Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 3
About 30% of Canadian workers are on shift work schedules, and 8% to 32% of them suffer from Shift Work Disorder (SWD). Only a few behavioural treatments exist to treat this population. This study explores the efficacy and feasibility of sleep restriction therapy for insomnia in a group of night shift workers. Six participants (3 women) meeting SWD criteria were recruited. Mean age was 45.7 years old (SD=8.2). A multiple baseline design was used. After baseline, each participant received six to eight weekly treatment sessions. They completed several selfreported questionnaires and a daily sleep diary throughout the study. For each sleep period, sleep variables were calculated from the sleep diary. Two participants had a high treatment response and all others participants had a moderate response. Moreover, all participants presented at least two significant clinical improvements. Five participants presented a decreased in both sleepiness scores. The study suggests that sleep restriction therapy is effective, feasible, and reliable. Sleep restriction therapy for insomnia could improve sleep and diminish sleepiness in shift workers suffering from SWD. The present study opens new possibilities of treatment for shift workers that deserve greater attention in the future.
Keywords: Shift work; Insomnia; Behavioural therapy; Pilot study
Shift work is a reality of our contemporary industrial world. Indeed, this work schedule involves approximately 28% of the Canadian work force [1]. Unfortunately, shift work can be accompanied by various problems such as sleep difficulties. When those sleep difficulties are insomnia or excessive sleepiness associated with the work schedule, they are called Shift Work Disorder (SWD) [2]. It is estimated that about 8% to 32% of shift workers [3-5] suffer from SWD. Specific negatives consequences are linked to SWD. For instance, it is associated with an increased risk of depression, morbidity and gastric ulcers [3], cardiovascular disease, cancer, reproductive troubles [6] and a decrease in quality of life [4,5,7]. Furthermore, it has a negative socio-economic impact as it is associated with increased absenteeism at work and to an increase in accidents caused by sleepiness [8] or insomnia [9]. Furthermore insomnia in the context of shift work seems to contribute to an aggravation of the overall clinical picture of shift workers [9]. Current interventions for SWD focus predominantly on alleviating sleepiness and increasing alertness in re-entraining the circadian rhythm. Most of the available treatments are pharmacological, such as hypnotics used to improve sleep [10,11], stimulants used to improve alertness [12,13], or luminotherapy used with or without dark sunglasses to shift the circadian rhythm at least partially to thereby improve sleep and alertness [14,15]. Other studies have evaluated the effect on the sleep of night workers, of a nap before [16-18] or during the night work [19,20]. Among all the interventions presently offered to shift workers, some provide improvement on either sleep or alertness but they fail to improve the whole symptomatology of SWD [21] and none of them, except hypnotics, specifically address insomnia in shift work. Furthermore, all pharmacological agents possess, the danger of developing physiological or sychological dependencies on medication, some provide insomnia rebound effects during withdrawal of the medication, and can also interfere with the sleep architecture [22]. Moreover, most of the studies evaluating intervention for SWD did not use specific diagnostic criteria [23] and only a few were conducted with a real shift worker population. Non pharmacological treatments for insomnia such as CBT-I are recommended as a standard treatment for chronic insomnia [24].
CBT-I includes stimulus control therapy, sleep restriction therapy, relaxation training, sleep hygiene education and cognitive therapy [24-26]. Two studies have attempted to improve sleep in shift work with CBT-I [27-29]. In the first one, a nonrandomized group of 26 shift workers received seven sessions of CBT-I while 21 shift workers in the second one received a home-based cognitive-behavioral intervention for insomnia. Both studies show sleep improvement. More specifically, participants of the first study improved on sleep onset latency and sleep efficiency while participants of the second study improved on sleep quality. Perceived insomnia severity as well as sleep-related dysfunctional beliefs also improved in Jarnefelt et al. [27] whereas emotional distress decreased in the other study [29]. These two first studies [27,29] are a very promising step in addressing insomnia in shift work. However, several issues related to the methodology and to the intervention itself might limit the conclusions. The most important problem concerns the fact that no clinical interview was conducted to ascertain the diagnosis. CBT-I had been developed for chronic insomnia, which is a specific disorder. To know its efficacy in a shift work population, it should be evaluated within a shift worker population suffering from SWD with insomnia. Also, several aspects of the CBT-I assessed in the two studies may hide the real treatment effect. Indeed, numerous changes from the original content of CBT-I were made, the CBT-I was delivered as a package and in two different formats. Moreover, the designs used did not allow any control for spontaneous change. Therefore, it is impossible to know to what part of the treatment might have been responsible for improvements, and what would be the real effect of CBT-I on sleep in a clinical population.
The work schedule can lead to an insomnia different from that of people sleeping by night. These differences can be in terms of when insomnia occurs in a 24 h period, as well as why it occurs or is maintained. The etiology of insomnia in shift work has not yet been documented. Nothing is known regarding conditioning process, sleep habits, beliefs or cognitive processes involved in shift work insomnia. Consequently, in order to adapt a CBT-I to shift workers, each component of CBT-I should be evaluated separately to know the component of CBT-I that needs to be applied, when it should be applied, and which works best as a function of the work schedule. Among the behavioral therapies for insomnia, sleep restriction therapy should be useful for shift workers as it uses the process of sleep homeostasis to improve sleep. The objective of sleep restriction therapy is to facilitate and consolidate sleep, using and regulating homeostatic sleep pressure [30,31]. Indeed, the sleep homeostasis mechanism of shift workers is known to be deregulated and to contribute to their level of sleepiness. Therefore, a better management of this pressure through sleep restriction therapy should have a beneficial effect on sleep. This study aims at exploring the efficacy of sleep restriction therapy adapted for SWD including insomnia symptoms. More specifically, it is expected that sleep onset latency will decrease for sleep, and sleep efficiency will increase after treatment for all participants. The study also evaluates the feasibility and the treatment acceptability among shift workers.
Participants
Participants were recruited through press releases in local media, advertising in hospitals and through participation in another study at the Centre d’étude des troubles du sommeil (CETS) of the Institut universitaire en santé mental de Québec (IUSMQ). Inclusion criteria were: (a) being over 18 years old; (b) being a shift worker (work a minimum of eight nights per month); (c) working at least four hours between 24:00 and 8:00 and (d) reporting a sleep disorder related to the work schedule as defined by the ICSD-II [2]. The criterion of 8 nights per month was chosen to ensure that sleep difficulties were related to the work schedule. Exclusion criteria were: (a) being unable to answer questions during interviews or being unable to respond to questionnaires; (b) being unable to go to the sleep laboratory; (c) being blind; (d) travelling more than one hour to get home after work; (e) having traveled over three time zones in the last month; (f) presenting a severe psychological disorder such as major depression; (g) presenting alcohol or substance abuse; (h) presenting another possible sleep disorder such as sleep apnea or periodic limb movement; (i) using hypnotics on a regular basis in the last month and (j) drinking over 10 cups of coffee (or other stimulants) per day. The study was approved by the IUSMQ ethical committee (#185). Eight eligible participants responded to recruitment publicity and underwent telephone screening. Subsequently, they went through a multi-step screening evaluation, which includes two pre-treatment interviews. One participant was then excluded because sleep apnea was suspected and another one was no longer interested in the study. The final sample included six participants (3 men and 3 women). The mean age of participants was 45.7 years (ranging from 38 to 57 years old). The average duration of sleep difficulties was 15.3 years (ranging from 1 to 30 years) and the average duration of shift work was 11.4 years (ranging from 0.7 to 20 years). Participants 2, 3, 4 and 5 completed all the assessment phases. Participant 1 left shift work at week 5: at that moment, the treatment strategies concerned nocturnal sleep only. Participant 6 dropped out of the study at week 6 of the treatment without giving any reason. Participants’ main characteristics are summarized in Table 1. Follow-up data are available for participant 2, 3, and 5 only.
