Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2013) Volume 2, Issue 7
Objective: To study the prevalence and associations of nocturnal hypoxia following surgery in PAP-treated (CPAP or bilevel pressure support) OSA patients.
Patients and Methods: PAP-treated OSA patients presenting for elective surgery (n=38) between August 2007 and October 2008 underwent overnight oximetry monitoring on their prescribed PAP therapy on postoperative night one. The lowest oxygen (O2) saturation (SpO2), time spent with SpO2 <89% and the presence of sleep disordered breathing (saw-tooth oscillations) were determined from the oximetry tracings. Need for supplemental O2, nursing/ respiratory interventions, and complications were recorded. Records were reviewed for the type and duration of surgery and anesthesia, net fluid balance, narcotic / sedative use, demographics and co-morbidities.
Results: Seven of 38 subjects (18.4%) spent at least 30 minutes with SpO2 <90% during the night (hypoxic group=HG) on their prescribed PAP therapy. The severity of baseline OSA (total and supine apnea-hypopnea index), pre-CPAP SpO2 (asleep on diagnostic PSG and awake evening after surgery), net fluid balance, and total IV narcotic dose were associated with the HG. Nursing interventions and addition of O2 were more common in the HG, though other adverse events were not. Review of the oximetry tracings suggested 71% of the HG, and 42% of the non-hypoxic group, had findings of uncontrolled sleep apnea.
Conclusions: Despite the use of prescribed PAP therapy the night following surgery, some OSA patients become hypoxic. Postoperative oximetry monitoring may be indicated in PAP-treated OSA patients undergoing surgery
Keywords: Obstructive sleep apnea; CPAP; Perioperative care; Postoperative complications
AHI: Apnea Hypopnea Index; BPAP: Bilevel Positive Airway Pressure; CPAP: Continuous Positive Airway Pressure; ODI: Oxygen Desaturation Index; OSA: Obstructive Sleep Apnea; O2: Oxygen; PAP: Positive Airway Pressure; CPAP: Continuous Positive Airway Pressure; BPAP: Bilevel Positive Airway Pressure; PSG: Polysomnogram; REM: Rapid Eye Movement; SpO2: Oxygen Saturation Ibrar
The estimated prevalence of Obstructive Sleep Apnea (OSA) is 5% in adults in western countries [1]. The prevalence of OSA in the surgical population is likely similar to that of the general population [2-4]. The majority of these patients are not diagnosed at the time of their presentation [2,3].
Patients with OSA are at increased risk for postoperative adverse events. Both surgery and general anesthesia alter pulmonary function, resulting in hypoxemia that could deteriorate during sleep [5,6]. Residual effects of general anesthesia and neuromuscular relaxants, as well as effects of narcotics and sedatives, may relax the pharyngeal muscles and depress the arousal response, leading to more frequent and prolonged apneas with ensuing hypoxia and hypercapnia [7-9]. Supine positioning, often required following surgery, and REM sleep rebound after the first postoperative night can both worsen sleep apnea [10,11]. All of these factors can translate into worsened postoperative outcomes, often catastrophic, for OSA patients undergoing surgery [12].
Retrospective case control studies have suggested higher rates of myocardial ischemia, arrhythmias, need for respiratory interventions, postoperative atrial fibrillation, encephalopathy / delirium, infections and a longer ICU length of stay in patients with OSA [13-15]. A recent retrospective review of over 6 million orthopedic and general surgeries from the National Inpatient Sample found OSA to be an independent risk factor for perioperative pulmonary complications [16].
The first line treatment of OSA remains CPAP therapy [17]. Limited data suggests that CPAP may be protective in the perioperative setting for patients with OSA. A case series of 14 OSA patients undergoing a variety of surgeries reported no postoperative complications following institution of a policy to use CPAP postoperatively [18]. In a retrospective orthopedic case control study, preoperative CPAP use was suggested to reduce postoperative complications, though the data set was too small for analysis [13]. However, there are concerns that a pressure setting established in a stable outpatient state may not be effective in perioperative environment.
We hypothesized that in OSA patients undergoing elective surgery, PAP (CPAP or bilevel pressure support=BPAP) set at prescribed home settings would not effectively eliminate hypoxia on the first night following surgery.
Subjects and design
This was an observational cohort study conducted at MetroHealth Medical Center (MHMC, Case Western Reserve University), an urban academic tertiary care hospital. Consecutive OSA patients undergoing elective surgery were recruited from the pre-surgical clinic between August 2007 and October 2008. All patients provided informed consent and the study was approved by the MHMC’s Institution Review Board (IRB #07-00732).
