | 0.8 ± 0.3 |
| SpO2 mean % | 96.0 ± 2.8 | 98.1 ± 0.6 |
| SpO2 min % | 79.9 ± 14.3 | 93.4 ± 2.2 |
| TST (min) | 562 ± 30 | 517 ± 47 |
Table 3: Polysomnographic data.
Haematic cortisol concentration at 2.00 AM was found higher in OSAS patients (57 ± 50 ng/ml) than in controls (23 ± 11 ng/ml) (p<0.05). Conversely differences in concentrations at 8.00 AM were not found significant (176 ± 40 ng/ml in OSAS; 177 ± 56 ng/ml in controls) (Figure 2).
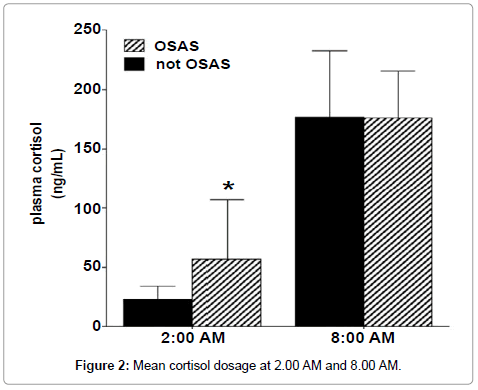
Figure 2: Mean cortisol dosage at 2.00 AM and 8.00 AM.
Cephalometric data are summarized in Table 4. A significant increase in craniomandibular (SN-GoMe, p<0.05) and intermaxillar (ANS.PNS-GoMe, p<0.01) angles indicated a high angle face in the OSAS group with a posterior rotation of the mandible. Retro-position of the mandible was detected by the reduction of SNPg angle (p<0.05) and the consequent enlargement of ANPg angle (p<0.001). Concerning the dentoalveolar parameters OVJ was found increased (p<0.01), according to the mandible’s retro-position mentioned before, while 1.1-ANS.PNS and OVB were found reduced (p<0.01 for 1.1-ANS.PNS, p<0.001 for OVB).
| Variables1 | OSAS subjects (mean ± sd) | Control values2 (mean ± sd) | p-value |
|---|---|---|---|
| SNA | 80.0 ± 3.7 | 80.1 ± 3.5 | NS |
| SNPg | 72.8 ± 3.8 | 76.2 ± 3.4 | 0.0168* |
| ANPg | 7.1 ± 2.0 | 3.4 ± 2.0 | 0.0001*** |
| SN-ANS.PNS | 4.9 ± 1.2 | 6.8 ± 3.0 | NS |
| ANS.PNS–GoMe | 34.5 ± 3.8 | 30.2 ± 4.4 | 0.0029** |
| SN-GoMe | 39.4 ± 3.4 | 37.0 ± 4.8 | 0.0491* |
| 1.1-ANS.PNS | 93.0 ± 10.6 | 105.2 ± 7.4 | 0.0039** |
| 4.1-GoMe | 87.5 ± 5.3 | 83.4 ± 7.3 | NS |
| 4.1-APg | 0.4 ± 1.6 | -1.8 ± 2.5 | NS |
| OVJ | 4.6 ± 1.8 | 3.5 ± 2.5 | 0.0032** |
| OVB | 0.3 ± 1.0 | 2.5 ± 2.5 | <0.0001*** |
| Interincisal Angle | 145.9 ± 12.1 | 140.9 ± 10.7 | NS |
Table 4: Mean cephalometric measures in OSAS subjects and respective control values.
Few studies have been conducted to assess the craniofacial architecture of subjects with OSAS in young children with deciduous or mixed dentition. In the present study, according to Marino et al. [15], the OSAS children showed an orthognatic and harmonious maxilla in the sagittal (SNA) and vertical plane (SN-ANS.PNS). The cephalometric values that were disharmonious with the orthognatic facial pattern were observed in the mandible. The angles SNPg and SN-GoMe showed a retro-positioned mandible with a strong posterior inclination in clockwise direction, in relation to the anterior cranial base. This skeletal discrepancies lead to a hyperdivergent class II with an increased ANPg and anterior facial height. Inclinations of the upper incisors were found reduced and this result can be explained by a dento-alveolar compensatory mechanism described by Solow in 1980 [21]. The increased OVJ is in line with the class II phenotype previously described, even if in literature OSAS and Class II skeletal pattern are not always correlated [12]. The decreased OVB is related to the increase of intermaxillary angle (ANS.PNS-GoMe). However, since the dentoalveolar parameters are evolving in preschool and schoolage children, they are considered less indicative for the prediction of a future facial morphology. Many studies attest the correlation between upper airway obstruction and craniofacial modifications. Harvold in 1981 observed that when a growing primate is experimentally induced to be an oral breather it always develops muscle and cranial alterations [16]. It is important to note that this is a two-way problem: just as oral breathing can determine malocclusive patterns by affecting growth and craniofacial development, it is equally true that the various types of malocclusion can favour oral breathing [13]. Adenotonsillectomy generally resolves the upper airway obstruction, but the persistence or reappearance of snoring and OSAS later in life, after surgery at a prepubertal age, suggests that craniofacial modifications may be precocious and related to genetic or environmental factors [12,21].