Design
A single case design called multiple baseline across subjects design [32] was used to explore the efficacy of the sleep restriction therapy for shift workers with SWD. This particular single case design provides a controlled investigation of treatment mechanisms [33]. Baseline length has to be different for each participant to ensure that the introduction of the experimental treatment occurs at a different time for each participant. This particularity of the design provides a control for possible maturational or spontaneous changes. Maturation refers to natural changes over time of a participant’s sleep that occurs without treatment. Figure 1 illustrates the design, showing a different baseline length for each participant.
Procedure
Before entering the study, participants were instructed to maintain their typical sleep habits. The study was conducted in French. At baseline and throughout the study, participants completed several self-report measures in French and continuous assessments of their sleep and sleepiness. Three months after the end of treatment, participants were as asked to complete the self-report measures about sleep, fatigue, depression, and anxiety.
Measures
Initial screening and evaluation: Initial screening consisted of a 20-minute telephone interview to determine participant eligibility. Subsequently, two pre-treatment interviews were conducted: a semi-structured psychological interview (SCID-IV evaluation) [34] and a sleep history interview adapted from the IIS (Insomnia Interview Schedule [35]) and the Standard Shift Work Index [35,36] to evaluate the presence of psychological disorders and sleep difficulties.
Sleep diary: Participants completed sleep diaries upon awakening after each sleep period. From these diaries Total Sleep Time (TST), Wake After Sleep Onset (WASO), Sleep Onset Latency (SOL), and Sleep Efficiency [SE; ratio of TST divided by Time in Bed (TIB)] were derived for each participant for diurnal and nocturnal sleep. Sleepiness according to the Stanford Sleepiness Scale [37] was also recorded in the sleep diary. Participants rated their level of sleepiness/alertness using a 7-point Likert scale (ranges from "1" to "7"). Higher scores represent a greater degree of sleepiness. This questionnaire is widely used in sleep and shift work population studies.
Questionnaires
Dysfunctional beliefs and attitudes about sleep-16: (DBAS-16 [38]) assesses with 16 items four domains of beliefs and attitudes regarding sleep: (a) misattribution or amplification of the causes of insomnia; (b) sleep concerns; (c) unrealistic sleep expectations and (d) faulty beliefs about insomnia consequences. Each item is scored on Likert-type scale ranging from "1" to "10". Higher scores indicate a high level of misconceptions and bad attitudes related to sleep. The psychometric properties of the French version are well documented in an insomnia population [38,39].
Glasgow content of thoughts inventory: (GCTI; [40]) assesses with 25 items the nature and frequency of intrusive thoughts at bedtime. Each item is scored on Likert-type scale from "1" to "4" and the total score ranges between "25" to "100". Higher scores indicate a high degree of intrusive thoughts at bedtime. The psychometric qualities of the French version have not yet been evaluated.
The multidimensional fatigue inventory: (MFI; [41]) assesses with 20 items global fatigue and five related domains: (a) general fatigue; (b) mental fatigue; (c) physical fatigue; (d) reduced motivation, and (e) decreased activity. Higher scores indicate a more severe fatigue. This French version of the questionnaire has good psychometric qualities [42] and is frequently used in an insomnia population.
Beck depression inventory: (BDI-II; [43]) assesses with 21 items the presence and severity of depressive symptoms within the last two weeks. Each item is scored on scale from "0" to "3" and total score ranges between “0” and “63”. Higher scores indicate a greater symptom severity. This questionnaire is widely used and the psychometric qualities of the French version are well established [43].
State-trait anxiety inventory: (STAI-Y; [44]) assesses with 20 items state and trait anxiety. Each item is scored on a Likert-type scale ranging from "1" to "4". Higher scores indicate a high level of anxiety. The psychometric properties of the French version of the STAI-Y are excellent and well documented [45].
Compliance and acceptability measures: Compliance to behavioral procedure was computed from the sleep diaries. A weekly percentage of adherences to the prescribe time to go to bed as well as to arising time were computed separately for each participant and sleep episode. Nonadherence was considered as going to bed more than 15 minutes earlier and getting out of bed more than 15 minutes later than the prescribed nocturnal and diurnal sleep window. Moreover, more than 30 minutes of the prescribed TIB was also considered as nonadherance. There were then six criteria to be respected: three for nocturnal sleep and three for diurnal sleep. For each criterion, a score of 1 was assigned when it was respected and a score of 0 if not. For each day the maximum score was 3. Daily scores were computed, divided by the total expected score and multiplied by 100. The total expected score is based on the assumption that the participant had entirely respected the procedures.
Treatment acceptability scale: (TAS; [46]) This 4-item scale assesses participants’ perceptions of treatment acceptability. Each item is scored on Liker-type scale from "1" to "10". Higher scores indicate a high degree of acceptability of treatment. The psychometric qualities of the French version have not yet been evaluated.
The sleep restriction therapy adapted to shift work and administered in this study is outlined in a treatment manual [47]. Use of the manual ensures treatment fidelity and facilitates treatment standardization and replication. The treatment includes five or six 50-minute individual consultation sessions. The first four sessions were administered weekly while the following two were at every two weeks. The content and aims of the sleep restriction therapy are summarized in Table 2. The treatment went from steps 1 to 3 where in step 1 sleep restriction was applied to night sleep, in step 2 to day sleep, and in step 3 to naps. At each step criterion SE level was reached before going to the next step. Therefore, the number of treatment session to reach criterion and pass to the next step could vary among participants. During the sleep restriction therapy, the first meeting with participants served to provide participants with information about sleep and its regulatory mechanisms, while the following meetings discussed the maintenance of therapeutic gains.
