Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2015) Volume 3, Issue 1
Purpose: Whole-body vibration (WBV) is new type of exercise that is being increasingly performed to prevent bone fractures and osteoporosis in frail people. Whether WBV plays an important role in positive skeletal responses of premenopausal women is controversial. The aim of this study was to determine the effects of 6 months of supervised WBV and high-impact aerobics (HIA) on bone metabolism and body balance in pre-menopausal women.
Methods: Sixty-seven eligible premenopausal women were stratified into three groups: the WBV training group (n = 23), HIA training group (n = 22), and control group (n = 22). The subjects in both training groups participated in a supervised training program involving three sets of 3-minute exercise sessions three times a week for 6 months. The WBV group received vibration in a static standing position. The HIA group jumped rope. Bone-related factors and body balance were compared at baseline and 6-month intervals.
Results: Comparison of the percent changes of the variables showed that WBV and HIA at the stimulus level of the current study had no superior effect on the bone metabolism of healthy premenopausal women compared with controls. However, comparison of the absolute changes between baseline and the 6-month intervention showed a couple of positive findings in all groups.
Conclusions: Our data suggest that higher exposures of isolated WBV than those used in the current study or WBV plus various types of HIA training might be needed to improve the bone metabolism and body balance in premenopausal women.
<Keywords: Whole-body vibration; High-impact aerobics; Bone metabolism; Body balance; Pre-menopausal women
Maintaining an optimal body composition, including optimal Bone Mineral Density (BMD) levels, muscle strength, and muscle volume, during the premenopausal years is important to reduce the risk of osteoporosis and subsequent fractures during the postmenopausal years. While pharmacologic therapy is usually contraindicated in premenopausal women, lifestyle modification is almost always recommended [1]. One potentially effective lifestyle approach for achieving this goal is exercise, which is a low-cost, nonpharmacologic intervention that is available to the vast majority of the population. Whole-body vibration (WBV), defined as exercise performed with the body in contact with a vibrating platform, is new type of exercise that has been increasingly performed to prevent bone fractures and osteoporosis mainly in frail people [2-14]. WBV can be separated into two training stimuli: the reflex muscle contraction induced by vibration, and the body-weight exercise performed on the platform. As reported by previous studies [2-17], the WBV stimulus is well-tolerated by both younger and older female subjects, and no adverse side effects have been reported. WBV at 25–45 Hz appears to be a safe and effective mode of enhancing muscular strength in variety of populations [3].
Some studies have reported the effects of various approaches such as resistance training [13], proprioceptive training [12], walking [6,8], fitness training [4], and conventional training or wellness controls [14] on body composition compared with the effects of isolated WBV training. Other studies have reported the effects of resistance training [3], physical therapy [5], or routine exercise [2,7,9,11] with or without WBV. Most of them reported effects of WBV that were superior or equal to those of the other training. For example, Gusi et al. [6] reported that WBV is feasible and more effective than walking to improve hip BMD and balance. WBV training is as efficient as a fitness program to increase isometric and explosive knee extension strength and muscle mass of the upper leg [4]. Finally, von Stengel et al. [14] concluded that training including WBV resulted in a significantly lower number of falls than experienced by the wellness control group. However, most of these studies included only postmenopausal women or occasionally both women and men [2,4,5,7,9]. To the best of our knowledge, only a couple of studies [15-17] have reported the effects of WBV on bone metabolism in healthy premenopausal women.
Therefore, the aim of this study was to determine the effects of 6 months of supervised WBV and High-Impact Aerobic (HIA) exercises on bone-related variables and body balance in premenopausal women.
This was a prospective comparative study. Informed consent, including a description of the protocol and potential measuring devicerelated complications, was obtained from all patients. We also received institutional review board approval. All subjects were assigned to one of three study groups. Because most of the subjects had an occupation, we did ensure to some degree that the study protocol did not disturb their work to minimize the number of drop-outs during stratification. Sixty-seven eligible premenopausal women (27–50 years of age) were stratified into three groups: the WBV training group (n = 23), HIA training group (n = 22), and control group (n = 22) (Figure 1).
