Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Mini Review - (2015) Volume 3, Issue 3
It is generally accepted that dental pulp plays important roles in maintaining tooth. Pulp inflammation caused by dental caries or tooth fracture sometimes results in a severe pain, and pulpectomy to remove entire dental pulp is often performed by dentists to release a patient from the pain. After pulpectomy, the tooth without vital pulp loses its defensive ability and becomes vulnerable to exogenous stimuli. It will be valuable to establish a local regeneration therapy of dentin-pulp complex from residual dental pulp before pulpectomy to preserve abilities of dental pulp. We are trying to develop a novel therapy to induce regeneration of dentin-pulp complex following pulp amputation. In this approach, growth factors and a scaffold are exogenously supplied, while cells and blood vessels are induced from the residual dental pulp in the tooth root canal. Establishment of a newly method for pulp amputation without leading necrosis of the residual root pulp is also essential for the local regeneration therapy of dentin-pulp complex. In this mini review, we show our research strategy for local regeneration therapy of dentin-pulp complex.
Keywords: Dentin-pulp complex, Pulp amputation, Regeneration therapy
Dental pulp, which is surrounded by hard tissue (dentin and enamel), consists of pulp cells, odontoblasts, endothelial cells, neurons, immune system cells, and the extracellular matrix, and plays key roles in maintaining the function of healthy teeth [1]. Via the apical foramen of tooth, blood vessels supply nutrients to the tooth and remove waste products, and neural network warns for harmful stimuli as pain [2]. Immune system cells including dendritic cells, macrophages, and T-lymphocytes, prevent entry of microorganisms and other foreign antigens [2]. Pulp cells and odontoblasts repair dentin that has been lost due to tooth wear or dental caries, by depositing tertiary dentin on the pulp chamber surface as a protective physical barrier in order to block exogenous stimuli [2].
Once the inflammatory response in dental pulp is triggered by stimulation such as severe infection, the internal pressure in the pulp chamber significantly elevates, resulting in severe pain for patients and pulp tissue ischemia [2]. To release patients from the pain, dentists eventually remove an entire pulp by pulpectomy [3]. If pulpectomy is not performed, ischemia develops due to impaired blood circulation, resulting in pulp necrosis [4].
Non-vital tooth becomes vulnerable to exogenous stimuli due to complete loss of perception and immune functions, and weak due to loss of metabolic capacity [3]. Further, non-vital tooth is often re-infected by bacteria. The success rate of root canal retreatment is not particularly high [5-8], and it is often necessary to repeat root canal treatment. Repetition of root canal treatment leads to cracking and/or fracture of the root. As a result, the weakening of the tooth leads to tooth extraction.
To keep sound teeth during entire life of patients, the development of novel therapies for preservation and regeneration of dental pulp are essential.
Problems of present pulp amputation
To avoid pulpectomy, we aim to establish local regeneration therapy of the dentin-pulp complex from residual dental pulp following “pulp amputation”. Pulp amputation in the current dental treatment is as follows; after the removal of damaged coronal pulp tissue and the irrigation of the root canal orifice with chemical reagents, calcium hydroxide-based materials or mineral trioxide aggregate are applied to the root canal orifice in order to promote formation of dentin bridge for the preservation of root pulp [3,9-11] (Figure 1A). However, necrotic tissue layer remains at an interface between the residual root pulp and the dentin bridge after the pulp amputation [3]. It is also known that the newly formed dentin bridge by pulp amputation is porous hard tissue with a low degree of calcification, thus they have poor ability to protect the residual root pulp [12]. Most important issue is that pulp amputation itself never leads to the regeneration of pulp or dentin that was lost in the coronal portion.
