Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2014) Volume 4, Issue 3
Pancreatic head resection represents one of the most demanding procedures in abdominal surgery; however, several complications may develop after this type of surgery such as fistulas (internal and/or external), gastrointestinal tract hemorrhage, and abdominal infections. The relaparotomy rate, as well as low perioperative mortality, may be present. The reported postoperative complication rate may range from 23 to 57%, even when an expert surgeon performs the resection. However, late complications of pancreatic head resection are rare. A case of double gastrojejunocolic fistula, which developed in a patient who had undergone pancreatic head resection some years earlier, is herein reported. The patient was admitted to our hospital for abdominal pain associated with nausea and vomiting. She also complained of diarrhea after food ingestion, even in small quantities, and referred the presence of undigested food in the feces and a weight loss of 10 kg in the previous three months. The patient was treated conservatively. We should be aware that symptoms of fistulas due to pancreatic head resections may be diagnosed several years after surgery.
<Keywords: Surgical complication, Pancreatic head resection, Pancreatic fistula, Medical treatment
Pancreatic head resection represents one of the most demanding procedures in abdominal surgery; however, several complications may develop after this type of surgery such as fistulas (internal and/or external), gastrointestinal tract hemorrhage, and abdominal infections [1-3]. The relaparotomy rate, as well as low perioperative mortality, may be present [1-3]. The reported postoperative complication rate may range from 23 to 57%, even when an expert surgeon performs the resection [1-3]. However, late complications of pancreatic head resection are rare. A case of double gastrojejunocolic fistula, which developed in a patient who had undergone pancreatic head resection some years earlier, is herein reported. This case is interesting because, to our knowledge there are no data in literature of so late diagnosis of double gastrojejunocolic fistula in patients operated for pancreatic head resection.
A 54-year-old female patient of was admitted to our hospital for abdominal pain associated with nausea and vomiting. She also complained of diarrhea after food ingestion, even in small quantities, and referred the presence of undigested food in the feces and a weight loss of 10 kg in the previous three months.
The patients were operated on 4 years before admission to our hospital for pancreatic head resection using the Whipple procedure for the presence of a non-functioning pancreatic neuroendocrine tumor. Ten days after this procedure, a relaparatomy was carried out due to the presence of dehiscence of the gastro-intestinal anastomosis. Six months after the operation, she developed hepatic metastases, and underwent chemotherapy and chemoembolization.
In the Emergency Room, a chest radiograph was normal and an X-ray of the abdomen showed a modest bloating of the loops of the small intestine at the level of the central portion of the abdomen in translateral projection; there was no evidence of free intraperitoneal air. An ultrasound of the abdomen confirmed the presence of multiple nodules of which the largest was in the right lobe on the sixth hepatic segment; the major hepatic lesion was 4×6 cm in diameter; no other alterations in the residual pancreas, kidneys and spleen were detected. On admission to our department, the patient was alert, oriented and cooperative; the arterial pressure was 110/70 mmHg, the cardiac rate was 76 beats per minute and peripheral oxygen saturation was 96%. The cardiopulmonary physical examination was normal whereas the abdomen was tender, especially in the upper abdominal sections and in the left iliac fossa; the bowel sounds were normal. The laboratory tests carried out during hospitalization were normal, and nonspecific alteration of ventricular repolarization was present at electrocardiogram.
The patient underwent abdominal contrast-enhanced computed tomography that confirmed the finding of the ultrasonography and, in addition, showed the presence of a possible fistula coming from the surgical jejunal anastomosis to the colon (Figure 1); in fact, small air bubbles were present in the pericolonic fat. To better investigate, we carried out a barium X-ray of the upper digestive tract (Figure 2) which showed the presence of two fistulas from the surgical anastomosis and the transverse colon; no stenosis of the jejunal loop was found. The glucose breath test was positive for bacterial ileal contamination. The patient refused the surgical approach for the closure of the fistulas and was medically treated with fasting proton pump inhibitors given intravenously, intestinal decontamination and parenteral nutrition for 15 days. The patient was then cautiously re-fed with solid food and pancreatic extracts. The patient was clinically followed and regained her weight. Currently the patient is still asymptomatic; she continues chemotherapy for her disease and continues with repeated courses of non-absorbable antibiotics orally.
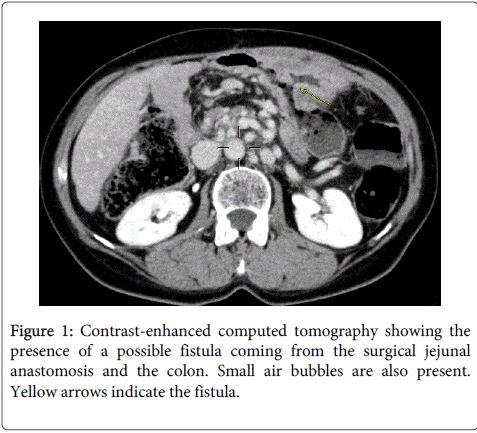
Figure 1: Contrast-enhanced computed tomography showing the presence of a possible fistula coming from the surgical jejunal anastomosis and the colon. Small air bubbles are also present. Yellow arrows indicate the fistula.
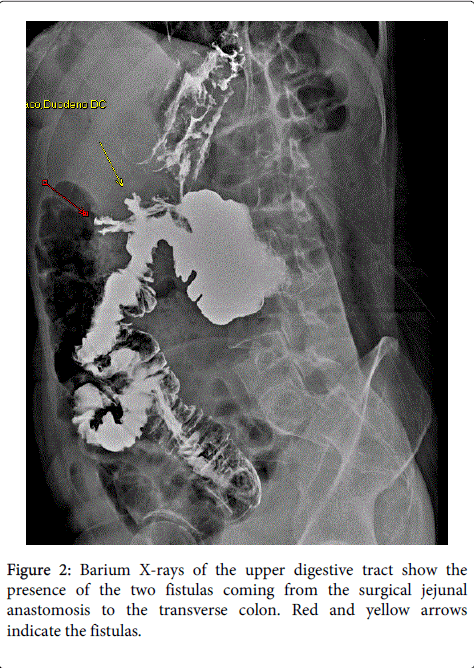
Figure 2: Barium X-rays of the upper digestive tract show the presence of the two fistulas coming from the surgical jejunal anastomosis to the transverse colon. Red and yellow arrows indicate the fistulas.
In Western Countries, the most common cause of ileo-colonic fistula is adenocarcinoma of the colon while, in Japan, adenocarcinoma of the stomach is the most frequent cause [4]. It seldom appears, as a complication of a benign peptic ulcer, in Crohn's disease or as the result of a significant intake of steroids or NSAIDs. The typical symptoms of a gastrocolic fistula are abdominal pain, nausea, vomiting, diarrhea and weight loss [4]. Our patient had all the reported symptoms, such as abdominal pain, nausea, vomiting, diarrhea and weight loss. The novelty is that our patient developed these symptoms after a number of years after the surgery
Pancreatic head resection is an established procedure for the treatment of benign and malignant diseases of the pancreas and the periampullary region. In order to decrease morbidity and mortality, several options have been suggested to avoid the activation of pancreatic juice by biliary secretion and, consequently, to reduce the appearance and severity of a pancreatic fistula [5]
It has also been reported that barium X-rays and CT findings have an equal role in the diagnosis [4] and our case confirms these data in the literature. In fact, since the patient refused the surgical approach, the problems related to the presence of the fistulas was resolved using medical therapy, and she is presently in satisfactory clinical condition
We should be aware that fistulas due to pancreatic head resections might be diagnosed several years after surgery when symptoms appear.