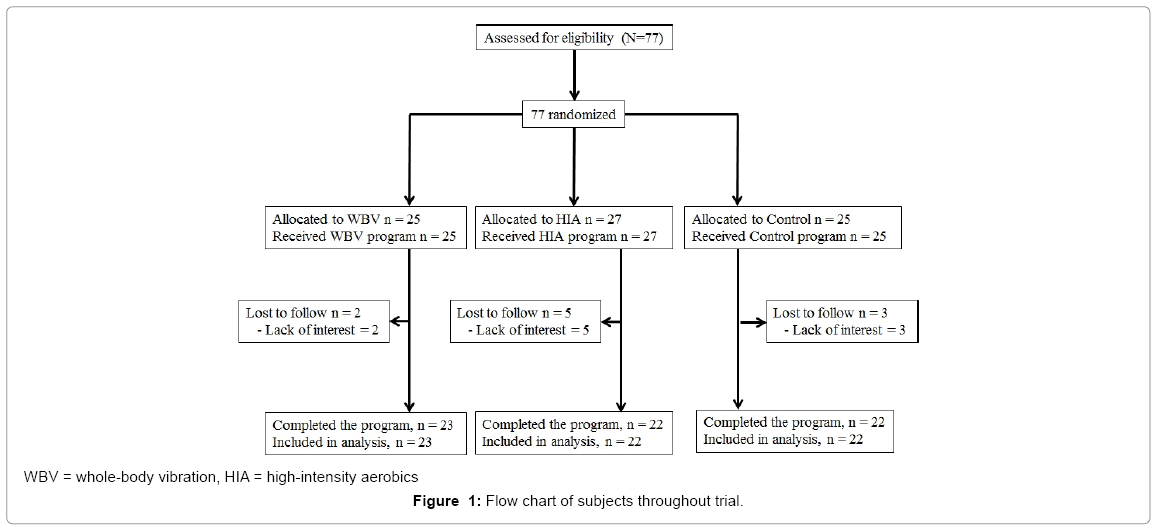
Figure 1: Flow chart of subjects throughout trial.
The characteristics of the 67 subjects, who completed all tests, are given in Table 1. No significant differences in age, weight, height, or Body Mass Index (BMI) among groups were detected as the start of the study (Table 1). The exclusion criteria were any cardiovascular, respiratory, abdominal, urinary, gynecological, neurological, musculoskeletal, or other chronic diseases; prostheses; medications that could affect the musculoskeletal system; menstrual irregularities; and participation in impact-type exercise more than three times a week. None of the subjects had been taking medications in the last 6 months that could potentially interfere with the evaluations carried out in the study.
| WBV | HIA | Control | p value | |
|---|---|---|---|---|
| Age (years) | 36.0 (29.0, 43.0) | 42.0 (38.0, 45.0) | 37.5 (32.0, 43.3) | 0.080 |
| Height (cm) | ||||
| Baseline | 158.0 (156.0, 162.0) | 156.5 (152.3, 160.8 ) | 160.5 (155.5, 165.0) | 0.075 |
| 6 months | 158.0 (156.0, 162.0) | 156.5 (152.3, 160.8 ) | 160.5 (155.5, 165.0) | |
| p value | 1.000 | 1.000 | 1.000 | |
| Weight (kg) | ||||
| Baseline | 55.0 (50.3, 61.8) | 51.5 (50.3, 54.8) | 54.0 (50.3, 56.0) | 0.491 |
| 6 months | 53.7 (48.6, 61.8) | 51.4 (50.1, 54.8) | 52.9 (50.1, 57.2) | |
| p value | 0.372 | 0.173 | 0.715 | |
| BMI (kg/m2) | ||||
| Baseline | 21.8 (20.3, 23.0) | 21.0 (19.8, 23.2) | 20.6 (19.9, 21.7) | 0.321 |
| 6 months | 21.4 (19.8, 23.0) | 20.7 (19.8, 23.2) | 20.8 (20.1, 21.8) | |
| p value | 0.355 | 0.218 | 0.768 | |
WBV: Whole-body vibration; HIA: high-impact aerobic; BMI: Body mass index
Table 1: Basic Characteristics of the Subjects.