The content and aims of the sleep restriction sessions are summarized in Table 2. Sleep restriction therapy consists of curtailing the time spent in bed to conform to the reported amount of time asleep. A sleep window is determined using the average of TST reported by participants in their baseline weeks of sleep diaries. The sleep window is increased by 15-30 minutes, contingent upon reaching a SE of 85% or more. When SE is between 80% and 85%, the sleep window is kept stable and when SE is lower than 80%, the sleep window is [14], bedtimes for daily sleep were set close to the time that participants arrived home after their work shift. The lower limit of the sleep window is five hours. An educational component including basic facts about sleep and circadian rhythm is included in the treatment. Sleep restriction is applied first to night sleep and then to day sleep. Treatment sessions are conducted by a graduate student in psychology (EBD) and supervised by a clinical psychologist (AV).
The five dependent variables were derived from sleep diaries for nocturnal and diurnal sleep. Mean comparisons at each stage (baseline and post-treatment) were performed to determine the magnitude of change of nocturnal and diurnal sleep. Clinically significant change criteria, based on expected results obtained with CBT-I, were used to determine the clinical value of the change [48]. For WASO and SOL, the reduction at post-treatment must be between 50 and 60% compared to baseline. TST increases must be between 30 and 45 minutes at post-treatment, SE must be greater than 85% and sleepiness must decrease. Subsequently, treatment response was evaluated using the following criteria: (a) and (b) respectively, reduction of diurnal and nocturnal WASO or SOL greater than 50% at post-treatment; (c) and (d) respectively, increase of diurnal and nocturnal TST greater than 30 to 45 minutes at post-treatment; (e) and (f) respectively, diurnal and nocturnal SE greater than 85%; (g) and (h) respectively, diminution of nocturnal and diurnal sleepiness scores.
With CBT-I, one can reasonably expect a improvement of 75% of the problem for those with chronic insomnia [49]. Since there are eight criteria, an amelioration for at least six criteria would represent the expected 75% improvement. Treatment response is considered "high" when at least six criteria are met, "moderate" if three to five criteria are met and "low" if fewer than three criteria are met.
A nonparametric one-tailed test was used to assess the significance of responses after treatment. The questionnaire data were visually analyzed and described, confidence intervals were computed on the mean difference from post to baseline. Cronbach alpha consistency was measured for the two self-report questionnaires without French validation (GCTI and TAS) [50].
Figures 1 and 2 illustrate daily changes in the percentage of nocturnal and diurnal sleep efficiency and total sleep time during each phase of the study (baseline, treatment and posttreatment) for each participant. The figures show night-to-night variability for nocturnal sleep and diurnal sleep, confirming the presence of insomnia.
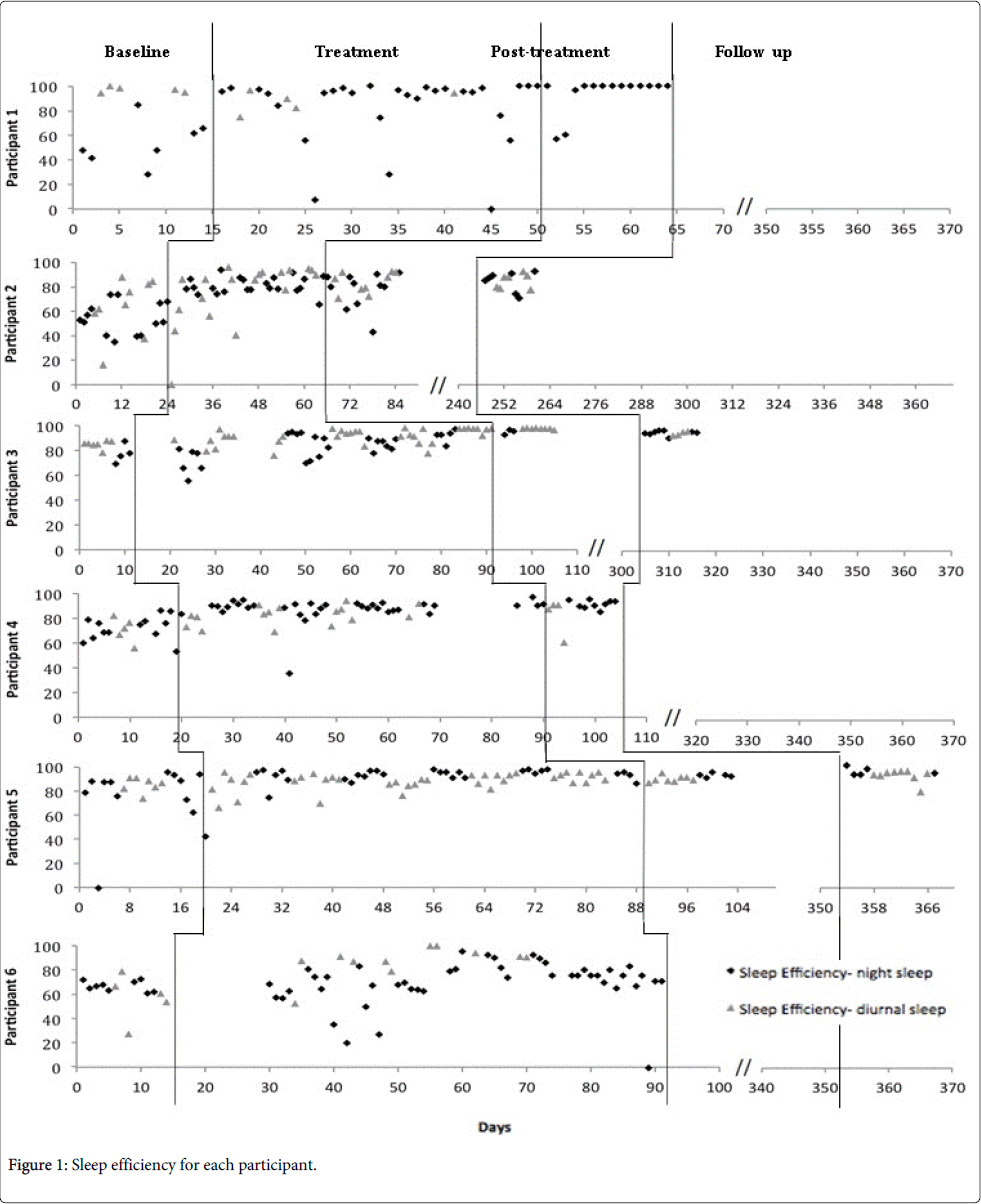
Figure 1: Sleep efficiency for each participant.
