Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Editorial - (2013) Volume 1, Issue 2
The strategy for increasing bone mineral density (BMD) has not been established in young men with low BMD. We report on a case of a young man with low BMD who was treated with exercise and nutritional management. A 29-year of old man consulted our clinic because of low BMD. He was instructed to perform maximum jumping exercise (5 times per day, 5 days per week) and intake calcium (800 mg/day), vitamin D (800 IU or 20 μg/day), and vitamin K (300 μg/day) for 6 months. The lumbar spine and femoral neck BMD increased by 2.9% and 4.7%, respectively. These results suggest the effectiveness of maximum jumping exercise and nutritional management (calcium, vitamin D, and vitamin K) on the BMD of the clinically relevant skeletal sites in young men with low BMD.
<Keywords: Jumping exercise; Nutrition; Femoral neck; Lumbar spine; Bone Mineral Density (BMD); Bone turnover marker
The lifetime risk for osteoporotic fractures is reported to be 40- 50% for females and 12-22% for males [1], which indicates that the incidence of osteoporotic fractures is lower in men than in women. The Dubbo Osteoporosis Epidemiology Study of community-dwelling women and men aged ≥ 60 years clarified the long-term mortality risk in women and men following osteoporotic fractures [2]; age-adjusted standardized mortality ratios were increased following hip fractures (2.43 and 3.51), vertebral fractures (1.82 and 2.12), and major fractures (1.65 and 1.70) for both women and men, respectively. Although lowtrauma fractures were associated with the increased mortality risk in both men and women, mortality after fractures was higher in men than in women.
The lifestyle including physical activity and nutritional management through all life plays an important role in the maintenance of bone health [3]. The strategies for preventing osteoporosis and its related fractures by physical activity in males are: i) maximizing peak bone mass in children and adolescents, ii) preventing age-related bone loss after 50 years of age, and iii) preventing falls and hip fractures in older men. Calcium, vitamin D, and vitamin K nutritional status needs to be improved. The purpose of exercise is different across ages. Maximizing peak bone mass in the most important in preventing osteoporotic fractures in later life. However, young males are less paid attention to than young females and older men from the view point of osteoporosis. The strategy for increasing bone mineral density (BMD) has not been established in young men with low BMD. We report on a case of a young man with low BMD who was treated with exercise and nutritional management.
After a medical check-up, a 29-year of old man consulted our sports medicine clinic because of low BMD. His height was 172 cm, body weight was 62 kg, and body mass index was 21.0 kg/m2. He had past histories of asthma, fibula fracture, and surgery for syndactyly. He was not a cigarette smoker, and had never drunk any alcohol beverages. He did not have a maternal history of hip fracture. The radiographs of the thoracic and lumbar spine did not show any vertebral fractures. The BMD of the lumbar spine and femoral neck were 0.992 g/cm2 and 0.764 g/cm2, respectively as measured using a dual-energy X-ray absorptiometry with a Prodigy Advance (GE Healthcare, Madison, USA), which corresponding to 84% and 80% of the young adult mean (YAM).
Blood and urine samples were obtained in the morning and were analyzed to assess biochemical markers; serum calcium, phosphorus, alkaline phosphatase (ALP), bone-specific ALP (BAP), undercarboxylated osteocalcin (ucOC), intact parathyroid hormone (iPTH), and urinary cross-linked N-terminal telopeptides of type I collagen (NTX). In particular, the serum levels of BAP, ucOC, and iPTH were measured by chemiluminescent enzyme immunoassay (CLEIA), electrochemiluminescent immunoassay (ECLIA), and ECLIA, respectively and the urinary level of NTX was measured by enzyme immunoassay (EIA). Although the serum level of ucOC was higher than the normal range, the serum or urinary levels of other biochemical markers were all within the normal ranges (Table 1).
