Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Research Article - (2015) Volume 4, Issue 1
Purpose: The objectives of the study were: (1) to determine kanamycin plasma concentrations using liquid chromatography coupled with mass spectrometry (LC-MS), (2) to investigate kanamycin pharmacokinetics (PK) in patients with multi-drug resistant tuberculosis (MDR-TB), (3) to find out whether HIV infection, kidney dysfunction and antiretroviral drugs influence kanamycin PK.
Methods: The study was designed as a non-randomized study involving male and female HIV- positive and HIV negative patients admitted for MDR-TB treatment. Blood samples were collected before (baseline) and ½, 1, 2, 4, 8 and 24 hours after intramuscular injection of kanamycin. LC-MS was used to quantify kanamycin plasma concentrations.
Results: Thirty one patients including 13 HIV (+) participated in the study. The lower limit of detection and lower limit of quantification of kanamycin were 0.06 μg/ml and 0.15 μg/ml respectively. Kanamycin PK parameters were described and there was no significant difference between HIV-positive and HIV-negative patients. A statistical significant difference (p=0.0126) was found in the renal function in HIV - positive and HIV - negative patients. However, this difference did not affect kanamycin elimination. No interactions have been identified between antiretroviral drugs and kanamycin.
Conclusion: LC-MS analysis method is highly specific and highly sensitive in the detection and quantification of kanamycin plasma concentrations. Kanamycin PK in patients with MDR-TB was described. Due to a limited number of patients, we cannot rule out any influence of HIV - infection, renal impairment and antiretroviral drugs on kanamycin pharmacokinetics. The relationship between the area under the curve of kanamycin free plasma concentrations (fAUC) and its minimum inhibitory concentrations (MIC) on M.tuberculosis isolated from the sputum of each patient should be assessed. Therefore, kanamycin free plasma concentrations and MIC should be determined
<Keywords: Multi-drug resistant tuberculosis; Human immunodeficiency virus; Liquid Chromatography-Mass Spectrometry; Plasma concentrations; Pharmacokinetics; Kanamycin
The surge of multidrug- resistant tuberculosis (MDR-TB) is raising concerns globally and in sub-Saharan Africa [1-6]. Although the epidemiological relationship between HIV infection and MDR-TB has not been established in sub- Saharan Africa [7-10], clinical evidence has shown that there is a link between HIV infection and the development of MDR-TB [11-14].
Many studies have confirmed that HIV -positive patients do not adequately absorb anti-TB drugs resulting in sub-therapeutic outcomes of anti-TB therapy that may result in the development of resistance to anti-TB drugs [12,13,15]. This evidence has not yet been confirmed for many of the second-line anti-TB drugs.
Interactions between anti-retroviral drugs and anti-TB drugs alter the plasma concentrations of anti-TB drugs and these interactions could result in sub-therapeutic anti-TB drugs plasma concentrations. For first-line anti-TB drugs, major drug/drug interactions occur between rifampicin (RIF) and highly active anti-retroviral therapy (HAART) drugs, protease inhibitors (PIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs) [16,17]. Furthermore, interaction between tenofovir and kanamycin as a result of reduced elimination by the kidney could result in an increase in the plasma concentration of kanamycin.
Consequently, a better understanding of the pharmacokinetics (PK) and pharmacodynamics (PD) of anti-TB drugs should improve treatment outcomes in patients with MDR-TB infection and in patients with MDR-TB co-infected with HIV [18].
Kanamycin is one of the drugs used in the intensive phase treatment of MDR-TB. The PK of kanamycin has been studied in healthy volunteers using microbiological assay methods and to a limited extent in patients with MDR-TB [19,20]. To the best of our knowledge, there is no recently published study on the analysis of kanamycin plasma concentrations using liquid chromatography coupled with mass spectrometry (LC-MS). In addition, little information exists on the PK of kanamycin in HIV -negative patients infected with MDR TB [21], and currently there is no information on its PK in South African patients with MDR-TB infection and in patients with MDRTB co-infected with HIV [22]. Therefore, information obtained from this study might help for future development of therapeutic drug monitoring (TDM) in order to improve patients’ treatment outcome and optimise drug therapy.
Hence, we determined kanamycin plasma concentrations using LC-MS and evaluated the PK of kanamycin in patients with MDRTB and in patients with MDR-TB co-infected with HIV during their course of treatment. We also examined the influence of HIV infection on kanamycin PK. We evaluated the effect of the kidney dysfunction on kanamycin PK and assessed the interaction between antiretroviral drugs and kanamycin.