Training protocol
The subjects in both training groups participated in a supervised training program, which involved three sets of 3-minute exercise sessions three times a week for 6 months. The WBV group received vibration (27 Hz, 2–2.8 G, 4.3-mm amplitude) in a static standing position with 20° of knee flexion. The WBV was received with a G-fleX (Canon Lifecare Solutions Inc., Osaka, Japan). The HIA group jumped rope (9 minutes of jumping per day) with a No. 91-130 jump rope (Asics, Kobe, Japan). The number of jumps during the index time depended on the ability of each subject. Finally, the control group was repeatedly advised not to change their lifestyle or physical activity during the project. All factors below were compared at baseline and 6-month intervals.
Evaluation of bone-related factors
In all subjects, the BMD of the total hip and lumbar spine (L1- 4) was measured with a Lunar Prodigy densitometer (GE Medical Systems, Lunar, Madison, WI). The coefficient of variation of replicant measurements in the same subjects is 1% [18]. Broadband ultrasound attenuation (BUA; dB/MHz) and speed of sound (SOS; m/s) through the calcaneus were measured to assess the bone quality of patients using an AOS-100SA (Hitachi-Aloka Medical, Ltd., Tokyo, Japan). The reported coefficient of variation of replicant measurements in the same subjects is less than 2% [19]. Measurement of dual-energy X-ray absorptiometry through the total hip and lumbar spine (L1–4), BUA, and SOS through the calcaneus was performed using the standard protocols of these devices. One of various markers of bone resorption, such as the level of urine N-terminal type I collagen telopeptides (NTx/ Cre), was investigated (standard value, 9.3–54.3 nmol BCE/mmol Cre). The second urine in the morning was measured at each evaluation.
Body balance
Using a gravicorder (Gravicorder GS-11; Anima, Tokyo, Japan), postural sway (cm) (caused as the body tries to balance) was measured for 30 s at 2-min intervals during two-leg standing with eyes open. The subjects stood barefoot, placing their feet on the center of the measurement field at a reference point on the examination platform. In the test with eyes open, the subjects fixed their gaze at a visual point placed 1 m in front of them at eye level so that no moving objects could enter the visual field. No device was used to prevent falling. The measured parameter of postural sway was the locus length per time, which indicates the postural control function by the proprioceptive reflex [20]. Three measurements were made, and the average of the three measurements was used for evaluation.
Statistical analysis
One-way analysis of variance (ANOVA) (Kruskal–Wallis method) and repeated-measures ANOVA (Scheffé’s method) were used to test for differences among the groups at baseline and for the rate of change among the groups. Changes between baseline and 6-month intervals in each group were compared using Wilcoxon’s signed-rank test. In all tests, a p-value of <0.05 was considered to be statistically significant. Statistical analyses were performed using IBM SPSS Statistics version 19 (IBM Japan Inc., Tokyo, Japan).
The WBV and HIA intervention was successful and safe. In the vibration group, the reported mean vibration training attendance was 2.7 ± 0.6 times per week (the planned minimum was three times per week). In the rope-jumping group, the reported mean rope-jumping training attendance was 2.5 ± 0.8 times per week (the planned minimum was three times per week). No vibration- or jumping-related side effects or adverse reactions were observed.