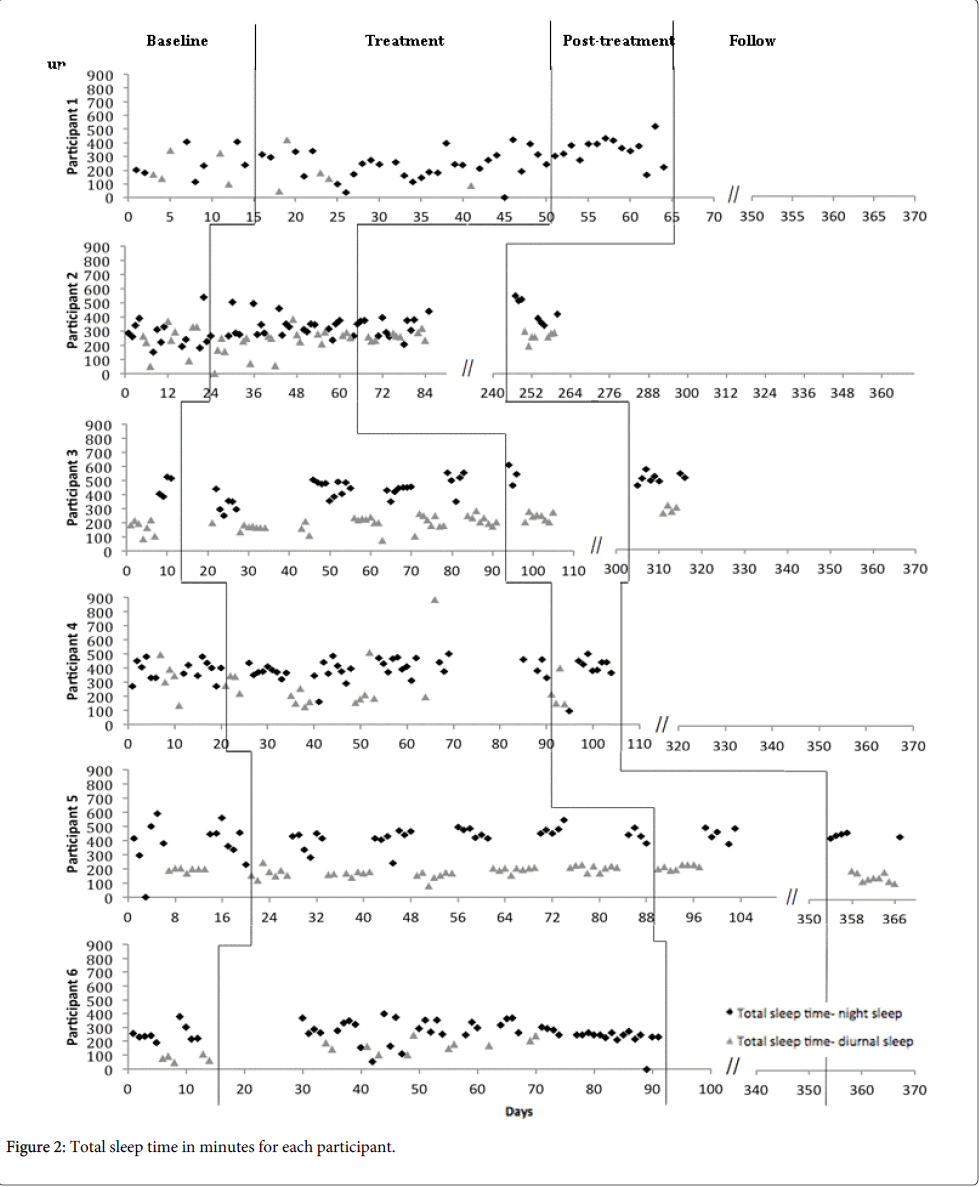
Figure 2: Total sleep time in minutes for each participant.
Moreover, the figures show that no changes in sleep occurred before treatment introduction, for each participant and sleep variable, indicating an adequate control in this respect. The internal consistency of the GCTI at baseline and posttreatment is excellent, with Cronbach alphas of .95 and .92, respectively. For the TAS, internal consistency is excellent at baseline and good at post-treatment with Cronbach alphas of 0.94 and 0.88, respectively.
Participant 1
Participant 1 was a man of 38 years old with sleep difficulties since beginning night work a year previously (Table 1). Before treatment, diurnal SOL and WASO were low while nocturnal SOL and WASO were respectively 25.6 and 72.3 minutes. Diurnal and nocturnal TST were 214.2 and 247.5 minutes, respectively. Diurnal SE was high but nocturnal SE was 52.6%. Diurnal and nocturnal sleepiness scores were 1.7 and 2.1, respectively (Tables 3 and 4).
| Participant | Age/Gender | Duration of shift work (years) | Duration of sleep difficulties (years) | Nature of sleep complaint |
| 1 | 38/M | 1 | 1 | Initiation, maintenance &prematuretermination |
| 2 | 43/F | 20 | 12 | Prematuretermination |
| 3 | 57/F | 0.7 | 5 | Maintenance &prematuretermination |
| 4 | 42/F | 20 | 20 | Initiation & maintenance |
| 5 | 39/M | 10 | 24 | Maintenance &prematuretermination |
| 6 | 55/M | 6 | 30 | Maintenance |
Table 1: Summary of participants’ characteristics (Note. F: Female; M: Male; (-): missing data).
| Steps | Treatment guidelines |
| 1: night sleep | Addressing insomnia symptoms occurring during night sleep |
| • Applying sleep restriction therapy using a sleep window as for insomnia | |
| • Once average sleep efficiency for night sleep reaches 85% then go to step 2 | |
| 2: day sleep | Addressing insomnia symptoms occurring during day sleep |
| • Applying sleep restriction using a sleep window as for insomnia | |
| • Once average sleep efficiency for day sleep reaches 85% then go to step 3 | |
| 3: naps | Addressing naps |
| • Scheduled naps using sleep restriction therapy and a sleep window | |
| • Length and timing of naps should be adapted to lifestyle habits and without interfering with sleep homeostasis process | |
| General recommendation with sleep restriction |
• The sleep window for each sleep period should be adjusted after computing the sleep efficiency of each sleep period. |
| • The time for going to bed, whether night sleep, day sleep or nap, should be determined regarding lifestyle habits and as a function of the sleep homeostatic drive. | |
| Recall | Sleep restriction therapy for insomnia |
| • Determined a sleep window length (time for going in and out bed) based on the total sleep time average | |
| • Modify the sleep window following these rules: | |
| • Increase of the sleep window if sleep efficiency is ≥ 85% | |
| • Decrease of the sleep window if sleep efficiency is < 80% | |
| • Otherwise maintain |
Table 2: Summary of sleep restriction adapted for insomnia in shift work.