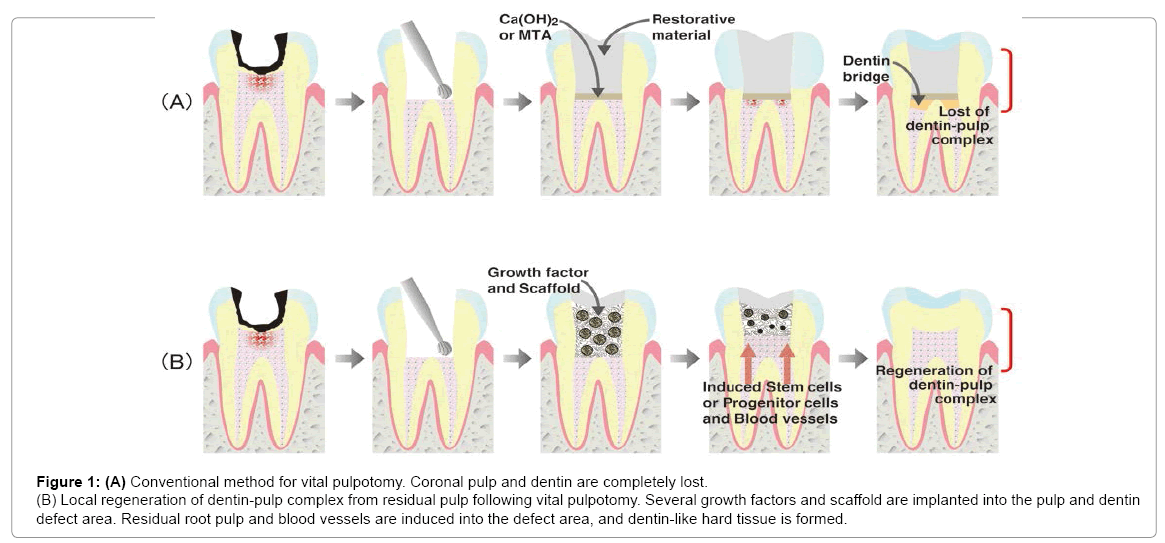
Figure 1: (A) Conventional method for vital pulpotomy. Coronal pulp and dentin are completely lost.
(B) Local regeneration of dentin-pulp complex from residual pulp following vital pulpotomy. Several growth factors and scaffold are implanted into the pulp and dentin defect area. Residual root pulp and blood vessels are induced into the defect area, and dentin-like hard tissue is formed.
Novel strategy for the local regeneration of dentin-pulp complex following pulp amputation
Our strategy for the local regeneration of dentin-pulp complex is to induce outgrowth of pulp cells, capillaries, and neurons from the residual root pulp with the modification of the current therapy (Figure 1B). It is well known that three factors are considered to be essential for tissue regeneration; cell, growth factor, and scaffold [13]. For successful regeneration, it is also necessary to induce a capillary network and a closed space that will create a suitable environment [14]. In the development of the dentin-pulp complex regeneration therapy following pulp amputation, it is possible to induce dental pulp stem cells (or pulp progenitor cells), which can differentiate into odontoblasts producing newly dentin, and capillaries from the residual root pulp tissue. Also, a closed space for tissue regeneration can be secured by application of temporary sealing with adhesive materials that are already used in the clinic. For the establishment of local regeneration of dentin-pulp complex, the choice of an appropriate growth factor, appropriate delivery system of a growth factor, and a scaffold to induce stem cells and blood vessels from the residual pulp are critical points.
Candidate growth factor for regeneration of dental pulp
Fibroblast growth factor-2 (FGF-2) plays an important role in physiologic conditions of odontogenesis [15-17], as well as pathologic conditions [18-20]. We focused on the potency of FGF-2 and chose it as the growth factor for local regeneration therapy of the dentin-pulp complex.
Delivery system of growth factors to the local tissue site is one of important factors for the regeneration. In vivo, growth factors usually effects for a certain period at low concentrations. If the growth factors are administered by directly injection in the pulp chamber, they rapidly lose their biological activities due to diffusion and degradation, and their effects are eliminated. To overcome this problem, we focused on a gelatin hydrogel incorporating FGF-2. It was previously demonstrated that a gradual and continual release of FGF-2 was achieved by in vivo biodegradation of gelatin hydrogels that incorporated FGF-2 [21-24]. Furthermore, the controlled release of FGF-2 from gelatin hydrogels induced regeneration of angiogenesis [25], bone [26-28], periodontal tissues [29], and other tissues [30-32].
To clarify whether FGF-2-incorporated gelatin hydrogel induces dentin-pulp complex regeneration, we implanted them with collagen sponge scaffold into the coronal pulp chamber of the rat first molar after pulp amputation. We found that controlled release of FGF-2 from gelatin hydrogel induced regeneration of pulp tissue and osteo-dentin like hard tissue at the defect area, demonstrating the efficacy of FGF-2- incorpotated gelatin hydrogel [33,34].
Suitable scaffold for dentin-pulp complex regeneration therapy
In our in vivo study, we used collagen sponge as scaffold and it did not show negative effects on the local regeneration of dentin-pulp complex. However, no studies had confirmed which scaffold materials were suitable for dentin-pulp complex regeneration in pulp chamber. We sought a suitable scaffold for the therapy and focused on the potential of hyaluronic acid (HA). HA is one of glycosaminoglycans that are widely distributed in human body. It plays important roles in maintaining morphologic organization by preserving extracellular spaces and is reported to be well suited for tissue engineering material [35-39]. Further, HA was reported to suppress production of proinflammatory cytokines such as interleukin-1 and tumor necrosis factor-alpha by activated macrophages [40,41]. Based on these superior properties, HA is extensively used in the fields of health care and cosmetics today.
