Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2015) Volume 3, Issue 3
We have used a series of economic models to evaluate the differences in medical costs associated with the use of each of the four targeted-specific oral anticoagulants (TSOACs), dabigatran, rivaroxaban, apixaban, and edoxaban vs. warfarin for the treatment of nonvalvular atrial fibrillation (NVAF) and venous thromboembolism (VTE). All economic models were based on clinical event rates reported in published randomized phase III clinical trials, except one model used real-world data among patients with VTE. Incremental annual medical costs among NVAF and VTE patients with clinical events from a U.S. payer perspective were obtained from the literature and inflation adjusted to 2013 cost levels. The economic model for NVAF patients estimated that in a year the total medical cost differences associated with TSOAC use relative to warfarin at $204, $140, $495, and -$340 per patient for dabigatran, rivaroxaban, apixaban, and edoxaban, respectively. The economic model for patients with acute symptomatic VTE estimated that in a year the total medical cost differences associated with TSOAC use relative to warfarin at -$146, -$482, -$918, and -$344 per patient for dabigatran, rivaroxaban, apixaban, and edoxaban, respectively. In all cases, univariate and multivariable sensitivity analyses were conducted to establish the robustness of the results of the economic models. Additionally, we extrapolated the results of our economic models to a combined population of NVAF patients and acute VTE patients among a hypothetical cohort of 1 million insured lives. Our economic evaluations have consistently shown that medical costs are reduced when TSOACs are used instead of warfarin for the treatment of NVAF or VTE, with apixaban being associated with the greatest reduction in medical costs. This review describes the execution of these economic evaluations and their results.
Keywords: Economic models; Healthcare costs; New oral anticoagulants; Nonvalvular atrial fibrillation; Venous thromboembolism
Nonvalvular atrial fibrillation (NVAF) is a common cardiac rhythm disorder that is associated with up to a 5-fold increase in stroke risk [1,2]. Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is the third most common cause of vascular disease-related death [3]. NVAF and VTE affect several million people in the U.S. and are associated with significant morbidity and substantial healthcare resource utilization and costs [1-10]. It was estimated in 2008 that the annual direct medical cost of NVAF was $6 billion for NVAF-related costs only and $26 billion when including other concomitant cardiovascular and noncardiovascular costs [9]. VTE was estimated in 2011 to cost between $13.5 and $27.2 billion annually in the U.S. [3,10].
To reduce stroke risk of patients with NVAF warfarin therapy has been used for decades [11]; however, warfarin has several disadvantages in that it has a slow onset of action, narrow therapeutic range, interacts with food and other medications, and its use requires frequent monitoring and dose adjustments [11,12]. Because of these reasons and others, such as increased bleeding risk, there is reluctance to prescribe warfarin therapy to many NVAF patients and for patients to remain adherent to therapy [12,13]. Warfarin therapy, succeeding low molecular weight heparin (LMWH), is also commonly used among VTE patients, who experience similar disadvantages as NVAF patients on warfarin therapy [14]. The suboptimal use of warfarin therapy among NVAF and VTE patients can lead to poor patient outcomes and higher healthcare costs, which may potentially be prevented with better alternative therapies [12,13,15-17].
Recently, the targeted-specific oral anticoagulants (TSOACs), dabigatran, rivaroxaban, apixaban, and edoxaban have been approved by the FDA for treatment of NVAF and VTE. All of the TSOACs have been shown to be efficacious for the treatment of NVAF and VTE in randomized phase III clinical trials [18-28]. In addition to being efficacious for the treatment of NVAF and VTE, TSOACs offer pharmacologic advantages over other anticoagulation therapies in that they are orally administered, have a rapid onset of action, few drug-drug or drug-food interactions, and predictable pharmacokinetics, thereby eliminating the need for regular monitoring [15,29]. In the TSOAC vs. warfarin clinical trials clinical event rates, including stroke and systemic embolism, recurrent VTE, and bleeding, differed among NVAF and VTE patients treated with the different TSOACs vs. warfarin [18-28]. As clinical event rates differed among NVAF and VTE patients treated with the different TSOACs vs. warfarin it is important to determine which of the TSOACs may provide the best clinical and economic benefits so that healthcare providers, healthcare policy makers, and payers have the information for decision-making processes. Therefore, we have undertaken several studies in an effort to demonstrate the potential savings in medical costs associated with use of each of the TSOACs vs. warfarin for the treatment of NVAF and VTE [30-36]. We have estimated that when any of the four TSOACs are used instead of warfarin medical costs are reduced for patients with NVAF and VTE, with apixaban being associated with the greatest reductions in medical costs for both patient groups [30,33,35]. This review describes the execution of these economic evaluations and their results.