| Participant 1 | Participant 2 | Participant 3 | Participant 4 | Participant 5 | Participant 6 | |||||||||||||
| Sleep parameters | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U |
| Sleep onset latency | ||||||||||||||||||
| Diurnal sleep | 5.0 | n/a | n/a | 14.2 | 10.7 | 10.4 | 12.1 | 5.0 | 5.0 | 24.0 | 11.3 | n/a | 6.2 | 10.6 | 15.4 | 7.9 | n/a | n/a |
| Nocturnal sleep | 25.6 | 1.8 | n/a | 13.3 | 11.0 | 11.3 | 18.8 | 6.3 | 7.5 | 32.2 | 15.4 | n/a | 25.8 | 22.1 | 7.7 | 9.8 | n/a | n/a |
| Number of awakenings | ||||||||||||||||||
| Diurnal sleep | 0.0 | n/a | n/a | 0.7 | 0.2 | 0.3 | 1.0 | 0.0 | 0.7 | 3.4 | 3.5 | n/a | 1.0 | 0.4 | 0.3 | 1.5 | n/a | n/a |
| Nocturnal sleep | 0.9 | 0.1 | n/a | 2.2 | 0.6 | 1.6 | 2.3 | 1.5 | 0.4 | 4.6 | 2.3 | n/a | 0.8 | 0.8 | 1.3 | 3.0 | n/a | n/a |
| Wake after sleep onset | ||||||||||||||||||
| Diurnal sleep | 0.0 | n/a | n/a | 11.3 | 1.1 | 1.7 | 10.7 | 0.0 | 6.7 | 66.0 | 26.3 | n/a | 30.4 | 22.2 | 15.6 | 49.4 | n/a | n/a |
| Nocturnal sleep | 72.3 | 34.3 | n/a | 31.9 | 8.0 | 7.9 | 97.5 | 12.5 | 4.2 | 78.3 | 38.1 | n/a | 51.7 | 45.0 | 50.6 | 139.6 | n/a | n/a |
| Total sleep time | ||||||||||||||||||
| Diurnal sleep | 214.2 | n/a | n/a | 193.3 | 213.9 | 175.0 | 167.1 | 242.1 | 303.3 | 333.0 | 227.5 | n/a | 242.8 | 264.4 | 297.7 | 119.0 | n/a | n/a |
| Nocturnal sleep | 247.5 | 348.9 | n/a | 432.2 | 447.0 | 492.1 | 457.5 | 540.0 | 560.8 | 385.3 | 345.8 | n/a | 286.3 | 334.2 | 505.6 | 265.7 | n/a | n/a |
| Time in bed | ||||||||||||||||||
| Diurnal sleep | 220.4 | n/a | n/a | 229.6 | 237.9 | 192.1 | 196.4 | 247.5 | 315.0 | 456.0 | 272.5 | n/a | 367.2 | 318.9 | 352.5 | 188.7 | n/a | n/a |
| Nocturnal sleep | 470.6 | 385.0 | n/a | 511.7 | 479.0 | 526.9 | 588.8 | 570.0 | 575.0 | 521.7 | 429.6 | n/a | 533.8 | 427.9 | 598.8 | 415.1 | n/a | n/a |
| Sleep efficiency (%) | ||||||||||||||||||
| Diurnal sleep | 97.2 | n/a | n/a | 84.2 | 89.9 | 91.1 | 85.1 | 97.0 | 96.0 | 73.0 | 83.5 | n/a | 65.2 | 83.2 | 84.4 | 66.2 | n/a | n/a |
| Nocturnal sleep | 52.6 | 91.6 | n/a | 84.9 | 93.3 | 93.4 | 77.7 | 95.0 | 97.5 | 74.0 | 91.9 | n/a | 53.6 | 78.0 | 84.1 | 64.2 | n/a | n/a |
Table 3: Sleep measures across assessment phases for individual participants.
After treatment, there was a clinical significant change for all criteria of nocturnal sleep. Indeed, nocturnal SOL and WASO decreased by 93.0% and of 52.6%, respectively while TST increased by 101.4 minutes, SE increased to 91.6%. Diurnal sleepiness decreased by 0.5 point. Participant 1 had an increased level of general fatigue. Intrusive thoughts at bedtime increased also, but the level of endorsement of dysfunctional beliefs and attitudes about sleep remained low. Depression and anxiety increased slightly (Table 4). Participant 1 did not complete the follow-up assessment. Finally, participant 1 had a moderate response to treatment, meeting all criteria for nocturnal sleep (criteria b, d, f, and h) but only one criterion for diurnal sleep (criterion g) (Tables 3 and 4). Participant 1 moderately accepted treatment and had diurnal and nocturnal sleep compliance of 55.6% and 58.7%, respectively (Table 5).
| Participant 1 | Participant 2 | Participant 3 | Participant 4 | Participant 5 | Participant 6 | |||||||||||||
| Questionnaires | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U | Pre | Post | F/U |
| GCTI | 38 | 47 | n/a | 42 | 33 | 29 | 60 | 44 | 43 | 48 | 29 | n/a | 82 | 60 | 68 | 75 | n/a | n/a |
| DBAS | 2.4 | 2.4 | n/a | 1.3 | 2.6 | 2 | 5.1 | 3 | 2.7 | 3.9 | 3.3 | n/a | 5.7 | 5.5 | 5 | 6.1 | n/a | n/a |
| MFI | 41 | 53 | n/a | 53 | 29 | 26 | 40 | 45 | 31 | 35 | 25 | n/a | 76 | 60 | 68 | 50 | n/a | n/a |
| BDI | 2 | 4 | n/a | 4 | 0 | 0 | 21 | 10 | 6 | 3 | 0 | n/a | 30 | 19 | 21 | 20 | n/a | n/a |
| STAI-Y | ||||||||||||||||||
| State anxiety | 31 | 27 | n/a | 35 | 32 | 21 | 34 | 29 | 28 | 33 | 21 | n/a | 43 | 56 | - | 40 | n/a | n/a |
| Trait anxiety | 24 | 33 | n/a | 31 | 36 | 23 | 36 | 31 | 29 | 31 | 24 | n/a | 59 | 49 | - | 49 | n/a | n/a |
| Sleepiness | ||||||||||||||||||
| Diurnal sleep | 1.7 | n/a | n/a | 2.5 | 4.2 | 3.5 | 3.3 | 2.4 | 2 | 3.4 | 1 | n/a | 3.2 | 2.4 | 2.4 | 3.2 | n/a | n/a |
| Nocturnal sleep | 2.1 | 1.6 | n/a | 2.9 | 3.4 | 2 | 1.5 | 1 | 1.3 | 3.3 | 1.2 | n/a | 3.5 | 1.4 | 1.6 | 3.1 | n/a | n/a |
Table 4: Total score on questionnaire across assessments phases (Note. GCTI: Glasgow Content of Thoughts Inventory; DBAS: Dysfunctional Beliefs and Attitudes about Sleep; MFI: Multidimensional Fatigue Inventory, BDI: Beck Depression Inventory; STAI-Y: State-Trait Anxiety Inventory; Pre: Pre-treatment; Post: Post-treatment, F/U: Follow-up; n/a: Not Applicable; (-): Missing Data).
| Statements | Participant 1 | Participant 2 | Participant 3 | Participant 4 | Participant 5 | Participant 6 | ||||||
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Acceptance of treatment | 5 | 7 | 8 | 10 | 5 | 8 | 6 | 10 | 9 | 9 | 10 | n/a |
| Expected short-termeffect | 5 | 8 | 7 | 10 | 6 | 9 | 7 | 10 | 9 | 8 | 10 | n/a |
| Expected long-termeffect | 7 | 5 | 8 | 10 | 7 | 7 | 7 | 10 | 8 | 9 | 10 | n/a |
| Treatment satisfaction | n/a | 7 | n/a | 10 | n/a | 9 | n/a | 10 | n/a | 8 | n/a | n/a |
| Mean total score | 5.7/10 | 6.8/10 | 7.7/10 | 10-Oct | 6/10 | 8.3/10 | 6.7/10 | 10/10 | 8/10 | 8.5/10 | 10/10 | n/a |
Table 5: Treatment acceptability (Note: Pre: Pre-treatment; Post: Post-treatment; n/a: Not Applicable).
