Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2015) Volume 3, Issue 3
Background: We conducted a retrospective study that focused on the disposition of excess embryos produced from ART at a hospital storage facility, and analyzed response rates and embryo decisions made as a result of these procedures.
Methods: Data collected from 552 patients from 2000-2011 included the number and content of written correspondences during time of storage, and on the final dispositions. We calculated the time it took to receive a response each year, assessed the decisions made, and reasons for non-response. Comparisons were made using chi square for categorical variables and ANOVA for continuous variables with significance at P < 0.05.
Results: The percentage of responses declined with increasing years in storage, and increased for nonresponse. Frozen embryo transfer (FET) and donation were the most common decisions; discard was made more frequently in year 1 than later years. After the maximum five years of storage, 34 of the 246 (13.8%) patients who still held embryos had never responded, resulting in default discard. There was no difference in the final decision made according to age, diagnosis of diminished ovarian reserve, or live birth at first cycle.
Conclusions: This study demonstrates the challenges in receiving time-sensitive responses from patients with regard to the disposition of their embryos; more studies are needed to further evaluate short-term storage facility protocols that assist in decision-making in effective ways.
<Keywords: Assisted reproductive technology; Frozen embryos; Embryo disposition; Cryopreservation; Embryo discard
It is well known that assisted reproductive technology (ART) treatment often results in excess embryos available to be cryopreserved for future use. Frozen embryos can remain viable indefinitely and are generally maintained by a patient or couple with the goal of proceeding with a frozen embryo transfer (FET) in the attempt to achieve pregnancy at a future date. Nevertheless, after a period of storage without use, other options must be sought. In addition to FET, options for embryo disposition have historically included donation to another couple, donation to research [1], continued storage, or discard.
The issue of how to deal with unclaimed excess embryos for which decisions has not been made, or which have been abandoned, has continued to be of great concern to clinics and has been addressed by national professional organizations [2]. Problems that occur include failure of contact due to a change of address, changes in a couple’s marital status, or inability to make decisions in a timely manner. Decisions about disposition of abandoned embryos is a particularly difficult issue because of the sensitive nature of the moral status of the human embryo resulting in hesitation about the ethical and legal aspects of the option of embryo discard on the part of the clinic. Nevertheless, it has been suggested that some of the problems with frozen embryos arise from the fact that clinic procedures are not clearly defined with regard to disposition, informed consent, and patient decision-making [3].
Recognizing that disposition of frozen embryos was an issue that required a clear policy and advance decision-making on the part of couples, the Dartmouth-Hitchcock (D-H) ART program, in conjunction with the Risk Management Department and the Hospital Ethics Committee instituted a policy early in its embryo freezing program to define the options for storage, disposition, discard, and to obtain advance consent from patients for the processes involved. Rather than have patients make decisions before treatment, the consent process informs patients in advance of clinic procedures for obtaining dispositional decisions for cryopreserved embryos and further informs them that failure to adhere to these procedures will result in discard of the embryos. The goal of this study was to evaluate the efficacy of this embryo disposition protocol. Our study focuses solely on patients with excess embryos stored at D-H and includes an analysis of response rates, the decisions made and not made as a result of the D-H ART program’s procedures.
D-H policy on embryo disposition
The D-H written policy on frozen embryos includes a multi-step process that begins at the initiation of an ART cycle (Figure 1). Verbal and written consent includes informing the patient/couple with excess cryopreserved embryos that they will be contacted annually and that they are expected to decide on one of several choices for disposition of the embryos. They must contact the clinic in writing within 30 days of receipt of the letter with this decision. Letters include a form to be filled out and an envelope that is stamped and self-addressed to the clinic. At the time of consent, patients acknowledge their understanding that they are expected to keep the D-H ART program informed of their current address and marital status and to pay storage bills as long as they have embryos frozen at the facility. Every year that embryos remain in storage, patients are sent this letter giving them one of 5 options with regard to the embryos: to undergo a frozen embryo transfer cycle, to donate the embryos to another couple, to donate to research, to have the embryos shipped to a long term storage facility, or to have the embryos discarded. When excess embryos are first frozen, patients are sent a letter informing them of how many excess embryos are being stored and reconfirming the above expectations. Patients pay a yearly fee for maintaining the embryo(s). If the ART program does not hear back from the patients within 30 days of letters sent, 2 additional letters are sent in the attempt to obtain the requested information. These two letters both contain the date for discard if no response is obtained. The final letter is a brief warning letter in bold type defining a date for discard with a stark warning that this will occur if the patient has not responded. This final letter is sent by certified mail. In the fifth year of storage, a similar protocol for mailing letters is carried out, but in this year the option for continued storage is omitted. All communication with patients is by letter and responses are expected in writing. Occasionally letters are sent regarding storage bills and failure to respond to these after 3 attempts also results in embryo discard.
