Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2014) Volume 2, Issue 1
Background: Most hip fractures are due to falls among frail elderly people. In order to formulate strategies to prevent falls leading to hip fracture, the characteristics of the falls of patients should be clarified in more detail. We investigate the fall situations of hip fracture patients.
Methods: The fall conditions of eighty female and seventeen male hip fracture patients with an average age of 82.3 y.o. who were admitted to the hospital of the National Center for Geriatrics and Gerontology, Japan over a two-year period were investigated by questionnaire concerning 1) the time of falling, 2) the place of falling, 3) what they were doing at the moment of falling, and 4) the cause of falling. Their Barthel Index, representing patients’ ADL capability before injuries, was obtained as well, and the relation between falling situations and the Barthel Index score was analyzed.
Results: The most frequent time, place, cause of the fall and activities at the time of the fall were in the evening (from 5 to 9 P.M.), in their own room, and involved their loss of balance and walking, respectively. Those who fell in the following situations had lower ADL capacity before injury: occurring at evening and night, either in the toilet or other places indoors and at falling, from losing their balance or slipping.
Conclusion: Fall situations causing hip fractures differed considerably with the hip fracture patients’ capacities before injury. These differences must be taken into careful consideration in order to formulate effective strategies in hip fracture prevention.
<Keywords: Fall situation; Hip fracture; ADL before injury
Prevention of hip fractures is a critical issue because it is one of the most common injuries which cause frail old people to become bedridden. Most of the hip fractures are due to falls of elderly people whose bones have become osteoporotic [1]. According to recent research reports of the Japanese Orthopedic Association, 70-80% of hip fractures occur by a fall from the standing position, and two-thirds of the falls take place inside the house [2]. This is actually quite different from the falls of general community dwellers, which occur mainly outside the house [3-5]. There have been several studies about the falls which lead to hip fracture but their situations have not been well investigated, and furthermore, most of the studies were done in Western countries [1,6-18]. Meanwhile, falls of generally healthy (or nearly healthy) old people have long been studied by many authors [3,5,19-30]. Most of those papers stress the importance of fall prevention [31]. But considering the differences between the two; fall prevention strategies for healthy (or almost healthy) old people in general may not necessarily be suitable for when targeting hip fractures. Thus, in order to develop a preventive method for hip fracture, a more detailed investigation should be made into the actual falling situations which haveresulted in the fracture. In the present study, we present the results of our investigations of fall situations in hip fracture patients and also describe the results of our analysis of the relations between fall states and their capability for Activities of Daily Living (ADL) before injury. The results of this study may thus be helpful in preventing hip fractures from the viewpoint of fall prevention.
Subjects
Subjects are patients who were admitted to the hospital of the National Center for Geriatrics and Gerontology (Obu, Aichi, Japan) for the treatment of proximal femoral fracture over a two-year period and gave their written informed consent to the investigation of their fall situations. Basically, study was designed to select consecutive patients during a certain two-year period, but since the fall situations were ambiguous in about a quarter of the patients, those cases were excluded, and 97 cases were included in this study. This number nearly equals 98 persons, which is calculated as an adequate sample size by the free software G*Power 3, when alpha was set at 0.05, power at 80%, and effect size at 0.4. Eighty cases (82.5%) were females and seventeen (17.5%) were males, and the average age of the patients was 82.3 y.o. (ranging from 55 to 98). Forty-five cases (46.4%) were right side fractures, 52 (53.6%) were left, 35 (36.1%) were femoral neck fractures, 61 (62.9%) trochanteric and 1 case (1.0%) was a subtrochanteric fracture. As for their living situation before injury, 65 cases (67.0%) lived at home, and 32 (33.0%) were nursing home residents. As for their walking ability before injury, 53 cases (54.6%) could go out by him (or her) self, 21 cases (21.6%) could walk independently only inside the house, 18 cases (18.6%) needed some aid or assistance for walking even indoors, and 5 cases (5.2%) lived only around their beds. The average Barthel index score, which represents the basic ADL capability was 79.7 points (± 24.2) (ranging from 5 to 100) [32]. The average MMSE score of the patients was 17.4 ponts (± 8.2) (ranging from 0 to 30).