We previously developed several Excel based models to estimate the differences in medical costs among NVAF and VTE patients treated with each of the four TSOACs vs. warfarin [30-36] (Table 1). These models included inputs of clinical event rates obtained from published clinical trial data and annual costs of clinical events from a U.S. payer perspective obtained from published literature. The economic evaluations included one-way and multivariable sensitivity analyses for each of the TSOAC vs. warfarin comparisons.
| Study Title | Indication | Patient Population | TSOACs Evaluated |
| Medical cost reductions associated with the usage of TSOACs vs. warfarin among atrial fibrillation patients, based on the RE-LY, ROCKET-AF, and ARISTOTLE trials [30] | NVAF | Overall NVAF population | Dabigatran, Rivaroxaban, Apixaban |
| Medical costs in the US of clinical events associated with TSOAC use compared to warfarin among non-valvular atrial fibrillation patients ≥75 and <75 years of age, based on the ARISTOTLE, RE-LY, and ROCKET-AF trials [31] | NVAF | Different age group NVAF populations | Dabigatran, Rivaroxaban, Apixaban |
| Medical costs of TSOACs vs. warfarin for atrial fibrillation patients with different stroke risks [32] | NVAF | Different stroke risk NVAF populations | Dabigatran, Rivaroxaban, Apixaban |
| Estimation of the impact of warfarin's time-in-therapeutic range on stroke and major bleeding rates and its influence on the medical cost avoidance associated with TSOAC use-learnings from ARISTOTLE, ROCKET-AF, and RE-LY trials [34] | NVAF | Different warfarin time-in-therapeutic range NVAF populations | Dabigatran, Rivaroxaban, Apixaban |
| Comparison of differences in medical costs when TSOACs are used for the treatment of patients with nonvalvular atrial fibrillation and venous thromboembolism vs. warfarin or placebo in the U.S [35] | NVAF and VTE | Overall NVAF and acute VTE populations | Dabigatran, Rivaroxaban, Apixaban, Edoxaban |
| Evaluation of medical costs associated with use of TSOACs compared with standard therapy among venous thromboembolism patients [33] | VTE | Acute VTE population | Dabigatran, Rivaroxaban, Apixaban, Edoxaban |
| Evaluation of medical costs avoided when TSOACs are used for extended treatment of venous thromboembolism based on clinical trial results [36] | VTE | Extended treatment VTE population | Dabigatran, Rivaroxaban, Apixaban |
| Real-world medical cost avoidance when TSOACs are used vs. warfarin for venous thromboembolism in the US [51] | VTE | Real-world VTE population | Dabigatran, Rivaroxaban, Apixaban, Edoxaban |
Table 1: Overview of Models Used to Evaluate Differences in Medical Costs Avoided Among Nonvalvular Atrial Fibrillation (NVAF) Patients and Venous Thromboembolism (VTE) Patients Treated with the Different Targeted-specific Oral Anticoagulants (TSOACs) vs. Warfarin [30-36].
Model inputs: Clinical event rates based on clinical trial data
For the economic model in which differences in medical costs were evaluated among NVAF patients treated with TSOACs vs. warfarin, the clinical events evaluated included ischemic or uncertain type of stroke, hemorrhagic stroke, systemic embolism, myocardial infarction (MI), pulmonary embolism (PE) or deep vein thrombosis (DVT), major bleedings excluding hemorrhagic stroke (MBEHS), clinically relevant non-major bleedings (CRNMB), and other minor bleeding events. The rates of clinical events among NVAF patients treated with warfarin and TSOACs were based on the published data obtained from each corresponding TSOAC vs. warfarin comparison clinical trial [18-21]. There were two edoxaban treatment arms in the ENGAGE-AF-TIMI trial, one of NVAF patients treated with 30 mg edoxaban once daily and the other of NVAF patients treated with 60 mg edoxaban once daily [21]. Since the 60 mg dose is the FDA recommended dose for the majority of NVAF patients (creatinine clearance (CrCL) >50 to ≤95 mL/min; not used in patients with CrCL>95 mL/min) only the edoxaban 60 mg dosing regimen arm clinical trial data were used [37].
Clinical event rates of ischemic stroke among NVAF patients were estimated at 0.91% vs. 1.20% for those treated with dabigatran vs. warfarin, 1.43% vs. 1.52% for those treated with rivaroxaban vs. warfarin, 0.97% vs. 1.05% for those treated with apixaban vs. warfarin, and 1.25% vs. 1.25% for those treated with edoxaban vs. warfarin. Clinical event rates of MBEHS among NVAF patients were estimated at 3.22% vs. 3.19% for those treated with dabigatran vs. warfarin, 3.28% vs. 2.96% for those treated with rivaroxaban vs. warfarin, 1.89% vs. 2.62% for those treated with apixaban vs. warfarin, and 2.49% vs. 3.43% for those treated with edoxaban vs. warfarin. Other evaluated clinical event rates among clinical trial NVAF patients are reported in Amin et al. [35].
For the economic model in which differences in medical costs were evaluated among VTE patients treated with TSOACs vs. warfarin, the clinical events evaluated included recurrent VTE/VTE-related death as defined in the clinical trials, major bleeding (MB), CRNMB, and other minor bleeding. Calculated as previously done for NVAF patients, clinical event rates of recurrent VTE among VTE patients were estimated at 2.35% vs. 2.15% for those treated with dabigatran vs. warfarin, 2.07% vs. 2.30% for those treated with rivaroxaban vs. warfarin, 2.26% vs. 2.69% for those treated with apixaban vs. warfarin, and 1.60% vs. 1.94% for those treated with edoxaban vs. warfarin. Clinical event rates of MB among VTE patients were estimated at 1.37% vs. 1.80% for those treated with dabigatran vs. warfarin, 0.97% vs. 1.75% for those treated with rivaroxaban vs. warfarin, 0.56% vs. 1.82% for those treated with apixaban vs. warfarin, and 1.36% vs. 1.60% for those treated with edoxaban vs. warfarin. Other evaluated clinical event rates among VTE clinical trial patients are reported in Amin et al. [33].