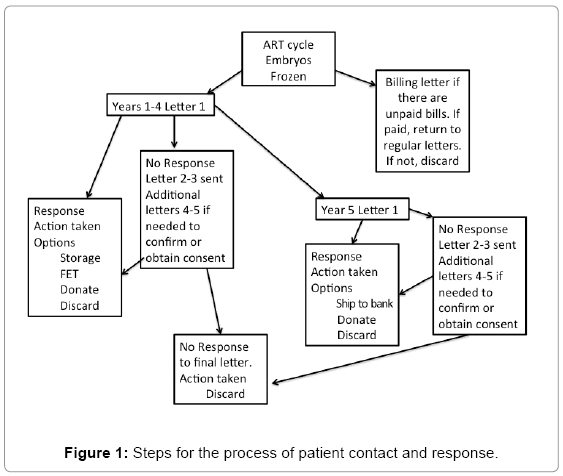
Figure 1: Steps for the process of patient contact and response.
All communications with the patients, including letters sent and received, are stored in the medical record. Once it is decided that embryos are to be discarded because patients did not respond or pay their storage bill, no further contact with them is attempted. A disposal form is completed that includes a detailed account of the time course of the attempted communication with the patient including dates and clinic personnel involved, and the final reason for disposal. For those patients who never responded, complete documentation prior to discard requires chart review to ensure that patients did not give any verbal response to anyone at the clinic. A final check with the billing office also confirms that payment for storage was not recently received. Final chart review and approval signatures by the Laboratory Director and the Physician of record are then required. With this paperwork in hand, the Laboratory Director and one other embryologist perform the discard and confirm identity of the discarded embryos.
Patient population and data collected
The study included all D-H ART patients with embryos frozen between 2000 and 2011. We collected data on disposition of the embryos from the first freeze within this timeframe on any patient. Information collected included the number of embryos frozen, and for each year (years 1-5) the number of days after the freeze date that the first letter was sent, the manner of patient response (telephone, letter, other communication), and any decision made. Possible decisions included embryo transfer including how many embryos were thawed and transferred and how many remained frozen; storage for another year; donation to another couple or to research; shipment off-site to long term storage; and discard. The study was approved by the Dartmouth Committee for the Protection of Human Subjects.
Outcome parameters
Outcome parameters included the number of patients who were contacted per year, number of letters needing to be sent prior to receiving a response, response received, number of patients who never responded and any complications. We analyzed each of these categories separately to also ascertain the frequency of different decisions made, and to calculate the average length of time it took to receive a response from patients each year. The length of time between sending and receiving a letter was measured in days since the first letter was sent. Length of time for letters sent in subsequent years was also measured in days from when the embryos were frozen.
Statistics
Comparisons were made using chi square for categorical variables and ANOVA for continuous variables with significance at P < 0.05.