Study site, design and subjects
The study was conducted at Brewelskloof Hospital (BKH), South Africa. BKH is one of the South African hospitals specialized in the treatment of MDR-TB. The study was designed as a prospective, non randomized pharmacokinetic study involving male and female HIVpositive and HIV-negative patients admitted for MDR-TB treatment.
Inclusion and exclusion criteria
A patient was included in the study if he/she complied with all of the following: (1) Signature of informed written consent; (2) Informed consent for HIV test; (3) On kanamycin treatment for at least 2 weeks; (4) Adult patients 18 - 65 years old; (5) MDR-TB sensitive to second - line anti-TB drugs.
Patients were excluded from the study in case any of the following criteria applied: (1) Patient request; (2) History of congestive cardiac failure; (3) Uncontrolled hypertension; (4) Ischemic heart disease; (5) Pregnancy or breast feeding; (6) Hypersensitivity to kanamycin; (7) Patients on drugs other than anti-retroviral drugs, known to interact with kanamycin; (8) Older than 65 years and younger than 18 years; (9) Haemoglobin less than 10g%, and (10) severe dehydration
Kanamycin dose and blood sampling
Patients received kanamycin at a dose of 500, 600, 660, 750, 1000 mg daily based on their body weight. On the study day, after an 8-hour overnight fast, blood samples were collected in a heparinised tube via an intravenous catheter fixed on the forearm vein before (baseline) and ½, 1, 2, 4, 8 and 24 hours after intramuscular administration of kanamycin. Blood samples were immediately centrifuged at 5,250 rpm for 5 minutes. Then, plasma was separated and stored at -80ºC until the day of analysis. Blood was also collected for renal and liver function tests, CD4 counts, viral load and haematology tests.
Determination of kanamycin plasma concentrations and chemicals used
Plasma levels of kanamycin were determined using LC-MS. The following chemicals were used in the study: analytical grade dimethyl sulfoxide (DMSO), acetonitrile (ACN), trichloroacetic acid (TCA), phosphoric acid and HPLC grade trifluroacetic acid (TFA). All of them were obtained from Sigma-Aldrich (Cape Town, Western Cape). Kanamycin was supplied by BKH and used as a working standard.
Liquid Chromatography-Mass Spectrometry
LC-MS was performed with Waters Acquity UPLC system connected to a Xevo triple quadrupole mass spectrometer (Waters, Milford, MA, USA). The Waters Atlantis is a reversed phase packing with a difunctional C18 ligand, designed to retain polar compounds better. The mobile phase used was 1 % formic acid in water (v/v) as solvent A, solvent B consisted of acetonitrile. A flow rate of 0.23 ml/ min was applied and an injection volume of 5 μl. The gradient started at 98% solvent A for the first 2 minutes followed by a linear gradient over 8 minutes to 70 % solvent B. The column was washed for 1 minute at 100% solvent B and re-equilibrated for another 6 minutes at the starting conditions.
The MS conditions were as follows: electrospray ionization in the positive mode was applied, the ion source and desolvation temperature were held at 140 ºC and 400 ºC, respectively. The capillary voltage was 2.8 kV. The desolvation gas at 1000 L/h and the cone gas was 50 L/h. The instrument was operated at multiple reactions monitoring (MRM) mode. The MRM settings for kanamycin was 485 > 163 at collision energy 20 eV.and cone voltage of 20 V. Propanolol was used as internal standard and was monitored at an MRM of 260.3 >183 at a collision energy of 20eV and cone voltage of 18 V. Waters MassLynx™ software was used for the data collection and processing.
Preparation of standards
The stock solution of 1 mg/ml was serially diluted with acetonitrile to obtain working solutions with the concentrations 10, 5, 1, 0.5, 0.1, 0.05 and 0.01μg/ml. All these standards contained 10 ppm propanolol as internal standard.
Patient samples preparation
To prepare the patients’ plasma samples for the LC-MS assay, trichloroacetic acid (30 μl) was added to 50 μl plasma followed by 170 μl internal standard solution (10 ppm propanolol in water). The mixture was vortexed for 1 minute, followed by centrifugation at 6000 g for 5 minutes. The supernatant was injected onto the LC-MS. Blank plasma was spiked with 1 and 5 ppm of kanamycin in triplicate to determine the recoveries and repeatability. The relative standard deviation was better than 12%. This relatively high standard deviation and relatively high limit of detection and quantification is due to the fact that kanamycin elutes just after the void volume of the column. The use of a C18 column with similar selectivity as the Waters Atlantis column used here is very important for this analysis.