Model inputs: Incremental costs of clinical events
Incremental annual costs, defined as the incremental costs to a U.S. health payer of a NVAF patient experiencing ischemic stroke, hemorrhagic stroke, systemic embolism, MI, PE/DVT or MBEHS during one year following the initial event, were obtained from published literature [12,38,39]. The one-year costs of a NVAF patient with CRNMB or other minor bleeding events were based on the costs of office visits obtained from the Medicare Fee Schedule, Payment and Reimbursement Benefit Guideline [40]. Among VTE patients, the one-year cost of recurrent VTE was obtained from Lefebvre, et al. [41]. The one-year costs of MB and CRNMB for a patient with VTE were derived from a retrospective analysis of MarketScan database claims of patients with a diagnosis of VTE (1/1/2008-12/31/2011) [42]. Among VTE patients the one-year cost of a minor bleeding event was obtained as for NVAF patients [40]. The one-year medical costs associated with all of the evaluated clinical events were inflation adjusted to 2013 cost levels via the CPI Medical Care Index [43].
One-year medical costs of NVAF patients with clinical endpoints relative to patients who did not have a clinical event in 2013 dollars were estimated as the following: ischemic stroke=$43,890 [12], hemorrhagic stroke=$57,384 [12], systemic embolism=$21,945 [12], MI=$41,277 [38], PE/DVT=$19,532 [39], MBEHS=$38,454 [12], CRNMB (based on estimated four claims of CPT code 99215: level 5 established office patient visit)=$547 [40], other minor bleedings (based on CPT code 99214: level 4 established office patient visit)=$102 [40]. Among VTE patients, one-year medical costs of patients with clinical events relative to patients who did not have a clinical event in 2013 dollars were estimated as the following: recurrent VTE=$58,174 [41], MB=$45,367 [41], CRNMB=$2,140 [42], other minor bleedings (CPT code 99214: level 4 established office patient visit)=$102 [40].
Model outputs: Estimates of differences in medical costs among NVAF patients
Based on the absolute risks determined for each of the clinical events, the total differences in medical costs from a U.S. payer perspective associated with use of each TSOAC vs. warfarin among NVAF and VTE patients were determined [30-36]. Our economic evaluations focused on the medical cost differences driven by clinical outcomes, with drug costs and other additional monitoring related expenses not included in the analyses. In a year, the total differences in medical costs associated with TSOAC use relative to warfarin among NVAF patients were estimated at $204, $140, $495, and -$340 per patient for dabigatran, rivaroxaban, apixaban, and edoxaban, respectively (Table 2) [35].
| Outcome | Dabigatran-150mg vs. warfarin ($/patient-yr) | Rivaroxaban vs. warfarin ($/patient-yr) | Apixaban vs. warfarin ($/patient-yr) | Edoxaban- 60mg vs. warfarin ($/patient-yr) |
| Primary Efficacy Endpoints | ||||
| Ischemic or uncertain type of stroke | ($126) | ($40) | ($37) | $0 |
| Hemorrhagic stroke | ($161) | ($104) | ($132) | ($124) |
| Systemic embolism | ($9) | ($32) | ($3) | ($9) |
| Secondary Efficacy Endpoints | ||||
| Myocardial infarction | $71 | ($88) | ($30) | ($19) |
| Pulmonary embolism or deep-vein thrombosis | $11 | ($1) | ($2) | $1 |
| Safety Endpoints | ||||
| Major bleedings-excluding hemorrhagic stroke | $12 | $122 | ($280) | ($181) |
| Clinically relevant non-major bleedings | $0 | $2 | ($5) | ($8) |
| Other minor bleedings | ($1) | $0 | ($6) | ($1) |
| Total Medical Cost Difference | ($204) | ($140) | ($495) | ($340) |
Table 2: Differences in Medical Costs Among Nonvalvular Atrial Fibrillation (NVAF) Patients Treated with Targeted-specific Oral Anticoagulants (TSOACs) vs. Warfarin [35].
Model outputs: Estimates of differences in medical costs for subgroups of NVAF patients
NVAF patients ≥75 years of age: In the TSOAC vs. warfarin trials the TSOACs and warfarin were reported to have different efficacy and safety profiles among NVAF patients ≥75 and <75 years of age [18-20]. Therefore, we conducted another economic evaluation, which estimated the differences in medical costs for clinical events among NVAF patients ≥75 years of age treated with dabigatran, rivaroxaban, and apixaban vs. warfarin [31]. This economic evaluation estimated that in a year the overall medical cost differences (2010 costs) associated with TSOAC use instead of warfarin among the overall NVAF population to be -$179, -$89, and $485 and among the NVAF population ≥75 years of age to be $199, $14, and $813 for dabigatran, rivaroxaban and apixaban, respectively [31]. Reductions in medical costs for NVAF patients aged ≥75 were observed for those treated with apixaban or rivaroxaban vs. warfarin, but not for NVAF patients aged ≥75 treated with dabigatran vs. warfarin [31]. Additionally, the medical costs reduction associated with apixaban use vs. warfarin among NVAF patients aged ≥75 was nearly twice that of the overall NVAF patient population treated with apixaban instead of warfarin (-$813 vs. -$485 per patient).
