Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 1
Effect of body position on electromyographic (EMG) activity has been studied in the cranio-cervical-mandibular muscles, but its effect on the activity of respiratory muscles in subjects with different breathing types has not yet been elucidated. This study included two groups of twenty male subjects each, one with upper costal and the other with costo-diaphragmatic breathing type. EMG activity was recorded using bipolar surface electrode technique. Electrodes were placed on the sternocleidomastoid (SCM), diaphragm (DIA), and external intercostal (EIC) and Latissimus dorsi (LAT) muscles. EMG activity was recorded in standing and lateral decubitus positions, during the following tasks: [1] Normal quiet breathing; [2] speaking the word “Mississippi”; [3] forced deep breathing. EMG activity of DIA and EIC muscles was higher in the standing than in the lateral decubitus position during all tasks in both breathing groups (p<0.05), excepting DIA activity during task 2 in the costo-diaphragmatic group. EMG activity of LAT muscle was higher in the standing than in the lateral decubitus position during task 3 in both breathing groups (p<0.05). EMG activity of DIA activity was higher in subjects with upper costal than in subjects with costo-diaphragmatic breathing type in the standing position during all tasks and also in the lateral decubitus position during tasks 1 and 2 (p<0.05). EMG activity of ECM, EIC and LAT muscles was not significantly different between both breathing types in the studied body positions. The higher EMG activity observed in the standing than in the lateral decubitus positions in both breathing groups, suggests differences in the respiratory effort depending on the body position. The higher EMG activity observed in DIA muscle of subjects with upper costal than costo-diaphragmatic breathing types, suggests differences in the respiratory effort depending on the breathing type.
Keywords: Electromyographic activity; Standing position; Lateral decubitus position; Upper costal breathing; Costo-diaphragmatic breathing
The acquisition and processing of oxygen is the primary task of any air-breathing vertebrate. Chewing, walking, reproducing and thinking are all fine, but first one must breathe [1]. There is no higher priority for the body than to breathe [2]. Respiratory muscle contraction is a continual process that ventilates the alveoli and it is usually under automatic control by respiratory centres in the ponto-medullary region of the brainstem [3].
Several breathing types have been defined depending on the expansion of the abdomino-thoracic region during inspiration at rest [4-6]: i) Costo-diaphragmatic breathing, ii) Upper costal breathing, and iii) Mixed breathing.
Obligatory muscles of respiration, e.g. diaphragm (DIA), scalene, parasternal and external intercostal (EIC) muscles, contract in every breath cycle during quiet breathing. Additional accessory respiratory muscles, e.g. sternocleidomastoid (SCM) and trapezius muscles, contract when the demand in the respiratory system changes, such as forced deep breathing [7-9].
In addition, the latissimus dorsi (LAT) muscle appears to have an inspiratory action in patients experiencing respiratory difficulty, e.g., hyperpnea, emphysema, and asthma [10,11], and with increased inspiratory load [12]. Electromyographic (EMG) activity of SCM, DIA, EIC and LAT muscles have been compared between subjects with costo-diaphragmatic or upper costal breathing in the standing position.
Higher EMG activity of DIA and EIC muscles was observed during different tasks in the upper costal group, whereas EMG activity of SCM and LAT was similar between both groups [13,14]. To the best of our knownledge no study has compared EMG activity of respiratory muscles, in the lateral decubitus position, between subjects with different breathing types. It is unknown if subjects with upper costal breathing also present higher EMG activity than subjects with costodiaphragmatic breathing, in the lateral decubitus position.
Therefore, the aim of the present work is to compare EMG activity of respiratory muscles between subjects with upper costal or costodiaphragmatic breathing types in the standing and in the lateral decubitus positions.
Ethical approval
All experimental procedures were conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983 and approved by The Ethics Committee of the Faculty of Dentistry, University of Chile. Written informed consents were obtained from all participant subjects.
Subjects
This study included two groups of 20 male subjects each, one with upper costal and the other with costo-diaphragmatic breathing. The breathing type of the subjects was determined by two authors (RM and RC) and the agreement of both examiners was needed for subject classification. Consistency in the clinical diagnosis across the examiners was high, and when there was no agreement, the subject was not included.
Each subject was asked to remain standing, looking straight ahead, with their feet 10 cm apart, and to breathe normally for 2 minutes as a baseline. First, the examiners placed the left hand on the upper chest and the right hand on the upper back; next, they placed the left hand on the upper abdomen and the right hand on the lower left costal region.