Methods
Just at the time of the admission, together with the general information about patients, the fall situations were asked by a questionnaires concerning about four items, as follows: 1) time of fall (using four-hour interval starting at 1:00 A.M. thus classified into six periods; from 1:00 to 5:00 A.M., 5:00 to 9:00 A.M., from 9:00 A.M. to 1:00 P.M., from 1:00 P.M. to 5:00 P.M. 5:00 to 9:00 P.M., and 9:00 P.M. to 1:00 A.M. next day); 2) places of fall (own room, front entrance area of house, kitchen, toilet, other places inside - including stairways, dining room, meeting room etc., outside the house, and other); 3) activities in which the patient was variously engaged at the moment of falling (walking, sitting or standing, using upper limbs, bicycle riding, and other); and 4) the causes of falling (losing one’s balance, tripping, slipping and feeling faint).
Also, the patients’ ADL capabilities before injury were evaluated by the Barthel Index questionnaire, one of the most common methods of evaluating the basic ADL level for each of the following 10 items; Bowels, Bladder, Grooming, Toilet use, Feeding, Transfer, Mobility, Dressing, Stairs, and Bathing, summing up to 100 points. Answers to these questionnaires were provided by either the key persons, who mainly take care of the patients, or by the children or brothers or sisters, so that the information would be as reliable as possible. The patients’ cognition states were evaluated several times using the MMSE (Mini Mental State Examination) by a quailed clinical psychologist, and the best score was recorded.
In order to investigate the relation between fall situations and patients’ ADL capability before injury, their Barthel index scores were compared among groups of patients classified by the items listed above. The statistical analyses were performed using ANOVA, Bonferroni’s test utilizing Stat View 5.0.The study protocol was approved by the Committee on Ethics of Human Research of the National Institute for Longevity Sciences. Written informed consent was obtained from each subject.
Fall situations
As for the time of falling, the largest number of patients (26 persons, 27%) fell in the evening (from 5:00 P.M. to 9:00 P.M.), followed by the afternoon (from 1:00 P.M. to 5:00 P.M.) (Table 1a). As for the place, the greatest number (30 persons, 31%) fell in their own room, followed by the doorway to their home (14%), toilet (5%) and kitchen (3%). Sixteen percent of the patients fell at other places inside the house (Table 1b). As for their activities, the largest number (38 persons, 40%) were walking at the time they fell, followed by sitting or standing (26%), using their upper limbs (9%) while bicycle riding (5%) (Table 1c). Finally, the greatest cause of falling was loss of balance (35 persons, 36%), followed by tripping (18%), slipping (11%), or feeling faint (5%). Actually, in about 20% of the patients, the causes of falling were unknown (Table 1d).
| 1:00 A.M. - 5:00 A.M. | 9% |
| 5:00 A.M. - 9:00 A.M. | 11% |
| 9:00 A.M. - 1:00 P.M. | 13% |
| 1:00 P.M. - 5:00 P.M. | 20% |
| 5:00 P.M. - 9:00 P.M. | 27% |
| 9:00 P.M. - 1:00 A.M. | 4% |
| unknown | 15% |
Table 1a: Time of falling.
| own room | 31% |
| entryway to house | 14% |
| toilet | 5% |
| kitchen | 3% |
| elsewhere inside house* | 16% |
| outside | 18% |
| terrace | 2% |
| unknown | 11% |
*corridor, dining room, meeting room, etc.
Table 1b: Places of falling.
| walking | 40% |
| sitting or standing | 26% |
| using upper limb(s) | 9% |
| bicycle riding | 5% |
| standing upright | 2% |
| turning around | 2% |
| other | 6% |
| none of above | 2% |
| unknown | 8% |
Table 1c: Activities at the moment of falling.
| loss of balance | 36% |
| tripping | 18% |
| slipping | 11% |
| feeling faint | 5% |
| colliding | 2% |
| other | 8% |
| unknown | 20% |
Table 1d: Causes of falling.