Persons ≥75 years of age have a greater risk of stroke, which are more frequently deadly, recurrent, require longer recovery periods and exacerbate concomitant illnesses [44]. In the U.S. in the near future (2020) the AF population is predicted to increase to 7.5 million individuals with an expected prevalence of 13.5% among individuals ≥75 years of age, and 18.2% for those ≥85 years of age [1]. Based on the Framingham study, the stroke risk attributed to AF (24%) is greatest for persons aged between 80 and 89 years [45]. Therefore, the healthcare and economic burdens of AF-related stroke, particularly among older persons are projected to increase and better treatment options, health-wise and cost-wise could potentially lessen these burdens [2,9].
NVAF patients with moderate (CHADS2=2) and higher stroke risk (CHADS2≥3): Since stroke risk in the TSOAC vs. warfarin trials also influenced the efficacy and safety of TSOACs relative to warfarin we also examined the medical cost differences among NVAF patients with moderate (CHADS2=2) and higher stroke risk (CHADS2 ≥ 3) treated with dabigatran, rivaroxaban, and apixaban vs. warfarin [18-20,32]. In this economic evaluation, the medical cost differences associated with TSOACs vs. warfarin varied according to stroke risk [32]. Of the three TSOACs, only apixaban demonstrated consistent medical cost reductions vs. warfarin for NVAF patients with moderate and high stroke risks [32].
NVAF patients with different ranges of warfarin TTR: Lastly, among NVAF patients we examined the impact of different ranges of warfarin TTR on the medical cost differences associated with use of dabigatran, rivaroxaban, and apixaban relative to warfarin [34].
Quartile ranges of warfarin's TTR and corresponding event rates of stroke and systemic embolism (SSE) and MB among NVAF patients treated with warfarin were based on the estimates from the original clinical trials [18-20]. The associations between rates of SSE and MB among warfarin treated patients and TTR were evaluated by linear regression analysis and then the regression coefficients were applied to predict warfarin clinical event rates at various TTR values (30-90%) [34].
In this analysis, an increase in warfarin's TTR corresponded with a decreased risk for stroke among warfarin treated patients and consequently, the differences in medical cost associated with treatment with dabigatran, rivaroxaban, and apixaban relative to warfarin decreased [34]. In contrast to the other TSOACs, the one-year medical cost reduction associated with the use of apixaban instead of warfarin was maintained at all evaluated warfarin TTR values [34].
Model outputs: Estimates of differences in medical costs among VTE patients
Among patients with acute symptomatic VTE the total differences in medical costs associated with TSOAC use relative to warfarin were directionally similar to that of NVAF patients and were estimated at -$146, -$482, -$918, and -$344 per patient per year for dabigatran, rivaroxaban, apixaban, and edoxaban, respectively (Table 3) [33].
| Outcome | Dabigatran vs. warfarin ($/patient-year) | Rivaroxaban vs. warfarin ($/patient-year) | Apixaban vs. warfarin ($/patient-year) | Edoxaban vs. warfarin ($/patient-year) |
| Efficacy Endpoint | ||||
| Recurrent VTE | $114 | ($132) | ($252) | ($197) |
| Safety Endpoints | ||||
| Major bleedings | ($195) | ($354) | ($572) | ($109) |
| Clinically relevant non-major bleedings | ($61) | $4 | ($89) | ($36) |
| Other minor bleedings | ($4) | $1 | ($5) | ($2) |
| Total Medical Cost | ($146) | ($482) | ($918) | ($344) |
Table 3: Differences in medical costs among patients with acute symptomatic venous thromboembolism (VTE) treated with targeted-specific oral anticoagulants (TSOACs) vs. warfarin [33].
We additionally conducted an economic evaluation of the differences in medical costs when dabigatran, rivaroxaban, and apixaban are used vs. placebo for the treatment of patients with VTE for extended periods [36]. The clinical event rates were estimated from the published data of the clinical trials, RE-SONATE, EINSTEN-EXT, and AMPLIFY-EXT as done for prior analyses [24,46,47]. The AMPLIFY-EXT trial included VTE patients treated with 2.5 mg and 5 mg doses of apixiban and data from both treatment arms were used in this economic evaluation [36].
Based on the differences in clinical event rates for VTE patients treated for extended periods with the TSOACs vs. placebo, the total differences in medical costs associated with TSOAC use relative to placebo were estimated at -$2,794, -$2,948, -$4,249 and -$4,244 per patient per year treated with dabigatran, rivaroxaban, apixaban 2.5 mg, and apixaban 5 mg respectively (Table 4) [36].
| Outcome | Dabigatran vs. placebo ($/patient-year) | Rivaroxaban vs. placebo ($/patient-year) | Apixaban 2.5 mg vs. placebo ($/patient-year) | Apixaban 5 mg vs. placebo ($/patient-year) |
| Efficacy Endpoint | ||||
| Recurrent VTE | ($2,995) | ($3,340) | ($4,153) | ($4,121) |
| Safety Endpoints | ||||
| Major bleedings | $133 | $303 | ($111) | ($163) |
| Clinically relevant non-major bleedings | $68 | $89 | $15 | $40 |
| Total Medical Cost | ($2,794) | ($2,948) | ($4,249) | ($4,244) |
Table 4: Differences in medical costs among venous thromboembolism (VTE) patients treated for extended periods with targeted-specific oral anticoagulants (TSOACs) vs. placebo [36].