The study population included 552 patients/couples who froze embryos between 2000 and 2011. The age of the female partners in these couples was 33.7 +/- 4.7 years and 12.9% had a diagnosis of diminished ovarian reserve. of the 552 patients, 38.3% had a live birth from their first cycle of treatment and 183 (33.3%) made a decision regarding embryo use before a letter was required at the end of year 1. As shown in Table 1 the number of first of the yearly letters required for each of the sequential years were 369 in year 1 and 211, 128, 70, and 37 letters in years 2 through 5 respectively. The percentage of responses to first letters declined with increasing years in storage and percentage with no response after all letters were sent increased with sequential years.
| Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | P | |
|---|---|---|---|---|---|---|
| Patients receiving letters (N) | 369 | 211 | 128 | 70 | 37 | |
| Responses Received (%) | ||||||
| Letter 1 | 73.6 | 65.9 | 59.4 | 48.5 | 45.9 | <0.0001 |
| Letter 2 | 17.9 | 19.9 | 16.4 | 20.0 | 18.9 | |
| Letters 3-5 | 4.5 | 9.4 | 16.4 | 14.2 | 10.8 | |
| No Response | 4.1 | 4.7 | 7.8 | 17.1 | 18.9 |
Table 1: Responses to letters.
The decisions made by patients are shown in Table 2. In years 1-3 the majority of decisions were for extension of storage with decision for this choice declining in years 4 and 5. Between 5% and 14% chose FET in each year while 8-14% chose to donate either to research or to another couple. A small percentage (1.4%) chose shipping to long term storage in years 1 and 2 with 40.5% choosing this option by year 5, the final year of storage. Decision to discard was made more frequently in year 1 than in subsequent years.
| Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | P | |
|---|---|---|---|---|---|---|
| Patients receiving letters (N) | 369 | 211 | 128 | 70 | 37 | |
| Extension | 61.0 | 67.3 | 57.0 | 47.1 | 8.1 | <0.0001 |
| Frozen Embryo Transfer | 8.1 | 10.0 | 5.5 | 5.7 | 13.5 | |
| Donate (research or pt) | 9.2 | 8.5 | 11.7 | 10.0 | 13.5 | |
| Long term storage | 1.4 | 1.4 | 5.5 | 7.1 | 40.5 | |
| Discard | 15.7 | 7.1 | 11.7 | 10.0 | 0.0 | |
| Other/junk | 0.5 | 0.9 | 0.8 | 2.9 | 5.4 | |
| No decision made | 4.1 | 4.7 | 7.8 | 17.1 | 18.9 |
Table 2: Disposition decisions.
Per protocol, each letter was expected to be sent by the clinic at 1 year post freeze, and on the anniversary of this date in subsequent years. Evaluation of time to letter sent indicated that we sent these within 25 days of this date on each year (Table 3). Time to response (and consequently, number of letters required) took longer with each subsequent year in storage.
| Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | P | |
|---|---|---|---|---|---|---|
| Days from Freeze | 390.0±77.5 | 751.1±72.0 | 1120.4±90.7 | 1489.0±104.8 | 1833.8±109.0 | |
| Average days from year | 25 | 21 | 25 | 29 | 8 | |
| Responses at >year+30 days N (%) |
61 16.5% |
55 26% |
31 24% |
21 30% |
8 21% |
|
| Days to Response | 35.9±39.8 | 38.5±32.6 | 48.6±51.0 | 47.5±39.0 | 52.0±50.1 | 0.004 |
Table 3: Timing of letters sent and received for years 1-5 letter 1.
When looked at in total as of year 5, of the 246 patients who did not use their embryos for an FET cycle in years 1-5, 74 (30.1%) chose to donate, 34 (13.8%) chose long term storage, 104 (42.3%) requested embryo discard, and 34 (13.8%) never responded resulting in discard by default. There was no difference in final decision made according to age, diagnosis of diminished ovarian reserve, or live birth at first cycle.
There has long been discussion of how clinics can and should deal with embryos maintained in cryostorage. In this study, we reviewed the procedures at a single clinic in the U.S. These procedures were specifically designed to deal with issues of patient contact and lack of response to contact. We found that even a clear and concise protocol for follow up of embryos in storage met with a need for multiple letters before decisions from patients could be received and that nearly 14% of patients with embryos at 1 year post freeze never made final disposition decisions. The process required to obtain this information was one that resulted in clinic staff writing multiple letters and expending considerable time and effort.