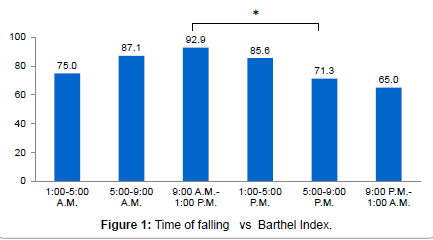
Figure 1: Time of falling vs Barthel Index.
Relation between fall situations and ADL capability before injury
Amongseveral groups classified by the time of falling, those who fell from 9:00 A.M. to 1:00 P.M. showed the highest average Barthel Index score, while those who fell after 5:00 P.M. until early morning presented a lower score. The difference between the 9:00 A.M. to 1:00 P.M. group and the 5:00 P.M. to 9:00 P.M. group was significant (P<0.05) (Figure 1). As to the places of falling, the average Barthel Index score of those who fell in toilet areas as well as those at other places inside the house presented a low Barthel Index score. On the other hand, high scores were obtained by those who fell outside as well as in the doorway to the house. The difference in the average score of (those who fell outside and at the doorway) and (those who fell in the toilet or elsewhere inside the house) was significant or nearly significant (Figure 2). As to what they were doing at the moment of falling, the score of those who fell during bicycle riding was high, but other than for that group, the Barthel Index was mostly low (Figure 3). As for the causes of falling, the score of those who lost their balance or slipped was low, whereas the score of those who tripped was high. And the difference in scores between those who tripped and those who lost their balance was significant (P<0.05), and between those who tripped and slipped was nearly significant (P=0.057) (Figure 4).
Hip fracture is one of the most devastating events for elderly persons who are injured in a fall, because they may become unable to walk due to the fracture, and the incidence has been still increasing in Japan. Thus, the prevention of such fractures is critical. In order to prevent hip fractures, it is important to develop effective strategies to prevent falls among elderly people, as well as to treat osteoporosis so as to strengthen weakened bone, because the majority of hip fractures are due to falls. Rigorous analysis of the falling events of actual hip fracture patients is indispensable to develop strategies for preventing them. In this paper, we investigated the fall situations of hip fracture patients in terms of time, place and activities at the moment of falling, and the causes of the fall. Although many investigations have been made about the fall events of hip fracture patients [1,6-16], but few have described the situations surrounding the falls in detail [7,8]. Also, most of those studies were done in western countries, largely in Caucasian subjects, and few papers have been published about Asian patients. Though the contents of the researched fall situations were different depending on the reported studies, especially regarding classification of the causes of falling, some results were similar to those obtained in the present study.
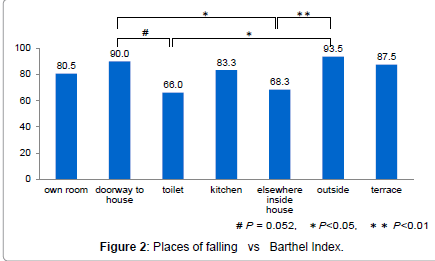
Figure 2: Places of falling vs Barthel Index.
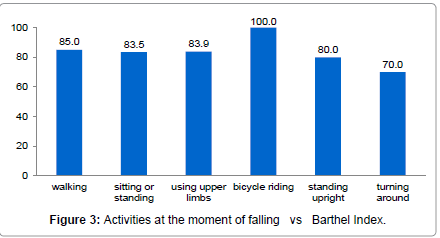
Figure 3:Activities at the moment of falling vs Barthel Index.
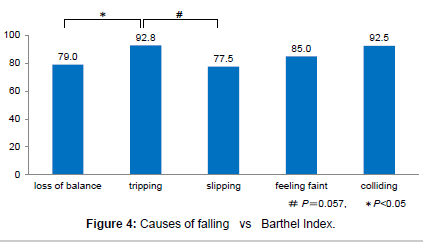
Figure 4:Causes of falling vs Barthel Index.