Univariate (one-way) sensitivity analyses were conducted to determine the effects of varying a single clinical event rate or the corresponding incremental cost on the medical cost differences associated with TSOAC vs. warfarin use among NVAF and VTE patients. In these sensitivity analyses variations in clinical event rates of MBEHS and IS associated with treatment with the different TSOACs among NVAF patients had the greatest influence on the differences in medical costs between the TSOACs and warfarin [35]. Among VTE patients variations in clinical event rates of VTE recurrence and MB associated with treatment with the different TSOACs had the greatest influence on the differences in medical costs between the TSOACs and warfarin [33].
Monte Carlo analyses were also conducted in the economic evaluations as multivariable sensitivity analyses. Descriptive statistics of the total medical cost differences were measured from the results of 10,000 random Monte Carlo cycles. The means of such 10,000 random cycles of Monte Carlo simulations for each TSOAC vs. warfarin comparison were very close to the estimated medical cost differences in the default model analyses.
This showed that the results of the original estimated medical cost differences were relatively robust to random variations. Figure 1 displays an example of the Monte Carlo analysis showing how variations in model parameters influenced the differences in medical costs for NVAF patients.
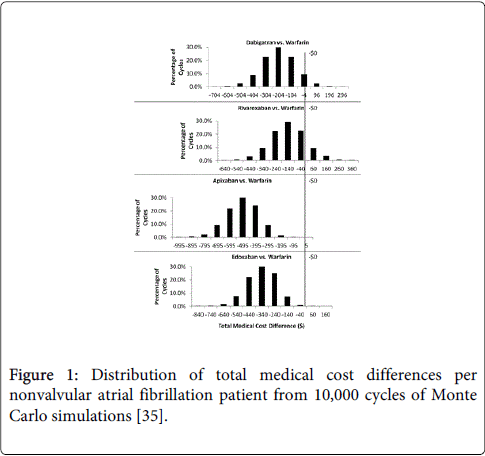
Figure 1: Distribution of total medical cost differences per nonvalvular atrial fibrillation patient from 10,000 cycles of Monte Carlo simulations [35].
Differences in medical costs among combined NVAF and VTE patient population treated with TSOACs vs. warfarin
A hypothetical health plan population in the U.S. with 1 million members was used to estimate and compare the combined medical cost differences for NVAF and VTE patients treated with each of the TSOACs vs. warfarin [35]. Prevalence rates of NVAF and VTE were derived from published literature [48-50]. The same usage rate (i.e. 10%) for each TSOAC was assumed in order to facilitate the comparison of the combined medical cost differences among NVAF and VTE patients treated with the TSOACs vs. warfarin. The usage rates represented approximate proportions of patients who currently receive TSOACs for anticoagulation therapy. Based on an assumed population growth rate of 2% for the hypothetical cohort, the medical cost differences of NVAF and VTE patients treated with the TSOACs vs. warfarin were also projected and compared in the years 2015-2018.
The estimated medical costs differences of NVAF and VTE patient populations among the hypothetical cohort of 1 million insured lives are shown in Table 5. In 2014, among the hypothetical population of one million insured lives, the medical costs were projected to be reduced by $3.0, $2.1, $7.3, and $5.0 million for NVAF patients treated with dabigatran, rivaroxaban, apixaban, and edoxaban, respectively and by $0.7, $2.2, $4.1, and $1.6 million for patients treated for acute symptomatic VTE with dabigatran, rivaroxaban, apixaban, and edoxaban, respectively [35]. In 2014, for the combined NVAF and acute VTE patient population within the hypothetical population of one million insured lives, medical costs were projected to be reduced by $3.7, $4.2, $11.5, and $6.6 million treated with dabigatran, rivaroxaban, apixaban, and edoxaban, respectively [35]. In the model, the reductions in medical costs associated with use of the TSOACs vs. warfarin were projected to steadily increase in the years 2015 to 2018 [35].
| Year 2014 | Year 2015 | Year 2016 | Year 2017 | Year 2018 | |
| Nonvalvular Atrial Fibrillation (NVAF) Patient Population | |||||
| Dabigatran | ($3,025,075) | ($3,085,577) | ($3,147,288) | ($3,210,234) | ($3,274,439) |
| Rivaroxaban | ($2,077,411) | ($2,118,959) | ($2,161,338) | ($2,204,565) | ($2,248,656) |
| Apixaban | ($7,325,621) | ($7,472,133) | ($7,621,576) | ($7,774,008) | ($7,929,488) |
| Edoxaban | ($5,033,264) | ($5,133,930) | ($5,236,608) | ($5,341,340) | ($5,448,167) |
| Venous Thromboembolism (VTE) Patient Population-Acute VTE Only | |||||
| Dabigatran | ($656,304) | ($669,430) | ($682,819) | ($696,475) | ($710,405) |
| Rivaroxaban | ($2,169,134) | ($2,212,516) | ($2,256,767) | ($2,301,902) | ($2,347,940) |
| Apixaban | ($4,131,354) | ($4,213,981) | ($4,298,261) | ($4,384,226) | ($4,471,911) |
| Edoxaban | ($1,550,065) | ($1,581,066) | ($1,612,687) | ($1,644,941) | ($1,677,840) |
| NVAF and Acute VTE Combined Population | |||||
| Dabigatran | ($3,681,379) | ($3,755,007) | ($3,830,107) | ($3,906,709) | ($3,984,843) |
| Rivaroxaban | ($4,246,545) | ($4,331,476) | ($4,418,105) | ($4,506,467) | ($4,596,596) |
| Apixaban | ($11,456,975) | ($11,686,115) | ($11,919,837) | ($12,158,234) | ($12,401,398) |
| Edoxaban | ($6,583,329) | ($6,714,996) | ($6,849,296) | ($6,986,281) | ($7,126,007) |
Table 5: Differences in medical costs among nonvalvular atrial fibrillation (NVAF) patients and patients treated for acute venous thromboembolism (VTE) of a hypothetical cohort of 1 million insured lives (2014-2018).