After checking 10 inspirations on each step of the clinical examination, the subject was classified to be of the upper costal breathing type if, during inspiration at rest, the superior thoracic expansion was predominant, and the costo-diaphragmatic breathing type when the abdominal and lateral costal expansion was predominant [13,14].
Those subjects who did not show a clear predominance of superior thoracic expansion or abdominal and lateral costal expansion (mixed breathing type), were excluded from the study. The participants were students enrolled at the Dental or Medical School of the University of Chile, to complete 40 subjects who met the inclusion criteria mentioned below.
All subjets selected had complete natural dentition (excluding the third molars), no history of orofacial pain or craniomandibularcervical disorders, no heart or respiratory disease. Subjects recruited were only male to avoid difficulties with breast size, asymmetry of breasts and the use of a bra related to female subjects during EMG recording. None of the subjects was on medication that could have influenced muscle activity.
Electromyography
Bipolar surface electrodes (BioFLEX, BioResearch Associates, Inc., Brown Deer, WI, and USA) were placed on the SCM, DIA, EIC and LAT muscles. Impedance was decreased by careful skin shaving and abrasion with alcohol.
The electrodes were placed as follows [13,14]: on SCM muscle (middle portion), in the anterior border 1 cm above and below the motor point; on DIA muscle, 1 cm below the xiphoid process; on EIC muscle, between the 6th and 7th ribs on the imaginary vertical line that passes through the nipple; and on LAT muscle, in the projection of the 12th rib or lumbar vertebra L1 following the thoracolumbar fascia edge.
The electrodes were unilaterally placed on the left side, because for EMG recording in the lateral decubitus position, all subjects were asked arbitrarily to lay on his right side. Surface ground electrode was attached to the forehead. EMG activity was recorded using a 4-channel computerized instrument in which the signals were amplified (Model 7P5B preamplifier, Grass Instrument Co., Quincy, MA, USA) and filtered (10 Hz high pass and 2 kHz low pass), with a common mode rejection ratio higher than 100 dB.
The output was filtered again (notch frequency of 50 Hz), full-wave rectified and then integrated (time constant of 0.1 s), and recorded online on a computer exclusively dedicated to acquisition and processing of EMG signals. EMG signal was acquired at a sample rate of 200 Hz (50 Hz each channel) with a 12 bits A/D converter (MAX191) connected to the computer through an RS-232 port. The system was calibrated before each record.
EMG activity was recorded in the following body positions:
Standing position; maintaining a stance with the feet 10 cm apart, eyes open, looking straight ahead. The self-balanced position was obtained by having each subject stand with his visual axis on the horizontal, with no external intervention or modification of his posture [13,14].
Right lateral decubitus position; head, neck and body horizontally aligned, checked by an external operator located approximately 3 m from the bed [5]. The head and neck of each subject were supported by a Sleep Easy Pillow (Interwood Marketing Groups, Ontario, Canada).
The subject placed his hands in front of the chest and slightly flexed his legs. A mattress (Rosen Runnair Physio-Actions, Temuco, Chile) was used. Lateral decubitus position was chosen because it is an habitual sleeping position and also it is possible to stay several hours a day in that position. At lateral decubitus position, room light was turn off and the subjects kept his eyes closed.
Each subject underwent three unilateral EMG recordings of left SCM, DIA, EIC and LAT muscles under the following experimental conditions:
Task 1: normal quiet breathing
Task 2: speaking the word “Mississippi”
Task 3: forced deep breathing
Before EMG recording, an examiner explained all tasks to each subject, in order he would be able to perform each one correctly. The order of the tasks was randomized. During task 1 the subject had his jaw in the resting posture.
During task 2 the subject pronounced the word “Mississippi”. This phonetic method was chosen for being a functional activity commonly used by dentists in most oral reconstructive procedures [15]. During task 3, each subject was asked to breathe in total lung capacity, holding the breath for 10s.
This period was selected to ensure maximum and sustained muscle activity without producing a respiratory function disorder. Tasks 1 and 2 also lasted 10 seconds based on the duration of task 3. A 20 s resting period was allowed between each EMG recording in each task.
To obtain the average value of each curve, measurements were taken every 0.1 s from the beginning to the end of the recording, using a computer program. The mean value of the three curves obtained at each task and for each subject was used. Variability of EMG data during the tasks was assessed by the coefficient of variability.