Subjects enrolled were required to have polysomnogram (PSG) diagnosed OSA, (an apnea-hypopnea index (AHI) of > 5 events per hour with OSA symptoms), and have been successfully manually titrated on CPAP or BPAP. A successful titration consisted of an AHI 2) > 89% on the best pressure setting. Subjective compliance with CPAP or BPAP prior to surgery was required. Subjects were excluded if they were unable to use their PAP postoperatively (i.e. remained intubated), if they were on supplemental oxygen preoperatively (daytime or nocturnal), if they required >40% FiO2 following surgery, if they were pregnant or if they were unwilling/ unable to consent to the study.
Subjects (n=38) enrolled in the study brought their own PAP units (certified by the hospital engineering department) and interface to the hospital. Following surgery, patients were recovered in the Post Anesthesia Care Unit (PACU) and then transferred to a general surgical floor under the care of the primary surgical service. Subjects were placed on their PAP when ready for sleep and a pulse-oximeter with recording capability (Nellcor N-595®) was placed on the patient’s index finger. Respiratory therapy and nursing personnel verified successful PAP placement and an adequate oximetry recording. Oximetry recordings were obtained between the hours of 2100 and 0615. A minimum of 5 hours of recording time was required (63% had more than 6 hours of recording).
Subjects were monitored throughout the night by nursing under the hospital’s sleep apnea protocol (vitals at 2 hour intervals or more frequently as clinically indicated, monitoring oxygenation). Respiratory therapy and nursing personnel documented if (and what time) the subjects removed their PAP therapy and, if so, they helped to replace the PAP therapy. Unsuccessful attempts were documented (3 subjects spent part of the night off of PAP therapy). The use of supplemental oxygen was also documented (occurred in 5 subjects).
Data collection
Upon completion of the oximetry recording, data was downloaded from the oximeter. Automated analysis included the oxygen desaturation index (4% or >desaturation from baseline events per hour=ODI) and time spent with SpO2 <89% (time off PAP therapy was excluded from analysis). The lowest SpO2 and mean SpO2 were also noted. Manual inspection of the oximetry tracings was performed and low SpO2 readings resulting from artifacts were removed from the analysis.
Waveform tracings were downloaded for review and independently evaluated by 2 Sleep-Boarded Sleep Specialists in a blinded fashion (clinical oximetries were mixed in). Each tracing was categorized as either normal, consistent with cardiopulmonary disease (steady low hypoxic pattern), consistent with sleep apnea (saw-tooth pattern waveforms) or consistent with both cardiopulmonary disease and sleep apnea (elements of both). If disagreements arose, a 3rd Sleep-Boarded Sleep Specialist reviewed the tracing and a consensus was obtained.
Data was abstracted from the electronic medical record for patient demographics, comorbidities, past polysomnography details, anesthesia type, surgery type and duration, postoperative fluid balance, postoperative narcotic and benzodiazepine use, any postoperative complications, and length of stay. Postoperative complications recorded included respiratory complications (new addition of oxygen, intubation, new hypercapnia [pCO2 >45 mm Hg], atelectasis [independent Radiologist report], pneumonia, pulmonary embolism), cardiovascular complications (hypotension, uncontrolled hypertension requiring urgent intervention, chest pain, myocardial infarction, new arrhythmia), transfer to a higher level of care, and general complications (delirium, fever, hypoglycemia, ileus, new anemia).
Statistical analysis
The cohort was divided into 2 groups based on the result of their oximetry recording. The groups included the Hypoxic Group (HG, n=7, 18.4% of the total cohort) and the NonHypoxic Group (NHG, n=31, 81.6% of the total cohort). To be part of the HG, subjects had to spend > 30 minutes of the oximetry recording time, while on PAP therapy, with SpO2 <89%. All subsequent data is presented with subjects categorized into one of these groups. For the purposes of analysis, the 2 subjects on BPAP (one in each group) had their PAP pressure recorded as the expiratory pressure setting.
Data is expressed as mean ± SD or, median with 25th and 75th percentiles or percentages. Comparisons of continuous data were made by Wilcoxon rank sum test or Welch two sample t-test for two group comparisons, Analysis of variance (ANOVA) or Kruskal-Wallis test for multiple group comparisons; and of the proportions by Fisher’s exact test. Statistical analysis was done using statistical software R version 2.5.1 (2007-06-27) (Copyright (C) 2007 The R Foundation for Statistical Computing ISBN 3-900051-07-0). P values
Thirty eight subjects completed the study and 7 (18.4%) of these met the criteria for the Hypoxic Group (HG). Baseline data for the HG and the NonHypoxic Group (NHG) are presented in Table 1. In general, the cohort as a whole was predominantly female, middle-aged and obese with significant rates of co-morbid cardiopulmonary disease. There were no significant differences between the oximetry categorized groups in baseline demographics or co-morbidities.