Economic model based on real-world event rates of patients with VTE
We additionally have estimated the real-world differences in medical costs from a U.S. payer perspective when TSOACs are used instead of warfarin for the treatment of patients with acute symptomatic VTE [51]. Reduction of real-world event rates of recurrent VTE and MB were obtained by applying rate reductions from the TSOACs vs. warfarin trials [22-28] to the Worcester study population, which was comprised of residents from metropolitan Worcester, MA in the years 1999, 2001, and 2003 [52]. Incremental annual medical costs among patients with VTE and MB from a U.S. payer perspective were obtained as mentioned in the prior analysis. Differences in total medical costs for VTE patients treated with TSOACs vs. warfarin were then estimated. Univariate and Monte Carlo sensitivity analyses were additionally carried out.
Real-world event rates of recurrent VTE and MB in the Worcester VTE study were 11.2% and 10.8%, respectively [51,52]. Differences in real-world event rates of recurrent VTE among VTE patients treated with TSOACs instead of warfarin were estimated at 1.02% for dabigatran, 1.23% for rivaroxaban, -1.80% for apixaban, and -2.02% for edoxaban [51]. Differences in real-world event rates of MB among VTE patients treated with TSOACs instead of warfarin were estimated at 2.57% for dabigatran, -4.97% for rivaroxaban, -7.48% for apixaban, and -1.73% for edoxaban [51]. Based on the real-world data, the one-year total medical cost differences associated with TSOAC use vs. warfarin were greatest for VTE patients treated with apixaban ($4,440 per patient year-ppy), followed by those treated with rivaroxaban ($2,971 ppy), edoxaban ($1,957 ppy), and dabigatran (-$572 ppy) [51]. From the 10,000 random variations in each of the Monte Carlo multivariate analyses the mean cost reductions associated with use of the TSOACs vs. warfarin among VTE patients were similar to that estimated in the default analysis, with use of apixaban associated with the greatest medical cost reduction vs. warfarin [51]. Apixaban was associated with a cost reduction in 100% of the 10,000 Monte Carlo iterations, while approximately one-third of the iterations for dabigatran showed a medical cost difference >$0 (cost increase) [50]. Rivaroxaban and edoxaban showed a medical cost difference <$0 in 99% and 95% of the 10,000 Monte Carlo iterations, respectively [51].
Since the differences in VTE and MB rates were substantially greater among patients treated with TSOACs vs. warfarin in the community setting in comparison to patients who participated in clinical trials the medical cost reductions associated with TSOAC use vs. warfarin were also much greater than previously estimated using clinical trial data [33,51,52]. The differences in recurrent VTE and MB rates among patients in the clinical trials and those in the Worcester study can be attributed to several factors. Firstly, patients who participate in clinical trials receive carefully planned treatments and monitoring and therefore, their quality of care may be greater than that in real-world settings. Secondly, the clinical characteristics of the Worcester study population were different from that of the TSOAC vs. warfarin trial populations [22-28,52]. The patient population in the Worcester study had a greater mean age, (65 years vs. 54-58 years in TSOAC trial populations) and approximately 50% had a provoked initial VTE event, while the proportions of patients in the clinical trials with a provoked VTE event were lower [22-28,52]. Other real-world observational studies have also reported high VTE recurrence rates, with 5-year cumulative incidence rates ranging between 21.5%-29.1% [53,54]. The higher MB rate in the Worcester study, relative to that of the TSOAC clinical trials, may also be related to the greater age and high prevalence of comorbidities of the Worcester study population [22-28,52].