Participant 2
Participant 2, a woman of 43 years old, had been a shift worker for 20 years and complained of sleep difficulties for 12 years (Table 2). Before treatment, the diurnal and nocturnal SOL and nocturnal WASO were less than 15 minutes while the nocturnal WASO were 31.9 minutes. Diurnal and nocturnal TST were 193.3 and 432.2 minutes and diurnal and nocturnal SE were 84.2% and 84.9% respectively. Nocturnal and diurnal sleepiness scores were 2.5 and 2.9 respectively (Tables 3 and 4). At post-treatment, diurnal WASO decreased by 90.3% and SE increased by 6.8%. TST increased by 20.6 minutes. Nocturnal sleepiness increased 1.7 points. Nocturnal WASO decreased by 74.9% and post-treatment SE increased by 9.9%. Diurnal TST increased by 14.8 minutes. Diurnal sleepiness increased by 0.5 points (score 3.4) (Table 3). Participant 2 had a decreased level of general fatigue at post-treatment. Intrusive thoughts at bedtime decreased, but level of endorsement of dysfunctional beliefs and attitudes about sleep increased. Depression and state anxiety decreased, but trait anxiety increased (Table 4). Most sleep improvement was maintained at the 3-month follow-up except for diurnal TST that decreased to baseline level (Table 3). Nocturnal TST increased while diurnal and nocturnal WASO remained low. Intrusive thoughts at bedtime, endorsement of dysfunctional beliefs about sleep, fatigue, depression, and anxiety remained at the post-treatment level (Table 4). Diurnal sleepiness decreased at follow-up but remained higher than baseline. Finally, participant 2 had a moderate treatment response, meeting four criteria (criteria a, b, e, and f) for diurnal sleep (a and e) and two for nocturnal sleep (b and f). Participant 2 readily accepted treatment but her compliance rate is missing (Table 5).
Participant 3
Participant 3, a woman of 57 years old, had been a night worker for 8.5 months, but had had sleep difficulties for 5 years (Table 2). Before treatment, diurnal SOL and WASO were less than 20 minutes while nocturnal SOL and WASO were of 18.8 and 97.5 minutes, respectively. Diurnal and nocturnal TST were 167.1 and 457.5 minutes, respectively, and diurnal and nocturnal SE were 85.1% and 77.7%. Nocturnal and diurnal sleepiness were of 3.3 and 1.5, respectively (Tables 3 and 4). After treatment, diurnal SOL and WASO decreased by 58.7% and 100%, respectively, while TST increased by 75 minutes. SE presented an increase of 14.0% and nocturnal sleepiness decreased by 0.9 point (Tables 3 and 4). For nocturnal sleep changes, SOL and WASO decreased by 66.5% and 87.2%, respectively, while TST increased by 82.5 minutes. SE increased by 22.3%. Diurnal sleepiness decreased by 0.5 point (Tables 3 and 4). Participant 3 presented an increase in general fatigue at post-treatment, while intrusive thoughts at bedtime, and level of endorsement of dysfunctional beliefs and attitudes about sleep decreased. The levels of depression and anxiety also decreased (Table 4). Finally, participant 3 had a high treatment response meeting all criteria for diurnal and nocturnal sleep. Participant 3 accepted treatment, having diurnal and nocturnal sleep compliances of 85.4% and 84.0%, respectively (Table 5). Most sleep improvement was maintained at the 3-month follow-up (Table 3). Diurnal and nocturnal TST further increased at the 3-month follow-up compared to post-treatment. Intrusive thoughts at bed time, endorsement of dysfunctional beliefs about sleep, depression, and anxiety remained at the post-treatment level (Table 4). Fatigue presents an additional decrease compare to post-treatment.
Participant 4
Participant 4, a woman of 42 years old, had been a shift worker for 20 years, with sleep difficulties during that whole time (Table 2). Before treatment, diurnal and nocturnal SOL were about 30 minutes, while diurnal and nocturnal WASO were 66.0 and 78.3 minutes, respectively. Diurnal and nocturnal TST were 333.0 and 385.3 minutes, respectively. Diurnal and nocturnal SE were of 73.0 and 74.0% and nocturnal and diurnal sleepiness of 3.4 and 3.3 (Tables 3 and 4). Participant 4 did not complete the follow-up assessment. After treatment, diurnal SOL and WASO decreased by 52.9% and of 60.2%, respectively, and sleepiness decreased by 2.4 points. Meanwhile, TST decreased of 105.5 minutes. Nocturnal SOL and WASO decreased respectively by 52.2% and 51.3%, and sleepiness decreased by 1.1 points. Post-treatment nocturnal SE increased by 24.2%. (Tables 3 and 4) and TST decreased by 39.5 minutes. Participant 4 had a decreased level of general fatigue at post-treatment: intrusive thoughts at bedtime, level of endorsement of dysfunctional beliefs and attitudes about sleep, and depression and anxiety levels also decreased (Table 4). Finally, participant 4 had a moderate response to treatment, meeting five criteria (criteria a, b, f, g, and h). Participant 4 accepted treatment, having diurnal and nocturnal sleep compliances of 45.0% and 66.4% respectively (Table 5).
Participant 5
Participant 5, a man of 39 years old, was a night worker for 10 years and had sleep difficulties for 24 years (Table 2). Before treatment, the diurnal and nocturnal SOL were 6.2 and 25.8 minutes while the diurnal and nocturnal WASO were 30.4 and 51.7 minutes. Diurnal and nocturnal TST were 242.8 and 286.3 minutes and diurnal and nocturnal SE were 65.2% and 53.6%. Nocturnal and diurnal sleepiness were 3.2 and 3.5, respectively (Tables 3 and 4). After treatment, there were clinically significant changes for two criteria of nocturnal sleep; nocturnal TST increased by 47.9 minutes and diurnal sleepiness decreased by 2.1 point. There was also a 0.8 point decrease in nocturnal sleepiness (Tables 3 and 4). Participant 5 had a decreased level of general fatigue. Intrusive thoughts at bedtime decreased also, as well as the level of dysfunctional beliefs and attitudes about sleep. The level of depression and trait anxiety decreased while state anxiety increased (Table 4). Most sleep improvement was maintained at the 3-month follow-up (Table 3). Diurnal and nocturnal TST further increased at the 3-month follow-up compared to post-treatment. Nocturnal WASO remained at baseline. Intrusive thoughts at bedtime, endorsement of dysfunctional beliefs about sleep, depression, and sleepiness remained at the post-treatment level (Table 4). Finally, participant 5 accepted treatment, having a diurnal and nocturnal sleep compliance of 80.0% and 78.3%, respectively (Table 5). This participant had a moderate treatment response, meeting three criteria (criterion d, g, and h).