Determination of pharmacokinetic parameters
The plasma concentration-time profile for each patient was plotted using a semi-log graph paper. Kanamycin PK parameters were calculated based on the non-compartmental analysis [22-24] and expressed as median and range (lowest to highest).
Statistical analysis
Patients’ data were organised and coded onto data collection forms and captured into Microsoft Excel spreadsheets. Kanamycin concentrations and PK parameters were analysed using descriptive statistics. Analysis was done using SAS version 9.0 (SAS Institute Inc., Cary, NC, USA).
Since the data is highly skewed in many cases, the HIV+ and HIVgroups were compared using the Wilcoxon Rank Sum test rather than a t-test. PK parameters were reported as mean and standard deviation. The Kruskal-Wallis one-way analysis of variance was used in comparing more than two groups to see if they originate from the same population. Statistical significance was assumed at the p < 0.01 level to avoid a type 1 error (false positive).
The number of patients in HIV-positive and HIV-negative groups was sufficient to give a power of about 80% in detecting a statistical significant difference in the means of about 1.2 standard deviations based on our power calculations. Also, the number of patients who participated in previously published studies [21,25-28] was similar to the number of patients in our study.
Ethics consideration
The study was approved by the ethics committee of the University of the Western Cape and the University of Cape Town. Permission to conduct the study was granted by the Western Cape Department of Health. It was conducted according to the national and international ethics requirements. The information collected was kept confidential and saved in a safe file which can only be accessed by the researcher. Patient confidentiality and privacy was maintained at all times.
Patients’ demographic data
Thirty-one patients (17 males and 14 females) infected with MDRTB participated in the study. Of these 31 patients, 13 (8 males and 5 females) were infected with HIV. The median (range) age and weight of patients were 32 (18–54) years and 53.0 (41.8–90.0) kg, respectively.
Renal and liver function profile
The renal function was normal in 5 HIV (+) and 15 HIV (-) patients, mildly impaired (60-89 GFR) in 6 HIV (+) and 3 HIV (-) patients, moderately impaired (40-59 GFR) in 2 HIV (+) patients. Liver function tests were normal in both HIV (+) and HIV (-) patients.
Virological profile
In HIV (+) patients the CD4 count (cells/mm3) was <100 in 5 patients, 100-299 in 3 patients and > 300 in 5 patients. The viral load was less than 40 copies/ml in 10 patients and 5,000 to 1,000,000 copies/ ml in 3patients.
Validation of the method of kanamycin liquid chromatography-mass spectrometry analysis
Liquid chromatography coupled with mass spectrometry was used in the quantification of kanamycin plasma concentrations. This method was validated by determining linearity, recovery, precision and accuracy, low limit of detection, low limit of quantification, and specificity.
The overall precision expressed as relative standard deviation (RSD %), was less than 12%. The accuracy, expressed in terms of recovery was 74 ± 9.1% and 111 ± 6.2% for 1 μg/ml and 5 μg/ml, respectively.
The lower limit of detection of kanamycin was 0.06 μg/ml. The lower limit of quantification of kanamycin in the plasma was 0.15 μg/ ml.
There were no interfering peaks from the plasma components with kanamycin peak in the blank plasma, which was detected at a retention time of 2.65 minutes. Figure 1 shows the chromatograms of kanamycin and internal standard of a patient’s plasma. This relatively high standard deviation and relatively high limit of detection and quantitation is due to the fact that kanamycin elutes just after the void volume of the column. The use of a very polar C18 column is very important for this analysis as most other columns and solvent systems tested were unable to retain kanamycin.