The pathophysiology of OSAS has been associated with alterations of the Hypothalamic Pituitary Adrenal (HPA) axis; however a relationship between OSAS and altered cortisol levels has not been conclusively established [8]. Since nocturnal awakenings are associated with HPA axis activation and associated sympathetic activation it is expected that concentrations of cortisol could be higher in patients with OSAS [6]. However, many studies have failed to find differences in cortisol between OSAS subjects and normal controls [22]. Further, several studies have reported that Continuous Positive Airway Pressure (CPAP), the gold standard treatment for OSAS, does not reduce cortisol levels in patients with OSAS [23]. Finally, the removal of CPAP in OSAS patients has not been shown to result in immediate increases in cortisol levels [24]. Methodological concerns, such as infrequent sampling and inconsistent timing of sample collection, may have contributed to null findings for some studies. Recent studies using more extensive circadian sampling have reported differences in cortisol levels between OSAS patients and normal controls [10,11].
In our study we found an elevation in cortisol levels at night (p<0.05), while there were no significant differences in the morning, according to the results of Vgontzas et al. [11]. The absence of significant alterations in cortisol levels at 8.00 can be explained by the awakening response phenomena. The awakening response is the marked and rapid rise in cortisol and Adreno-Corticotropic Hormone (ACTH) that occurs after final morning awakening and continues for about a 60-min period, it is distinct from nocturnal awakenings and it is predictable and independent of the mode of awakening (naturally or with an alarm). It does not appear to be simply a continuation of the morning rise in cortisol or due to a wake-up stimulus. Spontaneous final awakening time is not linked to either a sleep stage or a specific cortisol level. Anticipation of awakening at a certain time can augment the early morning rise of cortisol that occurs before awakening. This effect is distinct from and has no impact on the subsequent cortisol awakening response [7].
The alteration of nocturnal cortisol levels might be important not only for the effects, mentioned above, that this hormone exerts on sleep, but also for the inhibitory activity that cortisol exerts on the secretion of the Growth Hormone (GH). It’s known that elevated cortisol levels cause a reduction in the secretion of GH [25], moreover, since the peak of GH secretion occurs during SWS [25], OSAS itself, causing shortened SWS time, could cause an altered GH secretion. In fact, in literature it has been reported that children with obstruction of the upper airway show growth defects due to a reduced secretion of GH, which is restored after adenotonsillectomy [26]. In particular, in subjects with deficient GH secretion a reduced posterior facial height was found, when compared to healthy controls of the same age, due to a reduced growth of the ramus. Other studies report that the administration of GH in these patients lead to an acceleration in the growth of the mandibular ramus. Hence, if the obstruction of the upper airway can represent, through the modified tongue position and the consequent stretching of the soft tissues, a mechanical cause in the development of craniofacial alterations, it can be hypothized that an increased nocturnal secretion of cortisol in OSAS patients could provide a metabolic cause (Figure 3).
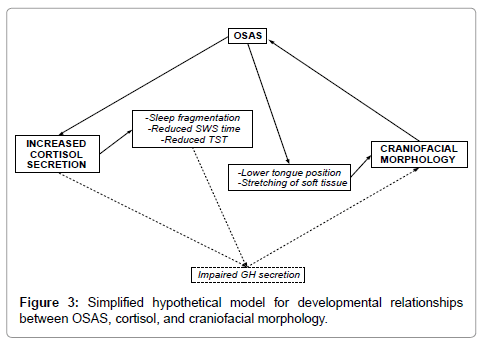
Figure 3: Simplified hypothetical model for developmental relationships between OSAS, cortisol, and craniofacial morphology.
Altered HPA axis activity and craniofacial modification are often found in OSAS children. We are not able to state whether if these conditions are causes rather than consequences of OSAS. It seems that they both present self-perpetuating vicious circles: in the former sleep fragmentation increase cortisol levels [6] and this increased HPA axis activity promotes sleep fragmentation itself [9], in the latter it is difficult to establish if the primary alteration is respiratory or maxillofacial [12,13]. Furthermore, due to the reduction of GH secretion caused by cortisol and sleep fragmentation, it can be assumed that, in OSAS subjects, the alteration of facial morphology may also have a metabolic cause. Independently of the primary cause of this vicious circle a multidisciplinary approach to OSAS children should be advisable.
The work was performed at the Department of Pediatrics and at the Department of Orthodontics, School of Medicine and Dentistry, University Of Insubria, Varese, Italy. All the authors declare the absence of any conflict of interest and financial support.