Participant 6
Participant 6 was a man of 55 years old. He had been a rotated shift worker for 6 years and complained of sleep difficulties for 30 years (Table 2). Before treatment, the diurnal and nocturnal SOL were less than 10 minutes while the diurnal and nocturnal WASO were 49.4 and 139.6 minutes, respectively. Diurnal and nocturnal TST were 119.0 and 265.7 minutes and diurnal and nocturnal SE were 66.2% and 64.2% respectively. Nocturnal and diurnal sleepiness scores were 3.2 and 3.1, respectively (Tables 3 and 4). Participant 6 did not complete the follow-up assessment.
Participant 6 dropped out of the study at the end of treatment and before post-treatment. When he dropped out of treatment his diurnal WASO decreased by 64.6%, TST increased by 106.0 minutes. SE increased by 37.4%, and diurnal sleepiness decreased by 0.2 points. Nocturnal WASO decreased by 52.5% and diurnal sleepiness decreased by 0.5 point. Nocturnal TST remained unchanged. At that time, participant 6 had a high treatment response, meeting six criteria (a, b, c, e, g, and h) (Tables 3 and 4). Finally, participant 6 readily accepted treatment (Table 5) but his compliance rate is missing.
Summary of treatment response
Two of the six participants (3 and 6) had a high treatment response, one of them meeting all criteria (Table 6). All others participants had a moderate response to treatment. Moreover, all participants presented at least two significant clinical improvements, one in diurnal and one in nocturnal sleep. Five participants presented a decrease in both sleepiness scores. Only one participant showed no WASO improvement. All participants, except one, presented at least one increase in SE. Four participants presented an increase in at least one TST. SOL is the sleep variable showing the least improvement. Given that all six participants had a moderate to high treatment response, the nonparametric sign test provided a significant one tailed p-value of 0.0156 (6 successes out of 6 trials).
| Participant | Sleepparameters | Diurnal sleep Criterion met no/yes | Nocturnal sleepCriterion met no/yes | Treatment response |
| 1 | SOL/WASO (⇓50-60%) | no (⇑ 266.6%)/no(⇑ +400%) | Yes (⇓93.0%)/ Yes (⇓52.6%) | 5/8 : 62.5%; moderate |
| TST (⇑30-45min) | no (⇓ 74,87min) | Yes (⇑101.4min) | ||
| SE (⇑85%) | no (76.12%) | Yes (91.6%, ⇑74.1%) | ||
| Sleepiness (⇓) | Yes (⇓0.7pt) | Yes (⇓0.5pt) | ||
| 2 | SOL/WASO (⇓50-60%) | no (24.6%)/Yes (⇓90.3%) | no (⇓ 17.3%)/Yes (⇓74.9%) | 4/8 : 50%; moderate |
| TST (⇑30-45min) | no (⇑20.6min) | no(⇑14.8min) | ||
| SE (⇑85%) | Yes (89.9%, ⇑ 6.8 %) | Yes (93.3%, ⇑ 9.9%) | ||
| Sleepiness (⇓) | no(⇑ 1.7pt) | no (⇑ 0.5pt) | ||
| 3 | SOL/WASO (⇓50-60%) | Yes (⇓58.7%)/ Yes (⇓100%) | Yes (⇓66.5%)/ Yes (⇓87.2%) | 8/8 : 100%; high |
| TST (⇑30-45min) | Yes (⇑75.0min) | Yes (⇑82.5min) | ||
| SE (⇑85%) | Yes (97.0%, ⇑14.0%) | Yes (95%, ⇑22.3%) | ||
| Sleepiness (⇓) | Yes (⇓0.9pt) | Yes (⇓0.5pt) | ||
| 4 | SOL/WASO (⇓50-60%) | Yes (⇓52.9%)/ Yes (⇓60.2%) | Yes (⇓52.2%)/ Yes (⇓51.3%) | 5/8 : 62.5%; moderate |
| TST (⇑30-45min) | no (⇓ 105.5min) | no (⇓ 39.5min) | ||
| SE (⇑85%) | no (83.5%) | Yes (91.9%, ⇑24.2%) | ||
| Sleepiness (⇓) | Yes (⇓2.4pt) | Yes (⇓1.1pt) | ||
| 5 | SOL/WASO (⇓50-60%) | no (⇑ 71%)/no (⇓27%) | no (⇓ 14.3%)/ no (⇓13%) | 3/8 : 37.5% moderate |
| TST (⇑30-45min) | no (⇑21.6min) | Yes (⇑47.9 min) | ||
| SE (⇑85%) | no (83.2%) | no (78.0%)) | ||
| Sleepiness (⇓) | Yes (⇓0.8pt) | Yes (⇓2.1pt) | ||
| 6 | SOL/WASO (⇓50-60%) | no (⇓ 36.7%)/Yes (⇓64.6%) | no (⇓ 29%)/ Yes (⇓52.5%) | 6/8 :75%; high |
| TST (⇑30-45min) | Yes (⇑106.0min) | no (⇑1.47min) | ||
| SE (⇑85%) | Yes (90.93%, ⇑37.4%) | no (78.3%) | ||
| Sleepiness(⇓) | Yes (⇓0.2pt) | Yes (⇓0.5pt) |
Table 6: Treatment response of each participant for diurnal and nocturnal sleep (Note: SOL: Sleep Onset Latency; WASO: Wake After Sleep Onset; TST: Total Sleep Time; SE: Sleep Efficiency; ⇑: Increase of; ⇓: Decrease of; pt: Point; min: Minute).
Mean of the difference scores from post-treatment to baseline for self-report questionnaires indicate negative change for all questionnaires except for TAS. These changes are in the expected direction, meaning that symptoms assessed improved with treatment and that treatment is more acceptable after treatment than before. Confidence intervals indicate non-significant changes except for TAS (Table 7).
| Questionnaires | n | Mean of difference | CI |
| GCTI | 5 | -11.4 | [-26.77, 4.0] |
| DBAS | 5 | -0.35 | [-1.86, 1.2] |
| MFI | 5 | -6.6 | [-25.05, 11.9] |
| BDI-II | 5 | -5.2 | [-11.85, 1.5] |
| STAI-Y | |||
| State anxiety | 5 | -2.2 | [-13.63, 9.2] |
| Trait anxiety | 5 | -1.6 | [-11.75, 8.5] |
| TAS | 3 | 45.33 | [22.25, 68.4] |
Table 7: Mean difference scores for self-reported questionnaires and confidence intervals (Note: GCTI: Glasgow content of thoughts inventory; DBAS: Dysfunctional beliefs and attitudes about sleep; MFI: Multidimensional Fatigue Inventory; BDI-II: Beck Depression Inventory; STAI-Y: State-Trait Anxiety Inventory; Mean of Difference: Mean of Difference Score between Post and Pre-treatment).