First of all, in almost all studies, the falls occur mostly indoors. And as for the time of falling, most falls occurred in the daytime and during walking which agreed with our results [7,9-12,14,16]. However, our study revealed more falls at doorways to the house, and most were caused by loss of balance, whereas in the literature, more patients fell by slipping or tripping. As for the reason so many falls occurred at the doorway in our study, the fact is that most Japanese houses have the usual step in the entryway where people take off their shoes (or slippers), step up (or down) or sometimes turn around. The change of footwear upon leaving/entering one’s home may also be one of the extrinsic risk factors in falling, which may be unique to Japanese culture. Moreover, the fact that loss of balance was the most common cause of falls may be because of the high average age of our Japanese subjects, namely.
Brocklehust et al. [13] reported that younger hip fracture patients fell more by tripping, whereas the older ones fell more due to loss of balance. As a matter of fact, tripping is the commonest reported cause of falls of normal (or nearly normal) elderly people living in the community worldwide [3-5,25,28]. Also, the majority of falling events of healthier persons occur outside of the house [3-5]. These statistics are in accordance with some of our findings that those who fell by losing their balance had lower ADL before injury and those who fell outdoors or fell by tripping had higher ADL before injury (Figure 4). As for the relation between ADL capabilities and other falling situations, we found that those who fell in the evening or at night, those who fell in the toilet and other indoor places, or by slipping, had lower ADL before injury, whereas those who fell at the entryway to their house had higher ADL before injury.
In our study we conducted a close investigation of the relations between fall states and the capability of ADL before injury. Some of the past reports describing the causes of fall situations did not distinguish between tripping and loss of balance [12], nor between tripping and slipping [32]. We found a difference among these causes at least from the standpoint of the ADL levels before injury. Namely, those who fell due to loss of balance had lower ADL, and this may imply that they had become frail with the weakening of their leg strength, which is required for maintaining their body balance. So far, in general, researchers have not dealt with the difference between tripping and slipping, probably because they are considered to have a similar meaning as extrinsic factors relating to the foot region. But our results would suggest that the reason for falling by tripping or slipping may be different. Those who fell by tripping had a higher ADL than those by slipping. This result accords well with the fact that the commonest cause of falling among the healthy (or nearly healthy) general community dwellers is tripping as mentioned before. But considering that tripping was not the most frequent cause of falling among the hip fracture patients, in order to formulate prevention strategy against falling (leading to the hip fracture event) it should be important to pay attention not merely to avoid obstacles around one’s feet or increase foot clearance [33], but also to avoid wearing slippery shoes or walking on slippery floors, as well as improving one’s balance, as by strengthening their leg power. Thus, such detailed information about hip fracture patient situations made good use of the hip fracture prevention attitude, suggesting that the strategy for preventing ordinary healthy people from mere falling may not be good enough to prevent fracture.
The limitation of the present study is that the selected subjects were not consecutive, because those cases whose fall situations were ambiguous were excluded. In up to a quarter of the cases the falling situations were not recognized either by patients or the people around them. Also, internal validity may be compromised by the system used for subject selection in which cases with ambiguous fall situations were excluded, and also by the lack of response of some subjects, particularly about the cause of falling, which was as high as 20%. We could not avoid this situation when conducting the study on the subjects whose average MMSE score was as low as 17.4, this may be why this kind of survey about the falling situation in hip fracture cases has been little reported. Also, the issue of developing comprehensive strategies to prevent falling of demented elderly may be more difficult. This is also the case in recommending the wearing of hip protectors [34-36].
In summary, among patients who suffered hip fracture, those who fell in the evening or at night, in the toilet and other places inside, and those who fell due to loss of balance and slipping had lower ADL capacities before injury. These points should be taken into careful consideration in formulating strategies to prevent falls leading to hip fractures in the frail elderly.
This study was funded by The Research Fund for Longevity Sciences from the National Center for Geriatrics and Gerontology (NCGG), Japan [22,23].