The values obtained were 38.5% in the SCM muscle, 11.8% in the DIA muscle, 11.6% in the EIC muscle, and 20.1% in the LAT muscle. Body mass index (BMI) was obtained for each subject by dividing the weight (kg) by the square of the height (m2). Age and BMI were used to check for possible influence on EMG activity recorded in each muscle (Table 1).
| Subjects | Costo-diaphragmatic breathing type | Upper costal breathing type | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Weight (Kg) | Height (m) | BMI | Subjects | Age | Weight (Kg) | Height (m) | BMI | |
| 1 | 21 | 76 | 1.75 | 24.82 | 1 | 25 | 60 | 1.74 | 19.82 |
| 2 | 22 | 80 | 1.76 | 25.83 | 2 | 24 | 76 | 1.81 | 23.20 |
| 3 | 21 | 68 | 1.7 | 23.53 | 3 | 24 | 73 | 1.77 | 23.30 |
| 4 | 24 | 67 | 1.8 | 20.68 | 4 | 19 | 65 | 1.66 | 23.59 |
| 5 | 24 | 64 | 1.76 | 20.66 | 5 | 20 | 73 | 1.76 | 23.57 |
| 6 | 22 | 70 | 1.7 | 24.22 | 6 | 19 | 71 | 1.73 | 23.72 |
| 7 | 23 | 73 | 1.67 | 26.18 | 7 | 20 | 94 | 1.8 | 29.01 |
| 8 | 24 | 69 | 1.7 | 23.88 | 8 | 18 | 90 | 1.81 | 27.47 |
| 9 | 23 | 72 | 1.79 | 22.47 | 9 | 19 | 70 | 1.75 | 22.86 |
| 10 | 26 | 74 | 1.8 | 22.84 | 10 | 19 | 70 | 1.64 | 26.03 |
| 11 | 25 | 85 | 1.75 | 27.76 | 11 | 18 | 58 | 1.64 | 21.56 |
| 12 | 19 | 64 | 1.74 | 21.14 | 12 | 18 | 69 | 1.73 | 23.05 |
| 13 | 22 | 78 | 1.75 | 25.47 | 13 | 19 | 65 | 1.75 | 21.22 |
| 14 | 19 | 60 | 1.68 | 21.26 | 14 | 19 | 70 | 1.71 | 23.94 |
| 15 | 19 | 68 | 1.73 | 22.72 | 15 | 20 | 69 | 1.73 | 23.05 |
| 16 | 18 | 100 | 1.8 | 30.86 | 16 | 22 | 63 | 1.76 | 20.34 |
| 17 | 20 | 69 | 1.71 | 23.60 | 17 | 19 | 55 | 1.68 | 19.49 |
| 18 | 18 | 82 | 1.76 | 26.47 | 18 | 21 | 75 | 1.86 | 21.68 |
| 19 | 20 | 80 | 1.83 | 23.89 | 19 | 22 | 90 | 1.7 | 31.14 |
| 20 | 21 | 64 | 1.75 | 20.90 | 20 | 22 | 70 | 1.68 | 24.80 |
| Mean | 21.6 | 73.2 | 1.7 | 24.0 | Mean | 20.4 | 71.3 | 1.7 | 23.6 |
| SD | 2.4 | 9.3 | 0.0 | 2.6 | SD | 2.1 | 10.2 | 0.1 | 2.9 |
Table 1: Characteristics of subjects studied.
Statistics
Data were analyzed using SYSTAT 13 program (Systat Software Inc. (SSI), San Jose, CA, USA).
EMG activity presented non-normal distribution (p<0.05; Shapiro- Wilk test); therefore, Wilcoxon rank-sum test for dependent samples was used to compare the activity of each muscle between body positions during tasks, and Mann-Whitney U-test was used to compare the activity of each muscle between both groups during tasks.
A value of p<0.05 was considered statistically significant. Age data presented a non-normal distribution (p<0.05; Shapiro-Wilk test); therefore Mann-Whitney U-test was used for the comparison between samples studied. BMI data presented a normal distribution (p>0.05; Shapiro-Wilk test); therefore t-test was used for the comparison between samples studied.