| Hypoxic Group (N = 7) | NonHypoxic Group (N = 31) | ||||
|---|---|---|---|---|---|
| Median or Percent | 25th, 75thpercentile | Median or Percent | 25th, 75th percentile | P-value | |
| Gender Males Females |
14% 86% |
26% 74% |
1 | ||
| Ethnicity African American Caucasian Hispanic |
29% 71% 0% |
61% 36% 3% |
0.35 | ||
| Age (years old) | 50 | 46, 55 | 50 | 46, 59 | 0.87 |
| BMI (kg/m2) At PSG At Surgery |
39 43 |
36, 42 37, 44 |
39 40 |
34, 44 33, 45 |
0.90 0.58 |
| Past Medical History Arrhythmias CAD CHF Stroke Diabetes Mellitus Hypertension Lung Disease |
0% 0% 0% 0% 57% 71% 71% |
10% 7% 3% 3% 36% 61% 39% |
1 1 1 1 0.40 1 0.21 |
||
Abbreviations: PSG=Polysomnogram, BMI=Body Mass Index, CAD=Coronary Artery Disease, CHF=Congestion Heart Failure
Table 1: Baseline Demographic Data.
Baseline PSG data for the 2 groups is displayed in Table 2. Compared to the NHG, the HG had more severe OSA (AHI 36 vs. 22, p=0.03) and supine OSA (AHI 37 vs. 22, p<0.01), as well as a lower average SpO2 during sleep (93% vs. 95%, p<0.01). Despite this, the CPAP settings and control of OSA by CPAP were similar in the 2 groups. Baseline PAP titration studies were performed further out from the date of surgery in the HG compared to the NHG, though this was not statistically significant.
| Hypoxic Group (N = 7) | NonHypoxic Group (N = 31) | ||||
|---|---|---|---|---|---|
| Median | 25th, 75th percentile | Median | 25th,, 75th, percentile | P-value | |
| Diagnostic PSG AHI Supine AHI REM AHI Average SpO2 (%) Lowest SpO2 (%) |
36 37 43 93 79 |
33, 52 35, 57 33, 51 92, 94 73, 86 |
22 22 40 95 84 |
14, 29 13, 32 15, 67 95, 97 79, 88 |
0.03 <0.01 0.97 <0.01 0.27 |
| CPAP titration PSG* Prescribed CPAP (cm H20) AHI on best PAP setting Average SpO2 (%) Lowest SpO2 (%) |
10 2 94 91 |
9, 13 1, 3 94, 97 90, 92 |
10 1 97 93 |
8, 12 0, 4 96, 98 91, 95 |
0.94 0.61 0.21 0.07 |
| Time from titration PSG to surgery (days) | 627 | 398, 856 | 343 | 74, 812 | 0.24 |
Table 2: Baseline PSG Data.
Data related to the specifics of anesthesia and surgery, as well as sedative and narcotic medication use on the first postoperative night are shown in Table 3. There were no significant differences between the 2 groups in the anesthesia delivery method, type of surgery, duration of surgery, or time of day of the surgery. Subjects in the HG had a more positive net fluid balance on the day of surgery (2.9 liters vs. 2.2 liters, p=0.03) and received more narcotics on the day of surgery / first postoperative night (morphine equivalent dose of 63 mg vs. 41 mg, p=0.04) compared to the NHG.
| Hypoxic Group (N = 7) | NonHypoxic Group (N = 31) | ||||
|---|---|---|---|---|---|
| Median or Percent | 25th, 75th percentile | Median or Percent | 25th, 75thpercentile | P-value | |
| Preoperative SpO2 (%) | 97 | 96, 98 | 98 | 96, 99 | 0.14 |
| Anesthesia Type of anesthesia General Conscious sedation Spinal Benzodiazepine dose (Midazolam IV mg) Anesthesia finish time Morning Afternoon Evening |
86% 0% 14% 2 43% 57% 0% |
2, 3.5 |
87% 10% 3% 2 39% 55% 6% |
2, 2 |
0.40 0.40 1 |
| Surgery Type of surgery Head & Neck Upper Abdomen Lower Abdomen Limb Lumbar Spine Skin Length of Surgery < 2 hours 2 – 6 hours > 6 hours |
0% 57% 14% 14% 14% 0% 14% 86% 0% |
7% 29% 29% 29% 3% 3% 42% 55% 3% |
0.54
0.32 |
||
| Net Fluid Balance (liters) (From OR till midnight on the general ward) | 2.9 | 2.6, 3.85 | 2.2 | 1.55, 2.65 | 0.03 |
| Morphine Equivalent Dose (MEQ) (From OR till oximetry completion) Total IV MEQ dose (mg) Total PO MEQ dose (mg) |
63 0 |
52, 67 0,10 |
41 4.5 |
31, 54 0,35 |
0.03 0.21 |
| Benzodiazepine Use (General ward post-operative night 1) IV Benzodiazepine (%) PO Benzodiazepine (%) |
14% 0% |
0% 10% |
0.18 1 |
||
Table 3: Anesthesia, Surgery and Postoperative Night 1 Data.