As the latter real-world study showed, the economic evaluations based on clinical trial data may under estimate the differences in medical costs associated with use of TSOACs vs. warfarin for the treatment of NVAF and VTE. Additionally, the clinical event rates for each of the TSOAC comparisons with warfarin are based on only one randomized control trial and direct comparison trials between the TSOACs have not been done. Differences among trial designs, outcome definitions, and patient populations also complicate the cross-trial comparisons. Another issue with the clinical trial data, is that some trials were designed as non-inferiority trials. However, use of such data is common in economic models of clinical trial findings, since clinical trials are generally not powered for the economic evaluations of trial results. The economic evaluations have other limitations in that monitoring related expenses, as well as the long-term burden of clinical events, indirect costs, and quality of life, all of which may be impacted by more efficacious pharmacotherapy for NVAF and VTE were not taken into account. Further studies incorporating all of these costs, as well as drug costs will provide valuable information for healthcare providers, patients, and health policy makers and will likely be best accomplished using a real-world observational study design. The incremental annual medical costs for patients with clinical events were based upon those obtained from published studies, which estimated costs from different U.S. health insurers. Therefore, the medical costs are generalized and may not apply to specific payers of U.S. health plans and also healthcare systems outside of the U.S. In regard to the real-world study, the Worcester VTE patient population differed from the clinical trial study populations in VTE recurrence risk, pre-existing conditions, and other characteristics, which may have influenced the clinical event rates and hence the estimates of medical cost differences [51]. Therefore, the validity of the estimates of the differences in medical costs between the TSOACs and warfarin may need to be further assessed when applying the study findings to other geographic regions in the U.S.
Based on our economic evaluations using clinical trial data, annual medical costs were estimated to be lower for NVAF and VTE patients treated with TSOACs vs. warfarin [30-36]. Among both NVAF and VTE patients, treatment with apixaban instead of warfarin was estimated to be associated with the greatest reductions in medical costs, which were driven by medical cost reductions associated with both efficacy and safety endpoints [30-36]. We extrapolated the results of our economic models to a combined population of NVAF patients and acute VTE patients among a hypothetical cohort of 1 million insured lives. The results of this economic evaluation showed that medical costs are projected to be reduced in 2014 by $3.7, $4.2, $11.5, and $6.6 million for NVAF and VTE patients treated with dabigatran, rivaroxaban, apixaban, and edoxaban, respectively [35]. Additionally, the reductions in medical costs associated with use of the TSOACs were projected to steadily increase in the years 2015 to 2018 [35]. As mentioned, the direct application of our results based on clinical trial data to the real-world setting where many other factors, including local healthcare cost, drug adherence, population risk, and health behaviors may vary, will require further assessment. However, prior to the broad exposure of TSOACs to the real world, clinical trial results are considered the best basis for conducting this type of research [55,56].
The efficacy of warfarin for reducing stroke risk and recurrent VTE is markedly influenced by its time in therapeutic range (TTR), referring to the time patients treated with warfarin spend having an international normalized prothrombin time ratio (INR) within the therapeutic range (INR=2-3) [11,14,57]. A meta-analysis of several observational studies conducted on AF patient populations in the U.S. reported that AF patients spend only about half the time in the therapeutic range of warfarin [58]. A study of Medicare beneficiaries with NVAF has reported that warfarin therapy was only associated with a stroke risk reduction of 35%, almost half of what has been reported in clinical trials [59]. This lower efficacy of warfarin in the real-world setting is also apparent among VTE patients, with a study of VTE patients treated in the usual community practice setting finding that patients were only in the warfarin therapeutic range 38% of the time and that the risks of recurrent VTE and MB were much higher than observed in clinical trial settings [60]. The suboptimal management of warfarin therapy in routine practice likely contributes to its reduced efficacy in the real-world. Additionally, the underutilization of warfarin therapy and low adherence levels in the real-world setting put many patients with NVAF and VTE at unnecessary risk for negative outcomes [13,61]. Since routine anticoagulation management and low adherence levels to warfarin were not taken into account in our economic evaluations, the medical cost differences associated with TSOAC use relative to warfarin may be much more substantial when further examined in the real world. Based on the clinical burden of stroke among the AF patient population in 2003 in the U.S., Caro (2004) estimated that optimizing warfarin therapy or using one of the TSOACs for just half of all patients with AF, who have suboptimal anticoagulation or no anticoagulation, would save Medicare nearly 2.5 billion dollars annually in costs related to stroke, major bleeding, monitoring visits, and tests [62].
Other cost-effectiveness studies, using different economic modeling approaches, have produced similar results as our economic evaluations [63-67]. A cost-effectiveness study using a Markov approach from a U.S. payer perspective reported that compared with warfarin, apixaban (5 mg) had an incremental cost-effectiveness ratio (ICER) of $15,026 per quality-adjusted life-year (QALY) gained, which is well below the threshold of $50,000 per QALY gained [63]. Additionally, Harrington et al. compared the cost-effectiveness of dabigatran, rivaroxaban, and apixaban vs. warfarin and using the Markov model predicted that of the three TSOACs, apixaban was the preferred anticoagulant for their hypothetical cohort of 70-year old patients with NVAF, as it was most likely to be the cost-effective treatment option at all willing-to-pay thresholds >$40,000 per QALY gained [63]. For the study by Harrington et al. the cost of apixaban was not yet available in the U.S. and was estimated by converting its cost in the U.K. to U.S. dollars, which resulted in a higher yearly cost than both dabigatran and rivaroxaban [63]. The cost-effectiveness of the TSOACs in Harrington et al. study was influenced by drug pricing and the results may be more favorable to apixaban in an updated analysis, in which all drug costs of TSOACs are the same [63]. Currently, the Wholesale Acquisition Costs of dabigatran, rivaroxaban, apixaban, and edoxaban in the U.S. are similar [35,64]. Thus, in our economic evaluations the drug prices of TSOACs are not likely to affect the relative cost differences among the four TSOACs. Another cost-effectiveness study estimated that among AF patients over a lifetime apixaban use was associated with the greatest gain of QALYs vs. warfarin use, followed by use of dabigatran, and use of rivaroxaban [65]. A cost-effectiveness study with a U.K. perspective also found apixaban to be the most cost-effective TSOAC alternative to warfarin among NVAF patients [66]. Economic evaluations have not been published that have compared the cost effectiveness of edoxaban with other TSOACs relative to warfarin among NVAF and VTE patients. Although, one study did predict that edoxaban was cost effective compared with warfarin for the treatment of NVAF patients in the Italian healthcare system [67].