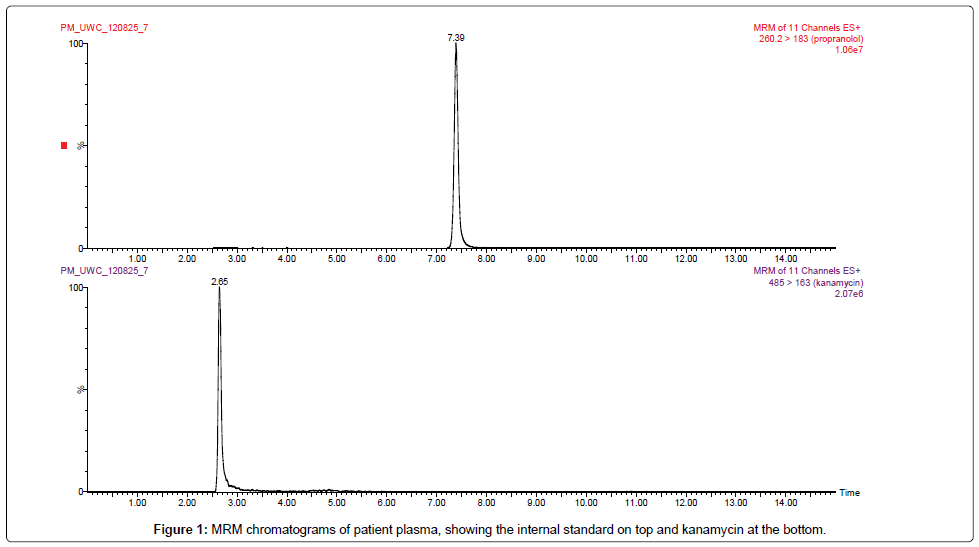
Figure 1: MRM chromatograms of patient plasma, showing the internal standard on top and kanamycin at the bottom.
Kanamycin pharmacokinetic parameters
Table 1 and Figure 2 present kanamycin mean plasma concentrations in HIV-negative and HIV-positive patients at different times of blood sampling as indicated in the methods. The standard deviations (STD) and P-values between HIV-negative and HIV–positive are also shown. Before kanamycin administration there were no detectable plasma concentrations from previous day kanamycin administration in both HIV - positive and HIV - negative patients. However, 24 hours after current study kanamycin dosing, the mean plasma concentrations we 1.27 ± 2.89 μg/ml in HIV (+) and 0.97 ± 2.54 μg/ml in HIV (-) patients.
| Time | HIV - NEG (N=18) | HIV - POS (N=13) | P-value | ||
|---|---|---|---|---|---|
| (hr) | Mean (µg/ml) | STD | Mean (µg/ml) | STD | |
| t0 | 0.00 | 0 | 0.00 | 0 | 1 |
| t0.5 | 1.94 | 3.83 | 3.83 | 5.27 | 0.3472 |
| t1 | 16.43 | 5.63 | 15.94 | 7.47 | 0.9447 |
| t2 | 14.33 | 5.92 | 14.46 | 4.78 | 0.9916 |
| t4 | 9.06 | 3.79 | 9.83 | 3.18 | 0.7004 |
| t8 | 4.96 | 4.13 | 5.64 | 4.14 | 0.4105 |
| t24 | 0.97 | 2.54 | 1.27 | 2.89 | 0.5139 |
Table 1: Kanamycin plasma concentrations in HIV-negative and HIV-positive patients.
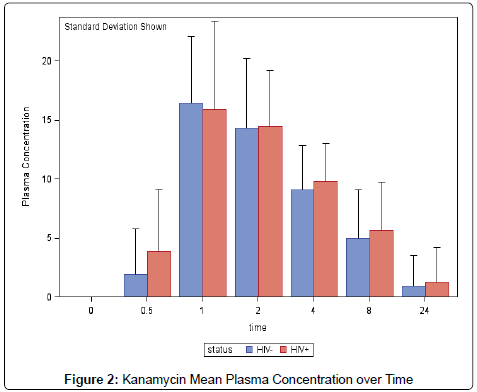
Figure 2: Kanamycin Mean Plasma Concentration over Time
Table 2 and Figures 3-5 present kanamycin pharmacokinetic parameters in HIV-negative and HIV-positive patients. The elimination rate constant (Ke), the elimination half-life (T1/2), the area under the plasma concentration curve during 24 hours (AUC0-24), the area under the plasma concentration curve from zero to infinity (AUC0-∞), the maximum plasma concentrations (Cmax), the time to the maximum plasma concentrations (Tmax), the absorption rate constant (ka), the absorption half-life (t1/2), the volume of distribution (Vd), the total clearance (Cltot), and the mean residence time (MRT) are given in Table 2 in the order at which they appear. Each parameter is shown as mean value plus STD. P-values between HIV (-) and HIV (+) patients are also indicated.