The patient was instructed to perform maximum jumping exercise (5 times per day, 5 days per week) and intake calcium (800 mg/day), vitamin D (800 IU or 20 μg/day), and vitamin K (300 μg/day) based on the recommended daily intake of calcium, vitamin D, and vitamin K [4]. Exercise and nutritional intakes were continued for 6 months, and the effect of this intervention was evaluated by measuring the BMD and biochemical markers. The patients complied with this intervention. The lumbar spine and femoral neck BMD increased by 2.9% and 4.7%, respectively (Figure 1). The serum levels of ALP, BAP, ucOC, and iPTH decreased (Table 1). No adverse events were observed.
| Baseline | 6 months | Normal ranges | |
|---|---|---|---|
| Serum | |||
| Calcium (mg/dL) | 9.9 | 9.6 | 8.5 – 10.2 |
| Phosphorus (mg/dL) | 4.1 | 3.1 | 2.8 – 4.6 |
| ALP (IU/L) | 292 | 234 | 100 – 320 |
| BAP (µg/L) | 17 | 9.9 | 3.7 – 20.9 |
| ucOC (ng/mL) | 7.95 | 3.16 | <5.5 |
| iPTH (pg/mL) | 24 | 17 | 9 – 80 |
| Urine | |||
| NTX (nmol BCE/mmol Cr) | 41.6 | 35.2 | 9.3 – 54.3 |
ALP: Alkaline Phosphatase, BAP: Bone-specific Alkaline Phosphatase, Ucoc: Undercarboxylated Osteocalcin, Ipth: Intact Parathyroid Hormone, NTX: Crosslinked N-terminal Telopeptides of Type I Collagen, BCE: Bone Collagen Equivalent, Cr: Creatinine.
Table 1: Changes in biochemical markers during the 6-month of intervention period.
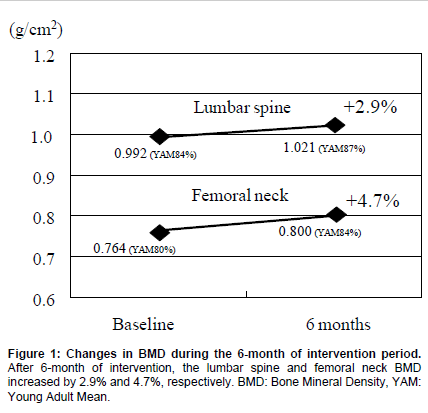
Figure 1:Changes in BMD during the 6-month of intervention period. After 6-month of intervention, the lumbar spine and femoral neck BMD increased by 2.9% and 4.7%, respectively. BMD: Bone Mineral Density, YAM: Young Adult Mean.
Exercise and nutritional management play an important role in increasing peak bone mass in children and adolescents [3]. The present report showed that maximum jumping exercise and nutritional management (calcium, vitamin D, and vitamin K) increased the lumbar spine and femoral neck BMD by 2.9% and 4.7%, respectively and decreased the serum levels of BAP, ucOC, and iPTH in a young man with low BMD. Peak bone mass is reached by age 30 years and bone mass remains stable until 50 years of age when the age-related bone loss starts in men. The results of the present report suggest the effectiveness of maximum jumping exercise and nutritional management on the BMD of the clinically relevant skeletal sites in young men with low BMD.
Increased mechanical usage stimulates bone modeling, suppresses bone remodeling, and increases bone strength [5,6]. The higher peak bone strain loaded is, the greater gains in bone mass and strength [5,6]. Because peak bone strain is important to control bone modeling and remodeling, high-impact mechanical loading appears to be effective to increase bone mass and strength. Experimental studies using turkeys and roosters demonstrates regulation of bone mass by mechanical strain; higher strain magnitude is beneficial in increasing bone mass, but lower cycle number with physiological strain magnitude is enough to obtain a significant increase in bone mass [7,8]. Another experimental study using young growing rats demonstrates that five jumps per day are enough to increase bone mass and strength [9]. These results suggest high-impact exercise like maximum jumping is effective in strengthening bone, but low-repetition is enough to obtain the significant effect of exercise.