The comparison of baseline parameters (before the intervention) among the groups did not show significant differences (Tables 1 and 2), with the exception of the hip BMD (p = 0.009 by Kruskal–Wallis method), between HIA and WBV (p = 0.012 by Scheffé’s method) (Table 2).
| WBV | HIA | Control | p value | ||
|---|---|---|---|---|---|
| SOS (m/s) | |||||
| Baseline | 1549.0 (1537.0, 1567.0) | 1546.5 (1529.8, 1553.0) | 1546.0 (1534.8, 1557.8) | 0.446 | |
| 6 months | 1551.0 (1535.0, 1569) | 1542.5 (1535.8, 1556.5) | 1541.5 (1531.0, 1557.0) | ||
| p value | 0.615 | 0.685 | 0.088 | ||
| BUA(dB/ MHz) | |||||
| Baseline | 67.7 (56.6, 75.2) | 59.4 (55.0, 67.7) | 64.9 (54.3, 71.5) | 0.369 | |
| 6 months | 68.4 (64.6, 78.4) | 67.4 (57.7, 74.8) | 70.5 (60.2, 79.1) | ||
| p value | 0.078 | 0.101 | 0.001 | ||
| BMD (L1-L4; g/cm2) | |||||
| Baseline | 1.175 (1.105, 1.278) | 1.206 (1.101, 1.269) | 1.216 (1.139, 1.285) | 0.678 | |
| 6 months | 1.189 (1.133, 1.290) | 1.207 (1.097, 1.277) | 1.220 (1.157, 1.294) | ||
| p value | 0.186 | 0.062 | 0.041 | ||
| BMD (Total Hip; g/cm2) | |||||
| Baseline | 0.943 (0.835, 0.994)# | 0.815 (0.756, 0.883 )# | 0.883 (0.822, 0.970) | 0.009* | |
| 6 months | 0.920 (0.857, 0.996) | 0.823 (0.766, 0.916 ) | 0.878 (0.824, 0.960) | ||
| p value | 0.082 | 0.256 | 0.236 | ||
| NTX/Cre (nmol BCE/mmol Cr) | |||||
| Baseline | 23.6 (17.7, 28.5) | 23.6 (19.2, 33.8) | 27.5 (22.3, 38.4) | 0.297 | |
| 6 months | 26.6 (16.9, 32.7) | 25.5 (22.2, 39.1) | 28.7 (22.0, 36.5) | ||
| p value | 0.186 | 0.211 | 0.783 | ||
| Body Balance (cm) | |||||
| Baseline | 28.1 (21.8, 33.0) | 27.1 (21.9, 34.0) | 26.0 (22.8, 31.8) | 0.921 | |
| 6 months | 28.3 (19.5, 34.4) | 24.7 (20.9, 28.8) | 22.8 (21.4, 25.2) | ||
| p value | 0.605 | 0.017 | 0.006 | ||
#p = 0.012
WBV: Whole-body vibration; HIA: high-impact aerobic; SOS: Speed of Sound; BUA: Broadband Ultrasound Attenuation; BMD: bone mineral density; L: lumbar spine; NTx: N-terminal type I collagen telopeptides; Cre: creatinine
Table 2: Bone-Related Evaluation and Body Balance at Baseline and After the 6-Month Intervention Period.
Body balance
The absolute values of body balance improved significantly in the HIA and control groups (Table 2). However, the comparison of the percent changes of each value in three groups did not show significant differences (Table 3).