| PK | HIV - NEG (N=18) | HIV - POS (N=13) | P-value | ||
|---|---|---|---|---|---|
| Parameters | Mean (µg/ml) | STD | Mean (µg/ml) | STD | |
| Ke (hr-1) | 0.20 | 0.11 | 0.19 | 0.08 | 0.8205 |
| Tmax (hr) | 1.16 | 0.49 | 1.27 | 0.53 | 0.6159 |
| Ka (hr-1) | 1.29 | 1.32 | 1.05 | 0.88 | 0.8357 |
| t1/2 (hr) | 1.67 | 1.86 | 1.29 | 1.59 | 0.9273 |
| T1/2 (hr) | 4.45 | 2.25 | 4.62 | 2.66 | 0.8205 |
| Cltot (L/hr) | 7.72 | 5.49 | 9.13 | 8.93 | 0.7153 |
| MRT (hr) | 3.99 | 3.01 | 4.16 | 3.56 | 0.7674 |
| Cmax (µg/ml) | 18 | 4.69 | 16.35 | 5.76 | 0.4892 |
| Vd (L) | 38.62 | 18.56 | 50.18 | 45.34 | 0.7078 |
| AUC0-24 (µg/ml.hr) | 122.53 | 58.58 | 122.89 | 77.94 | 0.6217 |
| AUC0-∞ (µg/ml.hr) | 170.26 | 91.37 | 169.08 | 115.32 | 0.5669 |
Table 2: Kanamycin PK parameters in HIV-negative andHIVpositive patients.
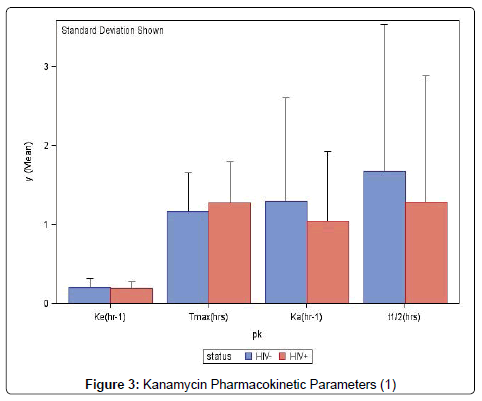
Figure 3: Kanamycin Pharmacokinetic Parameters (1)
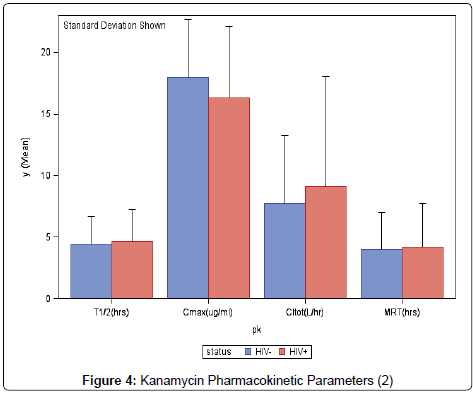
Figure 4: Kanamycin Pharmacokinetic Parameters (2)
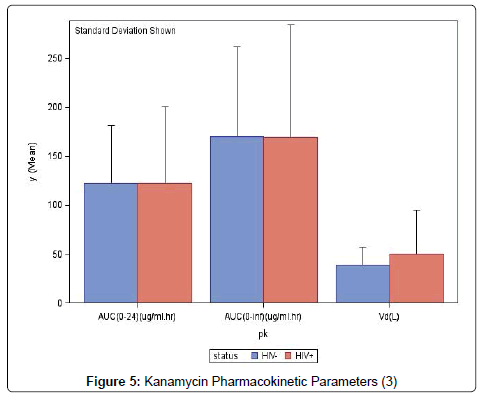
Figure 5: Kanamycin Pharmacokinetic Parameters (3)
Determination of kanamycin plasma concentrations using liquid chromatography-mass spectrometry
The LC-MS method is a proven method and has been widely used in the quantification of anti-TB drugs [22-24]. The plasma levels of kanamycin were determined using LC-MS method and analysis was conducted according to scientific standards. The linearity, lowest limit of detection, lowest limit of quantification, specificity, precision, recovery and accuracy were conducted to validate the assay. All chemicals used were prepared and standardised regularly. Chemicals were obtained from a reputable source (Sigma-Aldrich, Cape Town). Separation of kanamycin was achieved at a retention time of 1.50 minutes with a high recovery percentage of 92.5%.