A randomized controlled trial (RCT) in young women (mean age: 20.7 years) showed that low-repetition and high-impact exercise (10 maximum vertical jumps per day, 3 days per week) for 6 months was effective for improving the lumbar spine BMD (+2.64% in the training group vs. -1.12% in the control group) and femoral neck BMD (+2.42% in the training group vs. +0.60% in the control group) [10]. These results suggest that low-repetition and high-impact jumping may enhance the BMD at the clinically relevant skeletal sites in young women. However, a meta-analysis study demonstrated that brief (<30 min per day, 4.6 days per week) high-impact exercise improves the BMD at the femoral neck, but not at the lumbar spine in premenopausal women [11]. Another meta-analysis study demonstrated that impact activity with high-magnitude exercise (average dose: 1 hr per day, 3 days per week) increased the femoral neck and lumbar spine BMD in premenopausal women [12], suggesting the effect of the combined program with impact activity and resistance training on clinically relevant skeletal sites [3].
However, the effect of high-impact exercise on the BMD remains to be established in young men with low BMD. The present case report showed that maximum jumping exercise increased the lumbar spine and femoral neck BMD by 2.9% and 4.7%, respectively under nutritional management. Nutritional management (calcium, vitamin D, and vitamin K) might have stabilized the effectiveness of jumping exercise on the BMD. The magnitude of the BMD increase was greater at the femoral neck than at the lumbar spine, which supports the results of above meta-analysis studies. Muscle strengthening exercise of the back muscle might have been needed to enhance the BMD increase at the lumbar spine.
In the present case, the serum levels of BAP, ucOC, and iPTH were decreased (BAP: from 17.0 to 9.9 μg/L, ucOC: from 7.95 to 3.16 ng/mL, and iPTH from 24 to 17 pg/mL). The decrease in the urinary level of NTX was modest (from 41.6 to 35.2 nmol BCE/mmol Cr). The influence of jumping exercise on biochemical markers remains uncertain. However, the decrease in the serum levels of BAP and iPTH may partly be explained by the increased intake of vitamin D [13,14]. The increased intake of vitamin D through activate form of vitamin D3 or vitamin D supplementation is known to decrease serum levels of BAP and iPTH [13,14]. The decrease in serum ucOC level may partly be attributable to the increase intake of vitamin K. The high serum level of ucOC is associated with vitamin K deficiency (>5.5 ng/mL), and vitamin K2 administration is known to decrease the serum level of ucOC [15].
The limitation of the present report should be discussed. Nutritional assessment using a questionnaire before the intervention was lacking. The high serum level of ucOC (>5.5 ng/mL) suggested the existence of vitamin K deficiency. Vitamin K nutritional management was useful to reduce the serum level of ucOC. However, vitamin D status remains uncertain, because we did not evaluate vitamin D insufficiency/ deficiency by measuring the serum level of 25-hydroxyvitamin D. In Japan, the measurement of serum level of 25-hydroxyvitamin D is not covered by health insurance. However, the serum level of iPTH decreased after vitamin D nutritional management, possibly suggests the existence of vitamin D insufficiency. Further studies are needed to clarify the effect of nutritional management on the serum level of 25-hydroxyvitamin D.
A young man with low BMD was instructed to perform maximum jumping exercise (5 times per day, 5 days per week) and intake calcium (800 mg/day), vitamin D (800 IU or 20 μg/day), and vitamin K (300 μg/ day) for 6 months. The lumbar spine and femoral neck BMD increased by 2.9% and 4.7%, respectively. These results suggest the effectiveness of maximum jumping exercise and nutritional management (calcium, vitamin D, and vitamin K) on the BMD of the clinically relevant skeletal sites in young men with low BMD. It would be of interest to conduct RCTs to verify the results of this case report.
I received no funding from any pharmaceutical company, and have no conflict of interest, with regard to this paper.