| WBV | HIA | Control | p value | |
|---|---|---|---|---|
| Body Composition | ||||
| Height | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.0) | 1.000 |
| Weight | -0.2 (-3.4, 1.5) | -0.9 (-2.5, 1.3) | -1.7 (-0.1, 1.9) | 0.442 |
| BMI | -0.2 (-3.4, 1.5) | -0.9 (-2.5, 1.3) | -0.1 (-1.7, 1.9) | 0.442 |
| Body Balance | ||||
| Locus of Gravity Center | -5.9 (-14.5, 14.2) | 7.8 (-20.5, 3.4) | -9.8 (-30.5, 1.1) | 0.146 |
| Bone-related factors | ||||
| SOS | 0.1 (-0.6, 0.3) | 0.1 (-0.6, 0.6) | -0.3 (-0.6, 0.2) | 0.382 |
| BUA | 6.3 (-3.4, 11.7) | 5.3 (-4.1, 19.5) | 6.7 (2.9, 17.7) | 0.519 |
| BMD (L1-4) | 0.7 (-1.1, 2.6) | 0.4 (-0.7, 2.2) | 1.0 (-0.6, 2.3) | 0.929 |
| BMD (Total hip) | 0.6 (-0.4, 1.8) | 0.7 (-1.3, 3.4) | 0.5 (-2.6, 1.5) | 0.243 |
| NTX/ Cre | 13.3 (-24.7, 49.1) | 17.6 (-11.4, 32.8) | -1.6 (-13.9, 34.9) | 0.827 |
#p = 0.032
WBV: Whole-body vibration; HIA: high-impact aerobic; BMI: Body mass index; SOS: Speed of Sound; BUA: Broadband Ultrasound Attenuation; BMD: bone mineral density;
L: lumbar spine; NTx: N-terminal type I collagen telopeptides; Cre: creatinine
Table 3: Comparison of Percent Change in Each Value in the Three Groups Between Baseline and After the 6-Month Intervention Period.
Bone measurements and biochemical markers of bone turnover
Although the absolute values of the BUA and BMD (L1–4) showed significant improvement only in the control group (Table 2), the percent changes did not show significant differences among the groups (Table 3). There were no significant differences in both the absolute values and the percent changes of NTx/Cre in three groups (Tables 2 and 3).
The most important finding of this study was that compared with the control group, the WBV and HIA programs with the amount of stimulus used in the current study did not have a superior effect on the bone metabolism of healthy premenopausal women. However, the comparison of the absolute values between baseline and the 6-month intervention showed a couple of positive findings in each group.
This study has some limitations. First, because we intended to minimize the number of drop-outs in each group by taking the participants’ occupational backgrounds into account, this study was not defined as a randomized controlled study. Therefore, this study could have subject selection bias. The subjects selected the group that best fit their working schedule. As a result, 87% (67 of 77) could be followed-up. In addition, no significant differences in age, weight, height, or BMI among the groups were detected at the start of the study. Second, with regard to the comparison of baseline values among the groups, there was a significant difference in the hip BMD between the HIA and WBV groups, although the others did not show significant differences. We did not consider such a difference to have a crucial influence on the results of the current study because the hip BMD did not reveal a significant difference between baseline and the 6-month intervention in each group, and additionally hip BMD of the percent change did not have significant differences among the groups. Third, we did not control dietary intake, such as calcium, vitamin D, or protein, which may have influenced the results in the three groups. Actually, it is very difficult for subjects who had an occupation to check and control their diet in detail. Despite the above limitations, a major strength of this study is that we revealed the effects of WBV and HIA on bone metabolism not in postmenopausal women, as previously reported [3,6,8,10-14], but in premenopausal women [15-17].
We recognized that the significant findings of the absolute values in the control group between baseline and the 6-month intervention, such as the body balance, BUA, and BMD (L1–4), might be induced by the increased activities of daily life (at baseline measured in December [winter season: estimated less activity] and at the 6-month intervention evaluated in July [summer season: estimated more activity]) because no additional load to the bone was ordered in the control group during the index period. In addition, the absolute values of the positive findings between baseline and the 6-month intervention, such as body balance in HIA might not be regarded as positive effects of the additional exercise effects of WBV and HIA because there were no significant differences in the percent change compared with the control group. Considering that the values of the 6-month intervention among the three groups are comparable, the variability in the absolute values at baseline might be likely to have the main effect on these results.
Moreover, the balance function has been reported to decline with age [21] as evidenced by increased postural sway and decreased stability. All subjects did not display positive and negative results because they were still young and had no physiological problems that would affect maintenance of their body balance regardless of their intervention.