Nachtigall et al. [3] have suggested that patient decisions about frozen embryo disposition would be facilitated by clear procedures, counseling, and guidance about options. The procedures established at our clinic attempted to accomplish these ends. Nevertheless, our data show that, in spite of a clear informed consent procedure, clinic staff had to send multiple communications to obtain responses from many patients. Our numbers show that first letters each year were sent in a timely manner by the clinic. However, in this first year of storage more than one letter was required for 26.7% of patients. The percentage requiring multiple letters increased to the final year of storage when over 50% of remaining patients required more than one letter. Patient time to response also increased with successive years (Table 3). Embryo discard, when required for those who did not respond to letters, similarly resulted in clinic staff expending a significant effort in chart review procedures. In 2011, Provoost et al. [4] used a mailed survey and found that 12% of patients who did not reply did so due to the fact that they were older, had a negative outcome, and their treatment occurred many years prior to the survey. This group was more likely to be childless and also had anticipated having more regret if they were to make a clear decision than the group of patients who ultimately made a disposition decision. In our study, age and outcome of the first cycle did not significantly affect response.
Disposition decisions in the first years post freeze in this study most frequently included continued storage, but a significant portion of the patients chose continued storage even as the years progressed. Ultimately, 30% of patients who did not use their embryos for an FET chose to donate to either research or another couple and 42% chose the option to discard. The numbers for donation differ somewhat from those of Newton [5] who found that over 50% chose donation to either research or another couple, although discard was chosen by 42% in that study as well. A greater percentage in our study chose long term storage (13.8% vs. 6%, respectively). Differences could reflect the fact that differences in cultures and backgrounds affect patient decisions as demonstrated by a prior study in which decisions differed for patients from different countries [6].
Many previous studies on IVF patients’ decisions on what to do with excess embryos have focused on the decisions made, but have not focused on patients’ response rates or hospital storage policies. Using interview methodology, De Lacey [7] identified reasons for which patients donated embryos to other couples or had them discarded, and found that patients tended to focus on a pregnancy termination metaphor when thinking about embryo discard and donation as options. Provoost et al. [8] sought reflections from IVF patients who had excess embryos and found that there were two groups of patients, those who wanted continued storage even though their family building was completed and those who wanted to discard their embryos even though they had not ruled out the possibility of having another child. Haimes and Taylor [9] studied IVF patients making decisions about what to do with excess embryos while still going through their treatment cycle and found that patient’s thoughts on donation to research were heavily influenced by their real-time struggles with ART success and less on the moral status of the embryo. Provoost et al. [10] studied patients who had excess embryos and questioned how patient understanding of scientific research involving embryos affected their decisions to donate excess embryos to research or to choose instead to discard them; the study indicated that many patients do not fully understand the donation process or the research being done. Several other studies compare donation to research versus other patients [11- 14] a distinction we did not make in this study due to the fact that we influenced patient decisions on this matter as our program has strict criteria for accepting embryos for donation to other patients.
This study makes clear the difficulty for clinics in getting timely responses from patients with regard to the disposition of their embryos. Alternately, our procedures did facilitate the discard of embryos that were ultimately abandoned. Using our procedures that included prior consent for discard if a response was not obtained from them, we were able to ultimately discard those embryos for patients who did not respond to the communications. Procedures provided a method for dealing with abandoned embryos that is not available to many clinics and results at those clinics in indefinite continued storage of the embryos.
The strength of this study is that it evaluates outcomes at a single clinic with clearly delineated procedures and a robust consent process. The retrospective nature of the study also imposed several limitations. Some information that might have been helpful such as religion and patient beliefs about the moral status of the embryo were not available to us. We therefore could not evaluate reasons for non-response. These reasons could have included patients who moved away and didn’t leave forwarding addresses as well as patients who simply declined to make a decision.
In summary, this study evaluated one clinic’s policy on embryo storage and found that even with clear guidance and significant time spent on informed consent of patients, follow up on with them on disposition of their frozen embryos can be challenging.