Warfarin for NVAF and VTE treatment in comparison to TSOACs is less expensive when only drug costs are taken into account. However, the avoidance of NVAF- and VTE-related clinical events and hence lower healthcare costs should assist clinicians and health policy makers in determining the most cost-effective pharmacotherapies. Having the medical costs for clinical events avoided as a component of overall drug cost is highly relevant given the fact that hospitalizations and physician/clinical services account for 51% of all U.S. health expenditures [68]. Given our aging population and the increasing prevalence of NVAF and VTE there is greater need for anticoagulation therapy [1-4]. Compared to traditional warfarin therapy we have shown that the TSOACs have considerable cost advantages for the treatment of patients with NVAF or VTE. It is important now and in the future to balance optimizing the quality of care and hence, patient outcomes with reducing pharmacotherapy costs as this is a central strategy of healthcare reform for improving healthcare quality and driving clinical practice innovation.
The introduction of TSOACs to the market for treatment of NVAF and VTE allows for physicians and patients to have multiple alternative therapies for more individualized treatment. In addition to the different efficacy and safety profiles of TSOACs and their potential differences in medical cost savings vs. warfarin, the choice of the most appropriate TSOAC alternative to warfarin also must take into account their limitations of use and use in specific patient populations (Table 6). Prescribing information for edoxaban indicates that it should not be used in NVAF patients with creatinine clearance >95 mL/min because of increased risk of ischemic stroke compared to warfarin [37]. The other TSOACs do not have specific limitations of use listed in the indications of prescribing information [69-71]. However, the TSOACs do differ to some extent in their use in specific NVAF and VTE populations [37,69-71], such as dabigatran use may need to be modified in geriatric patients with increased bleeding risk. TSOAC use may also need to be restricted or dose adjusted for NVAF patients with hepatic and renal impairment [37,69-71].
| Dabigatran | Rivaroxaban | Apixaban | Edoxaban | |
| Treatment of nonvalvular atrial fibrillation (NVAF) patients | To reduce the risk of stroke and systemic embolism in patients with NVAF |
To reduce the risk of stroke and systemic embolism in patients with NVAF | To reduce the risk of stroke and systemic embolism in patients with NVAF | To reduce the risk of stroke and systemic embolism in patients with NVAF |
| Limitations of use in NVAF patients | None | None | None | Should not be used in patients with creatinine clearance >95 mL/min because of increased risk of ischemic stroke compared to warfarin |
| Treatment of patients with deep vein thrombosis (DVT) and pulmonary embolism (PE) | For the treatment of DVT and PE in patients who have been treated with a parenteral anticoagulant for 5-10 days To reduce the risk of recurrence of DVT and PE in patients who have been previously treated |
For the treatment of DVT, PE, and for the reduction in the risk of recurrence of DVT and of PE | For the treatment of DVT and PE, and for the reduction in the risk of recurrent DVT and PE following initial therapy |
For the treatment of DVT and PE following 5-10 days of initial therapy with a parenteral anticoagulant |
| Use in specific populations | Geriatric use: Risk of bleeding increases with age | Nursing mothers: discontinue drug or discontinue nursing | Pregnancy: Not recommendedNursing Mothers: Discontinue drug or discontinue nursing | Nursing mothers: Discontinue drug or discontinue nursing |
| Renal impairment: Avoid or adjust dose based on creatinine clearance Hepatic impairment: Avoid use in patients with Child-Pugh B and Chepatic impairment or with any degree of hepatic disease associated with coagulopathy |
Severe Hepatic Impairment: Not recommended | Impaired renal function (creatinine clearance 15 to 50 mL/min): Reduce dose Moderate or severe hepatic impairment: Not recommended |
Table 6: FDA Approved Indications of Targeted-specific Oral Anticoagulants (TSOACs) [37,69-71].
When any of the TSOACs are used instead of warfarin for NVAF and VTE treatment medical costs are projected to be reduced, with apixaban being associated with the greatest reduction in medical costs. The estimated medical cost reductions associated with TSOAC use, relative to warfarin may be helpful in determining the overall cost impacts of the use of TSOACs among NVAF and VTE patients in the U.S., although, further evaluation is warranted.
Declaration of funding: Sponsorship of this review and article processing charges were funded by Bristol-Myers Squibb and Pfizer.
Declaration of financial/other relationships: Alpesh Amin was a paid consultant to Novosys Health for research only and received no funding for the development of this manuscript. Amanda Bruno is an employee of Bristol-Myers Squibb and owns stock in the company. Jeffrey Trocio is an employee of Pfizer and owns stock in the company. Jay Lin and Melissa Lingohr-Smith are employees of Novosys Health, which received research funds from Bristol-Myers Squibb and Pfizer in connection with conducting this review and development of this manuscript.