Mean age values ± (SD) of both groups were 20.4 ± (2.1) and 21.6 ± (2.4) for upper costal and costo-diaphragmatic breathing types, respectively. No significant difference was observed between both groups (p>0.05, Mann-Whitney U-test). Mean BMI values ± (SD) of both groups were 23.6 ± (2.9) and 24.0 ± (2.6) for upper costal and costo-diaphragmatic breathing types, respectively. No significant difference was observed between both groups (p>0.05, t-test for independent samples).
Figure 1 shows the effect of body position on EMG activity in both breathing groups in all muscles studied.
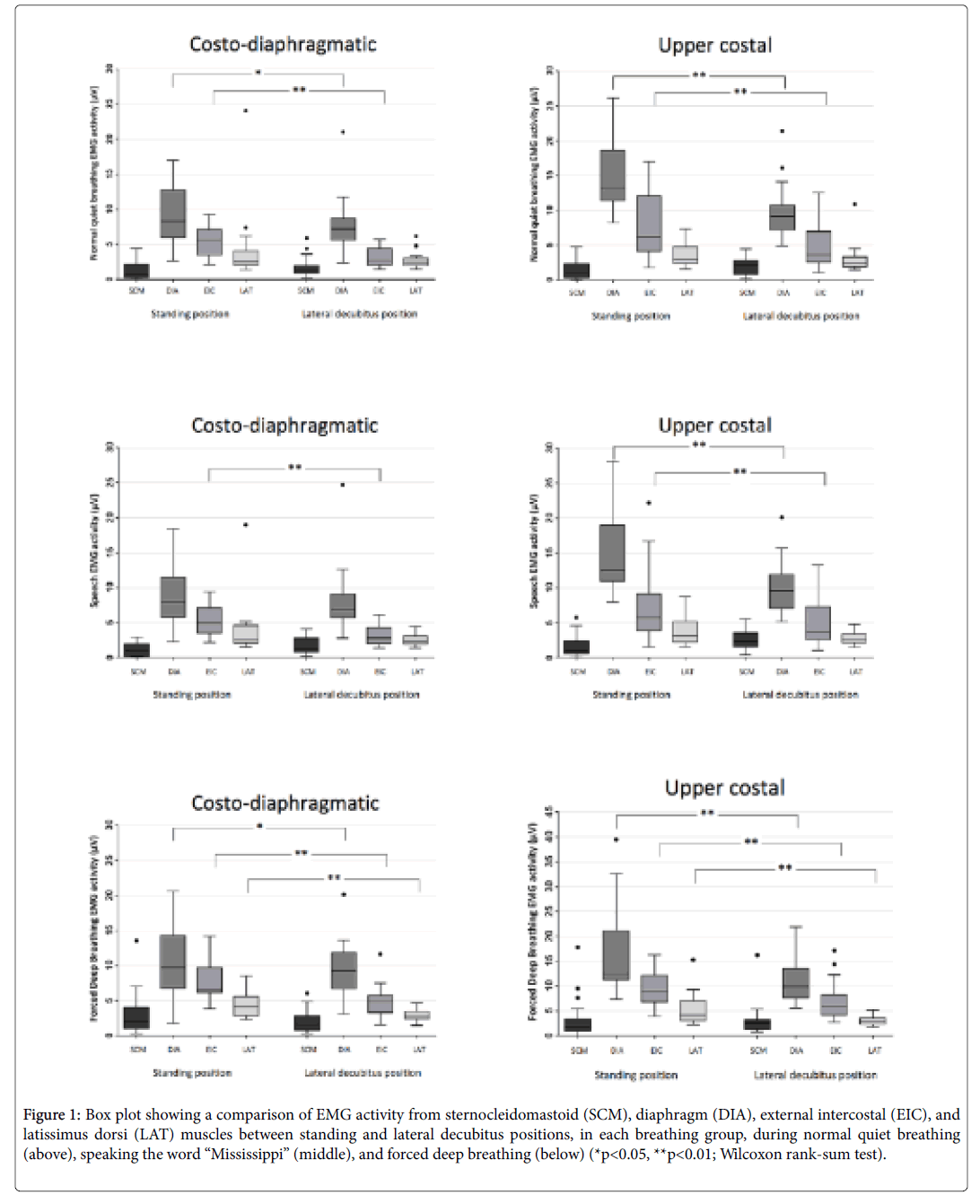
Figure 1: Box plot showing a comparison of EMG activity from sternocleidomastoid (SCM), diaphragm (DIA), external intercostal (EIC), and latissimus dorsi (LAT) muscles between standing and lateral decubitus positions, in each breathing group, during normal quiet breathing (above), speaking the word “Mississippi” (middle), and forced deep breathing (below) (*p<0.05, **p<0.01; Wilcoxon rank-sum test).