The findings of this study suggest that sleep restriction therapy adapted to treat SWD with insomnia symptoms is feasible and effective. All participants presented sleep improvement, the most frequently observed being a decrease in WASO. Moreover, either diurnal or nocturnal TST increased while subjective sleepiness decreased for five participants. Nocturnal and diurnal SE increased or remained over 85% for most of participants. The majority of participants reported a decrease in intrusive thoughts while falling asleep. Depression and anxiety levels were improved or remained low for five participants as shown by the difference scores between post and pretreatment. Most of the improvement remained stable at follow-up; these measures were available for only half of the participants. Furthermore, the treatment was well accepted by participants while compliance rates were moderate. Taken together, these preliminary results suggest that shift workers with SWD may benefit from a direct intervention targeting insomnia symptoms. They also underline the importance and relevance of addressing night and day sleep for shift workers. Overall, these results converge with those reported by Jarnefelt et al. [27] and Lee et al. [29] who use a CBT-I in a population of shift workers. The first study demonstrated some improvement on SOL and SE while sleep quality improved for participants of the second study. The present study seems to show even more sleep improvement regarding WASO and TST. These results are probably due to the fact that our participants received a diagnosis of SWD based on a clinical interview, which was not the case in the two previous studies. In other words, they were more likely to improve because they were more severely disrupted before treatment. Results for nocturnal sleep are very interesting, showing that the sleep improvement obtained compares with that seen in other studies using sleep restriction therapy for day workers [30,31]. Results on TST are highly promising and deserve attention. Indeed, several of our participants presented an increase in TST or a stable TST for nocturnal and diurnal sleep. The increase in TST obtained for diurnal sleep varies from 20.6 to 106 minutes while nocturnal TST varies from 1.5 to 101.4 minutes. These results are unexpected for several reasons. First, the range of increases obtained seems to be higher than that reported in other interventions for shift workers. For instance, wearing dark sunglasses has been shown to increase diurnal TST by an average of 25 minutes [15] while luminotherapy has been shown to produce an increase of about 30 minutes for shift workers [51]. Second, in the present study TST increased in a way comparable to what is expected for TST after sleep restriction therapy for day workers. In fact, with a population sleeping by night, TST is expected to diminish in the first weeks of treatment and increase again later after treatment [31,52]. Furthermore, although sleepiness is a known side effect of sleep restriction [30,31,52], nearly all our participants improved on sleepiness. Taken together, these results suggest that insomnia responds faster to sleep restriction therapy in SWD than in day workers. Also, these results suggest that at least part of the sleepiness in shift work seems to be related to TST. Finally, these results underline the importance of having a well diagnosed population to evaluate treatment efficacy. Sleep restriction therapy used alone seem also to have an effect on psychological distress. Results on depression and anxiety levels show clearly that most participants benefit from treatment. Intrusive thoughts at bedtime seem highly present before treatment and their diminution constitutes another improvement observed for most participants following sleep restriction. Interestingly, our study shows that a specific insomnia treatment might produce mood relief even if the intervention does not specifically address depression. Again, these results are in line with Jarnefelt et al. [27] and Lee et al. [29]. The feasibility of sleep restriction for SWD is also demonstrated in the present study. First of all, sleep restriction therapy was well accepted by the participants as shown by the scores obtained on the treatment acceptability scale. Second, results on TST and sleepiness also support the feasibility of sleep restriction therapy, showing that there are no potential side-effects such as have been observed with day workers with insomnia. In addition, most of participants completed the treatment sessions. The greatest obstacle to sleep restriction therapy we faced were changes in the participants’ work schedule, changes which are more related to workplace constraints than to the treatment itself. Subsequent assessments such as post-treatment and follow-up were more difficult to obtain. This situation could reflect the fact that, due to their work schedule, the workers have less time for meetings or participation in a demanding study. Finally, the compliance data showed that treatment procedures were moderately followed. This last result might negatively affect treatment efficacy and feasibility. The question of compliance in this population should be taken into account in other studies. The present study suggests guidelines as well as some methodological issues. The first and most important is that this study shows the usefulness of assessing nocturnal and diurnal sleep for shift workers. It is clear that sleeping by both day and night is part of the reality of shift workers, and that they benefit from addressing both periods of sleep during treatment. In addition, it appears that several questionnaires assessing insomnia components need to be adapted to shift work in order to capture insomnia during diurnal sleep as well. Another methodological issue rising from the present study regards the use of semi-structured clinical interviews that ascertain the diagnosis of the population studied. This methodology presents two advantages. First, it ascertains the presence of the disorder to be studied in the population, decreasing interpretive biases. Second, sleep restriction therapy, as CBT-I, is a treatment developed and tested for a specific disorder, which is insomnia. Therefore, it is likely to be effective within other populations having a specific disorder with insomnia symptoms. These preliminary results possess also some methodological limitations. First, the absence of a control group limits the interpretation of the results as nonspecific factors cannot be separated. Second, given the small sample size the study needs to be replicated in larger sample size. Doing so, a randomized design with a control group would be mandatory. Third, long-term effects of treatment were difficult to assess. Future studies should have reliable follow-up data to confirm the long term efficacy of sleep restriction therapy for shift workers. In addition, sleep diaries are subjective measures and, although important, the absence of more objective measures precludes definite conclusions about objective sleep changes. Finally, the lack of measure of the circadian rhythm markers precludes any conclusions about the circadian misalignment of shift workers and its possible realignement due to sleep restriction therapy. In conclusion, the present study is one of the first evaluating a specific intervention for insomnia in a shift workers population diagnosed for SWD. The preliminary results obtained are promising, showing that sleep restriction therapy adapted for SDW produces sleep, sleepiness, and mood benefits. Further studies should investigate side-effects of sleep restriction therapy for shift workers to clarify the surprising results of an increase in TST and a decrease in sleepiness. Future studies could also consider adding stimulus control therapy for insomnia in shift workers as it is known for its efficacy and commonly used with sleep restriction therapy for insomnia. After a specific investigation of cognition for shift workers, cognitive interventions could be added to the treatment protocol and evaluated as well. In conclusion, the present study opens a new possibility of treatment for shift workers that deserves greater attention in the future.
This research was supported by a grant from the Faculté des sciences sociales of Université Laval and from the Research center of the Institut universitaire en santé mentale de Québec. The authors wish to thank Dr. James Everett for English revision.