The WBV and HIA groups did not experience effects on bone-related factors superior to those in the control group in the premenopausal women in this study. There may have been a couple of reasons for this nonresponse. First, the subjects had the good basic physical condition; the musculoskeletal tissues of premenopausal women have no special physiological necessity to fit the vibration and high-impact rope-jumping loading. Second, because most of the subjects in three groups had an occupation, even the subjects in the control group may have performed a higher number of activities to compensate for those of the additional stimulus in the WBV and HIA groups. Finally, the stimulus amount in WBV and HIA groups might have been insufficient to result in a difference from the control group. A couple of previous studies reported the effect of WBV on bone metabolism in young healthy adults. Torvinen et al. [17] supported our results with regard to BMD. They found no effect of WBV training on the mass, structure, or estimated strength of bone in young healthy adults. In their trial, the daily stimulus was only 4 minutes long three to five times per week for 8 months. In addition, in a 16-week study involving 51 healthy, active women, Humphries et al. [16] reported a significant within-group change in the BMD with WBV (femoral neck, 2.7%) and WBV plus resistance training (femoral neck, 1.9%; vertebra, 0.98%). Therefore, whether WBV might have positive effects on the body composition of young healthy women remains inconclusive.
With regard to HIA exercises in premenopausal women, a couple of recent papers [22-24] reported the effects of exercise on bone metabolism. Heinonen et al. [22] stated that an 18-month high-impact exercise intervention strengthened the femoral neck in premenopausal women by enhancing its structural properties. Liang et al. [23] concluded that a 12-month high-impact step aerobic exercise program resulted in a significant increase in the heel areal BMD in untrained young women aged 20 to 35 years who complied with the exercise regimen. A moderate-intensity strength-training intervention of similar duration had no effect on areal BMD, although leg strength increased significantly. Finally, Saraví et al. [24] reported significant associations between physical activity level and bone mass measures at all sites with the exception of the middle third of the radius in adult premenopausal women at three levels of physical activity. In our HIA trial, the duration of the daily stimulus (9 minutes three times per week for 6 months) seemed inadequate to improve the bone metabolism. Taking these studies into account, we may need a much longer period and higher impact level to obtain positive results using the ropejumping procedure.
WBV is new type of exercise that has been mainly reported in terms of its ability to increase bone mass [10-12], or fall-related neuromuscular parameters [6,10,12,13] and thus help to prevent bone fractures and osteoporosis in frail people. The effect of vibration on bone mass appears to be dependent upon the vibration characteristics (method of application, amplitude, and frequency) and exercise protocols (training type, intensity, and volume) employed [17,25]. Whether WBV plays an important role in a positive skeletal response for premenopausal women remains controversial [15-17]. There might be a possibility that a positive skeletal response to WBV is consistently observed only in older individuals, as previously reported [2-14].
Finally, the prevalence of osteopenia and osteoporosis is reportedly 15% and 0.6%, respectively, in premenopausal women [26]. In addition, it has been estimated that the loss of BMD ranges from 0.25% to 1% per year in premenopausal women [1]. Therefore, maintaining optimal BMD levels and body balance during the premenopausal years is important to reduce the risk of osteoporosis, falling down, and subsequent fractures during the postmenopausal years. Further studies might be needed that indicate the optimal stimulus amount in WBV and HIA procedures and the optimal timing (when to start) to maintain BMD for preparation for postmenopausal age, although the current study did not demonstrate it probably because of an insufficient stimulus and much younger age than the age at the beginning of the negative perimenopausal changes. Our results propose that higher exposure to isolated WBV than in the current study or WBV combined with HIA training might be needed to improve the bone metabolism of premenopausal women.
In conclusion, our data suggest that the 6 months of supervised WBV training and HIA exercises in our protocol might not effectively improve the bone metabolism or body balance in premenopausal women. Improvement in BMD after aerobic exercise reportedly depends on the degree of intensity strength training [23]. In addition, the vibration stimulus can be varied in multiple ways (including type, magnitude, frequency, and duration) with different effects on bone mass [17,25]. A proper quality and quantity of stimulus for premenopausal women should be established in the application of WVB and HIA for the prevention of osteoporosis, falling down, and subsequent fractures during the postmenopausal years.