Previously published studies have used microbiological and fluoroimmunoassay in the quantification of kanamycin [21,25-28]. This study results demonstrate that the LC-MS analysis method is highly successful and accurate in the detection and quantification of kanamycin concentrations in plasma.
At baseline kanamycin plasma concentrations were below detectable levels (0.05 μg/ml). This could be as a result of an insufficient amount of kanamycin remaining in the body 24hrs after previous dosing that could be detected at baseline.
Kanamycin pharmacokinetics
Kanamycin PK parameters have been described in 3 studies in healthy volunteers [25,26,28] and in one study involving HIV -negative patients infected with MDR-TB [21] using immunoassay methods. Cmax , Tmax , Ke , T1/2 , Cltot and Vd results of these studies range from 20 to 35 μg/ml, 1 to 2 hours, 0.29 to 0.30 hr-1, 2 to 4 hours, 5 to 6 L/hr and 17–23 L respectively [21,25,26,28].
When comparing kanamycin PK parameters in previous studies to that of HIV -negative patients in the study, the mean Cmax (18.39 μg/ ml) was lower, Tmax (1hr) was similar, Ke (0.13hr-1) was lower, T1/2 (5.37 hrs) was longer, Cltot (4.00L/hr) was higher and Vd (33.02L) was higher. The increased Vd kanamycin could be responsible for the long time kanamycin molecules resided in HIV-negative patients [20,25,26,28].
Influence of human immunodeficiency virus on the pharmacokinetics of kanamycin
The rate and extent of absorption of kanamycin as represented by the Tmax and Cmax were similar in both HIV -positive and HIV -negative patients. The AUC0-24, which quantifies the extent of absorption of kanamycin was also similar in HIV -positive and HIV -negative patients. HIV -positive patients were not severely affected by HIV. Many HIV positive patients had good immunological and virological profile. Eight out of thirteen patients had a CD4 count within the ranges of (100-599) cells/mm3 and ten had a viral load of less than 40 copies/ml.
When compared to other HIV -positive patients in the study, a reduction in the extent of distribution of kanamycin in two patients with CD4 count of 382 and 336 cells/mm3 and represented by a Vd of 13.28 and 15.39 L, respectively, might be associated with the short elimination T1/2 of 2.10 and 3.15 hours and MRT of 2.39 and 2.87 hrs, respectively that was observed. The T1/2 of a drug is a PK parameter dependent on both Vd and CLtot and is a reflection of the extent of the distribution or elimination of a drug [29-32]. Similarly, an increase in the Vd (60.22, 51.92, 26.26 and 30.17 L) of kanamycin in some patients as compared to other HIV -positive patients resulted in the lengthening of the elimination T1/2 of 6.30, 8.77, 11.00 and 5.33 hrs and MRT of 7.92, 8.80, 12.96 and 4.69 hrs, respectively.
There were no significant differences in the PK parameters of kanamycin in HIV -positive patients when compared to the mean PK parameters in HIV -negative patients. The smallest observed p-value is about 0.48 However, it should be remembered that the sample sizes are relatively small so that there is limited power to detect differences. Differences may in fact exist but could not be detected statistically.
Influence of renal dysfunction on the pharmacokinetics of kanamycin:
There was a significant difference (p=0.013) in the renal function between the HIV -positive and HIV -negative patients. However there was no significant difference (p=0.31) when we correlated the GFR values and the PK parameters in the two groups of patients to see if changes in the renal function affected the PK of kanamycin. HIV could be responsible for the significant difference in the renal function between HIV -positive and HIV -negative patients. A decline in renal function and low CD4 count are associated with HIV-related nephropathy, due to HIV infecting the renal cells directly [33-35]. Also, we had more patients with impaired renal function in the HIV -positive group than in the HIV -negative group and this could have contributed to the statistical difference. This result is consistent with a study done in South African patients, reporting that HIV-related nephropathy is exhibited in HIV positive patients at any stage of HIV infection and is characterised with varying degrees of GFR [33].
Influence of antiretroviral drugs on the pharmacokinetics of kanamycin?
Kanamycin was administered with other MDR-TB drugs to all patients. Some of the HIV positive patients were also given lamivudine, stavudine and efavirenz. None of these drugs affected the metabolism, distribution and renal elimination of kanamycin.