EMG activity of DIA and EIC muscles was significantly higher during standing than in the lateral decubitus position in both breathing groups during all tasks (*p<0.05), except activity of DIA muscle in subjects with costodiaphragmatic breathing during task 2 (speaking) (p>0.05).
EMG activity of SCM muscle was the lowest of all muscles studied and did not change with body position or breathing type (p>0.05).
EMG activity of LAT muscle was higher in the standing than in the lateral decubitus position in both breathing groups, only during task 3 (forced deep breathing) (*p<0.05).
Figures 2 and 3 show that EMG activity of DIA muscle was significantly higher during task 1 and 2, respectively, in subjects with upper costal than with costo-diaphragmatic breathing, in the standing position (**p<0.01; upper panel) and in the lateral decubitus position (*p<0.05; lower panel), whereas EMG activity of SCM, EIC and LAT muscles did not differ between both breathing types in the studied body positions (p>0.05).
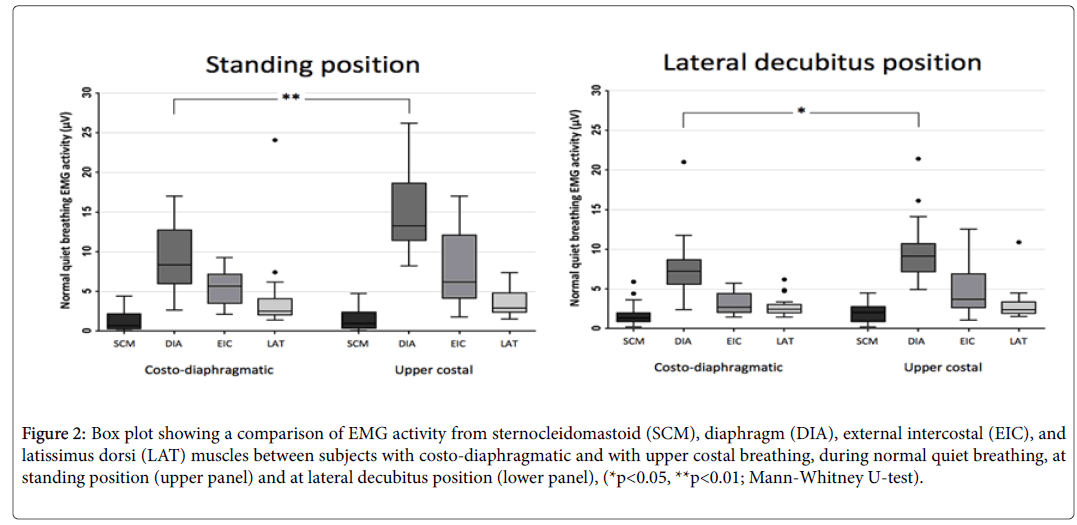
Figure 2: Box plot showing a comparison of EMG activity from sternocleidomastoid (SCM), diaphragm (DIA), external intercostal (EIC), and latissimus dorsi (LAT) muscles between subjects with costo-diaphragmatic and with upper costal breathing, during normal quiet breathing, at standing position (upper panel) and at lateral decubitus position (lower panel), (*p<0.05, **p<0.01; Mann-Whitney U-test).