To clarify whether HA sponge is useful as a scaffold for dentin-pulp complex regeneration therapy, we carried out in vitro and in vivo studies. In vitro study, odontoblast-like cells (KN-3 cells) established from the incisors of 7-day-old rats were used [42,43], and found that KN-3 cells adhered to HA sponge. In vivo study, implantation of HA or collagen sponges in pulp and dentin defect areas following pulp amputation, showed that pulp tissue regeneration was induced into tissue defect, while inflammatory cell invasion in HA sponge implantation area was significantly less compared with collagen sponge [44]. These results suggest that HA sponge has an ideal property as a scaffold for dental pulp regeneration.
These studies suggest the feasibility of the local regeneration therapy following pulp amputation using existing agents and materials. However, for the clinical application of this therapy, we have to establish new techniques for pulp amputation without necrosis of the root pulp, as well as the combination of FGF-2 with other factors to induce regenerated dentin with proper quantity and quality.
In a tooth targeted for pulp amputation, coronal dental pulp is in an inflammatory state because of dental caries and/or trauma. Amputation of coronal vital pulp will cause an additional severe stimulation of root pulp, resulting in necrosis of the remaining root pulp. A critical point to avoid necrosis is how to regulate heat stress and ischemia simultaneously produced by pulp amputation.
Heat stress produced by rotary cutting instruments used to remove infected dental hard tissue is known as one of the most severe exogenous stimuli for dental pulp [2,45]. It is also known that ischemia, caused by inflammation and/or local anesthetics containing a vasoconstrictor [46-48], induces hypoxia and starvation in dental pulp [49,50]. Pulp cells have abilities to resist to heat stress and ischemia [51,52]. We examined the combinatorial effects of these stimuli, and found that the effects of heat stress on dental pulp cells were significantly reinforced by starvation. These results imply that use of vasoconstrictor-free local anesthetic would be beneficial for preserving the root pulp following pulp amputation [53,54].
We have also performed studies aimed to increase the resistance ability of pulp cell to lethal heat stimuli. It is known that fever-range heat stress, the range of 40-42°C, has a beneficial role in various mammalian cells [55-57], and exogenous fever-range heat stress as hyperthermia has been widely used as a physical therapy for various diseases [58]. We hypothesized that the fever-range heat stress for several hours can increase resistance of pulp cells to stimuli. KN-3 cells were pretreated with fever-range heat stress at 41°C for 12 hours, followed by additional lethal heat stress at 49°C for 10 minutes. We found that the cells pre-treated by heat stress survived with odontoblast-like properties after lethal heat stress, and that various heat shock proteins (HSPs) accumulated in the cells [59], and transient cell-cycle arrest was induced by the fever-range heat stress for 12 hours [60]. Accumulation of HSPs and/or cell-cycle arrest is able to induce cellular resistance to various stimuli [61-65]. We are now continuing research to identify the effective methods to induce HSPs accumulation and transient cell-cycle arrest.
Previously we showed that newly dentin was induced on the occlusal side of the regenerated dental pulp through the controlled release of FGF-2 from gelatin hydrogels [34]. However, the induced dentin did not have an ideal structure with dentinal tubules, and its quantity was insufficient for protecting the dental pulp or withstanding bite forces. These weak points should be overcome before clinical application.
Bone morphogenetic protein 2 (BMP-2) is known to induce the differentiation of dental pulp stem cells into odontoblasts [66], and in vivo dentin formation after pulp amputation [67]. BMP-2 is a growth factor to be approved by the US Food and Drug Administration for clinical use such as oral maxillofacial surgery [68]. Our previous study with KN-3 cells showed that BMP-2 induced the expressions of dentin matrix proteins such as dentin sialoprotein and dentin matrix protein-1, markers of the differentiation of odontoblasts [69-71], and that Smad signaling pathway involved in the induction process [72]. Furthermore, we found that platelet-rich plasma (PRP) enhances differentiation of KN-3 cells, as well as alkaline phosphatase activity [73]. PRP is an autologous blood product, and it has been used for wound healing of soft tissue and bone repair as a source of growth factors in several clinical settings such as orthopedic surgery [74-77]. These results suggest that the suitable combination of BMP-2, FGF-2 and PRP may solve the problem in local regeneration of dentin-pulp complex after pulp amputation.
In this mini-review, we show our strategy for the local regeneration therapy of dentin-pulp complex, and critical points to overcome before clinical application of this method with ideal efficacy and safety. We believe that our challenge for the local regeneration therapy of dentinpulp complex would change the current dental treatment to preserve dental pulp.