Therapeutic implications
The two common PK parameters associated with the clinical efficacy of aminoglycosides are Cmax and AUC0-24 [36]. High peak plasma concentration of aminoglycosides is associated with increased rate of elimination of Mycobacterium tuberculosis (MTB) and better therapeutic response in patients [4,12]. However, due to the narrow therapeutic range (20-35) μg/ml of aminoglycosides [12], care must be taken when administering kanamycin in patients with renal impairment.
Kanamycin shows inhibitory activity against MTB at concentration of about 6 μg/ml in vitro and an intramuscular dose of 15 mg/kg produces a Cmax of 35-45 μg/ml [4,12]. Most of our patients had a low peak plasma concentration of kanamycin when compared to the literature [25-28]. A median dose of 18.9 mg/kg of kanamycin in both HIV -positive and HIV –negative patients in the study resulted in a peak plasma level of 18.19 (8.40-27.63) μg/ml and 18.39 (13.32- 25.26) μg/ml, respectively. The low Cmax could result in poor response to therapy and increased risk of selection of drug-resistant organisms. This is because kanamycin has a concentration-dependent bactericidal activity as the rate of bacterial killing increases as the concentration increases [37-40]. In addition, the Cmax: MIC ratio correlates best with bacterial killing and it is important to have a high Cmax: MIC ratio of at least 8–10 to prevent resistance for aminoglycosides [40,41]. Therefore, the ideal dosing regimen of kanamycin would maximise concentration, because the higher the concentration, the higher the extent of bacterial killing [40].
It has been suggested that clinicians should aim for a Cmax of between 20 and 35 μg/ml to maximise the rate and extent of bacterial killing and a Ctrough (trough level) of <10 μg/ml to prevent toxicity when kanamycin is given intramuscularly [12]. Based on our results, the mean Ctrough of kanamycin in HIV -positive and in HIV -negative patients was 1.27 ± 2.89 μg/ml and 0.97 ± 2.54 μg/ml respectively. This explains that kanamycin plasma levels were not toxic in our patients.
Furthermore, a high Cmax: MIC ratio suggests a persistent prolonged period of bacterial growth inhibition after exposure to aminoglycosides. Clinically, the post antibiotic effect (PAE) for aminoglycosides is usually between 2 and 4 hours [42]. The PAE of aminoglycosides suppresses bacterial regrowth when serum concentrations are below the MIC [42,43].
We had an unequal distribution of patients in the HIV-positive and HIV-negative groups. Thirty-one patients volunteered to participate in the study, of which 13 were HIV-positive. Also, there were very few patients with kidney dysfunction and no drug–drug interaction was observed between kanamycin and co-administered medications.
There was no balance in the CD4 count and viral load in HIVpositive patients. Five patients had a CD4 count of <100 cells/mm3 and eight had a CD4 count of >100 cells/mm3. Some patients were in the early stage of the disease, while some had advanced HIV infection. In addition, studies on the PK of kanamycin are very scarce, especially in sub-Saharan Africa. Thus, comparison of our results with previously published studies for similarities or differences in the PK parameters was limited. Future studies involving more volunteers are needed.
Based on the results obtained, we can conclude that objectives of the present study were achieved.
The LC-MS analysis method is highly specific and highly sensitive in the detection and quantification of the plasma concentrations of kanamycin. The PK of kanamycin in patients with MDR-TB and in those with MDR-TB co-infected with HIV was described. Furthermore, HIV infection does not have any influence on the PK of kanamycin. Finally, changes in renal function do not influence the PK of kanamycin.
Based on the results of this study, the following should be considered for future studies.
Kanamycin-free plasma concentrations should be evaluated, in order to determine the AUC of the free plasma concentrations (fAUC) which, together with the MIC will be used to determine the relationship between fAUC and MIC of kanamycin.
Therefore, the MIC of kanamycin on M.tuberculosis isolated from the sputum of each patient should be determined.
PK/PD relationship of kanamycin should be determined, because it quantifies the activity of an antibiotic and describes the time course of action of the antibiotic.
The following people and departments are acknowledged:
The medical superintendent at Brewelskloof Hospital for permission to conduct the study.
Staff members at Brewelskloof Hospital for their support.
The Pharmaceutical Services, Provincial Administration of the Western Cape for supplying anti-tuberculosis tablets.
The Department of Health, Province of the Western Cape for the permission to conduct the study at Brewelskloof Hospital.
Patients who participated in the study.
The research department, University of the Western Cape for financial support of the study.
The Medical Research Council for financial support of the study.