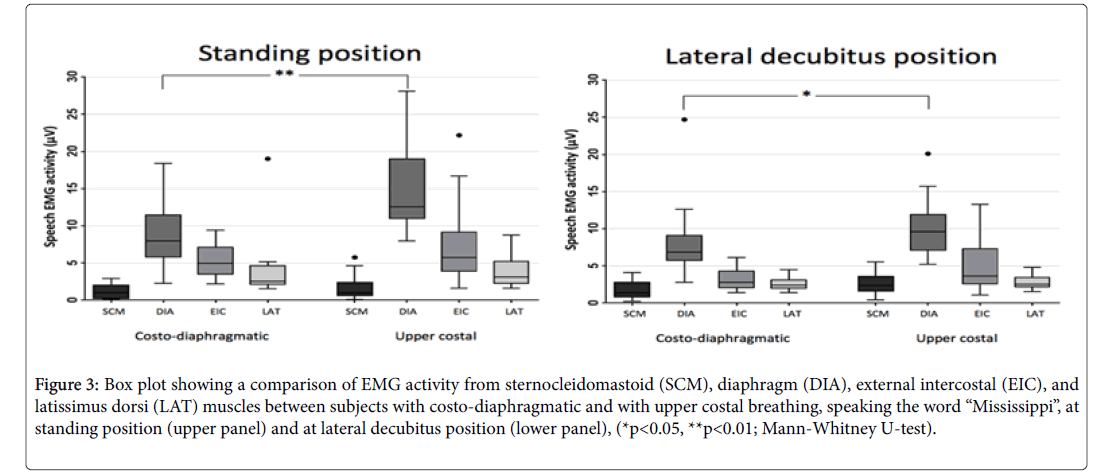
Figure 3: Box plot showing a comparison of EMG activity from sternocleidomastoid (SCM), diaphragm (DIA), external intercostal (EIC), and latissimus dorsi (LAT) muscles between subjects with costo-diaphragmatic and with upper costal breathing, speaking the word “Mississippi”, at standing position (upper panel) and at lateral decubitus position (lower panel), (*p<0.05, **p<0.01; Mann-Whitney U-test).
Figure 4 shows that EMG activity of DIA muscle in the standing position (upper panel) was significantly higher during tasks 3 (forced deep breathing) in subjects with upper costal than in subjects with costo-diaphragmatic breathing type (*p<0.05); whereas EMG activity of SCM, EIC and LAT muscles did not differ between both breathing groups (p>0.05). EMG activity of all muscles was similar during task 3 in the lateral decubitus position (lower panel) between both breathing types (p>0.05).
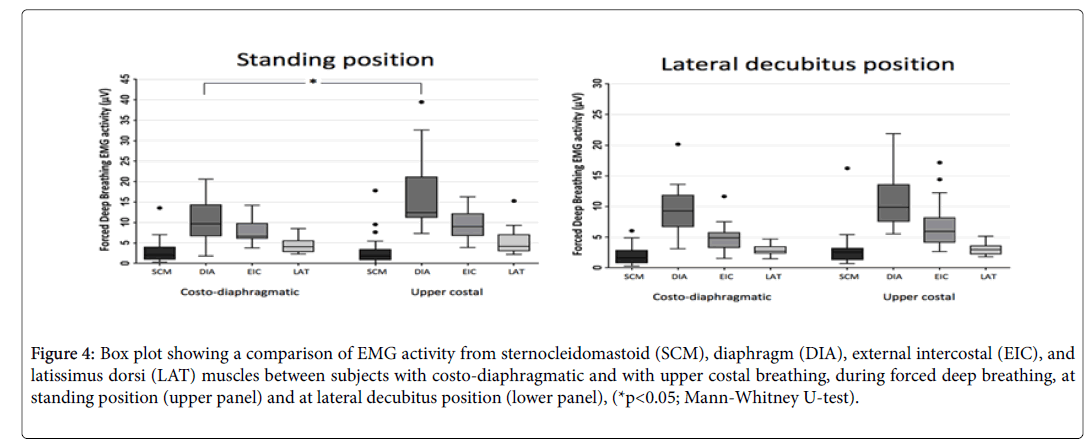
Figure 4: Box plot showing a comparison of EMG activity from sternocleidomastoid (SCM), diaphragm (DIA), external intercostal (EIC), and latissimus dorsi (LAT) muscles between subjects with costo-diaphragmatic and with upper costal breathing, during forced deep breathing, at standing position (upper panel) and at lateral decubitus position (lower panel), (*p<0.05; Mann-Whitney U-test).
In the present study, the subjects were asked to perform all tasks voluntarily, in accordance to previous instructions. This is important, since it is well known that premotor drive from multiple descending pathways, i.e., from the motor cortex for voluntary respiratory tasks, are integrated at the spinal cord [16,17]. They may arise directly from oligosynaptic pathways from the motor cortex to the diaphragm and intercostal motoneurons [18] or from local spinal reflexes. At the spinal level, all inputs acting on motoneurons and interneurons, including spinal reflexes, are coordinated to produce the appropriate motor output [17].
The significantly higher EMG activity observed during standing than in the lateral decubitus position is important because it suggests differences in the respiratory effort depending on the body position. This finding can be explained by the fact that, in the standing position, intrapleural pressure is lower at the apex than in the base of the lungs [19]. This results in more expanded alveoli in the apex than the base, leading to lower alveolar ventilation in the apex, which is independent of the breathing type. In the right lateral decubitus position, the intrapleural pressure gradient goes from the left to the right lung, therefore, alveolar ventilation is higher in the right than in the left lung. Since the right lung is bigger than the left, respiratory effort is lower in the right lateral decubitus than in the standing position, thus explaining the lower EMG activity recorded in the former position.
The higher activity recorded in the standing position may also be due to a differential modulation of the motor neuron pools of respiratory muscles arising from different types of receptors, such as: plantar mechano-receptors, leg muscular proprioceptors, knee articular proprioceptors, vestibular and visual receptors. It is reasonable to assume that afferences stemming from these receptors are different in the standing than in the lateral decubitus positions. In addition, in our work, it is very important to consider the change in visual inputs, since in the standing position the subjects kept his eyes open and looked straight ahead, while in the lateral decubitus position, room light was turned off and the subjects kept his eyes closed.
The significantly higher EMG activity observed in DIA muscle of subjects with upper costal breathing, during standing at all tasks (Figures 2-4, upper panels), agrees with the result observed in previous works [13,14]. The higher activity of DIA muscle is contrary to that expected, since in the presence of a predominant superior thoracic expansion, a lower EMG activity would be expected in this muscle. Subjects that preferentially expand the superior part of the thorax (upper costal breathing), however, require higher respiratory effort to produce a normal alveolar ventilation, since, as mentioned above, respiratory effort is higher in the standing than in the right lateral decubitus position. Therefore, the higher EMG activity recorded in DIA muscle would result from the higher respiratory effort, depending on the breathing type which could reduce the adaptive capability of these subjects.
The higher EMG activity observed in DIA muscle of subjects with upper costal breathing in the right lateral decubitus position during tasks 1 and 2 (Figures 2 and 3, lower panels) is important because normal quiet breathing is frequent while resting in a bed and is also an habitual sleeping position and to speak is frequent during awake hours, respectively.
This higher EMG activity recorded in DIA muscle of subjects with upper costal breathing in the right lateral decubitus position, however, cannot be attributed to a higher respiratory effort, since alveoli expansion in the apex and in the base of the lung are similar in both breathing types. We do not know if subjects with upper costal breathing (diagnosed in the standing position) maintain their breathing type in the lateral decubitus position, therefore, in a future study this should be assessed.
Similar EMG activity of SCM muscles in the standing position, in both breathing groups, is in agreement with previous studies [5,13,14]. This same EMG activity pattern was observed in the lateral decubitus position in the present study. This behavior of SCM muscle could be explained by a predominant effect of vestibular and/or visual afferents than other influences on its pool of motoneurons, depending on the body position, due to its role as postural rather than respiratory muscle.
Similar EMG activity of LAT muscle in both breathing groups, during all studied tasks in the standing position, agrees with previous studies [13,14]. This same EMG activity pattern was observed in the lateral decubitus position in the present study, suggesting that activity of this muscle is more relevant during longer disturbances and/or critical conditions [10,11].
The present study has at least four limitations. First, subjects studied were only male which limits the ability to extrapolate these findings to the general population. Second, we do not have data regarding the difference or similarity in the smoking habit in both groups. Third, we only studied young subjects and it is possible that elderly subjects with lung or cardiac disease could present differences in the EMG pattern. Fourth, surface electrodes on the chest could capture electrocardiogram and/or pick up activity from neighboring muscles. In addition, EMG activity recorded in the left EIC muscle during right lateral decubitus position could be more influenced by cardiac activity than right EIC activity recorded in the left lateral decubitus position. This could be important and deserves to be assessed in a future study. In spite of these limitations, this is the first study that shows significant higher diaphragm EMG activity in the lateral decubitus position, in young adult subjects with upper costal breathing than in subjects with costo-diaphragmatic breathing during low effort (normal quiet breathing and speech).
• Higher EMG activity in the diaphragm and external intercostal muscles observed in both breathing types in the standing than in the lateral decubitus position, suggests differences in the respiratory effort depending on the body position.
• Higher EMG activity in the diaphragm observed in subjects with upper costal than in subjects with costo-diaphragmatic breathing, during normal quiet breathing and speaking the word “Mississippi”, suggests a higher respiratory effort depending on the breathing type that could reduce their adaptive capability.