Table 4 displays the data from the first night following surgery for both groups. The baseline pre-PAP SpO2 was lower in the HG group, though still in the normal range (95% vs. 97%, p=0.02). From the oximetry, the HG had a lower average SpO2 (89% vs. 95%, p<0.01), lower average nadir SpO2 (77% vs. 89%, p< 0.01) and higher ODI (19 vs. 1, p< 0.01). Figure 1 shows the lowest SpO2 encountered for each subject on their diagnostic PSG, on their titration PSG on the chosen CPAP setting, and on the oximetry postoperative night 1 on that same CPAP setting. While the HG required more nursing intervention/use of supplemental oxygen than the NHG, the rates of other complications was similar with the exception of more atelectasis noted in the HG.
| Hypoxic Group (N = 7) | NonHypoxic Group (N = 31) | ||||
|---|---|---|---|---|---|
| Median or Percent | 25th, 75th percentile | Median or Percent | 25th, 75th percentile | P-value | |
| Pre-CPAP Average SpO2 (%) (On ward, prior to CPAP ) |
95 |
94, 96 |
97 |
95, 99 |
0.02 |
| Oximetry Results (On CPAP Ist post-operative night) Time below SpO2 of 89% (minutes) Average SpO2 (%) Lowest SpO2 (%) *Oxygen Desaturation Index (ODI) |
172 89 77 19 |
118, 240 88, 90 75, 80 7, 23 |
0 95 89 1 |
0, 1 93, 97 86, 91 1, 3 |
< 0.01 <0.01 <0.01 <0.01 |
| Postoperative Complications Nursing intervention (adding O2 bleed to CPAP or changing to high-flow O2 mask) O2 added to CPAP (liters per min) Atelectasis **Non-cardiovascular complications ***Cardiovascular complications |
43% 0 29% 57% 0% |
0, 2 | 10% 0 0% 29% 16% |
0, 0 | 0.03 0.01 <0.01 0.20 0.56 |
| Post-operative Day 1 Lowest SpO2 recorded (%) |
92 |
86, 93 |
94 |
86, 95 |
<0.05 |
Table 4: Postoperative Night 1 Oximetry Data.
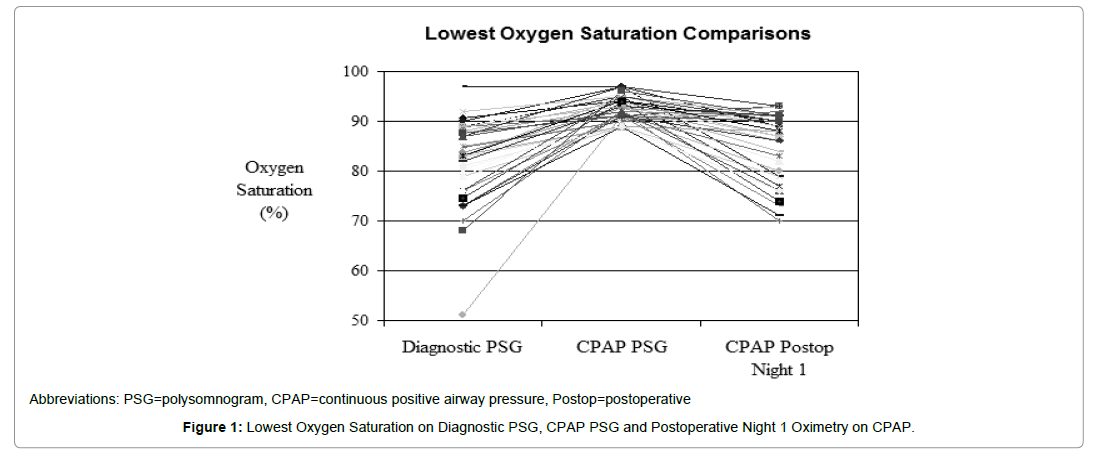
Figure 1: Lowest Oxygen Saturation on Diagnostic PSG, CPAP PSG and Postoperative Night 1 Oximetry on CPAP.
Results of the oximetry interpretations are shown in Figure 2. Those in the HG had more studies interpreted as being consistent with sleep disordered breathing, as well as cardiopulmonary disease, than the NHG. Of note, 42% of the NHG oximetries were interpreted as consistent with uncontrolled sleep apnea. An example of a patient’s oximetry tracings on their diagnostic PSG, on their chosen CPAP setting, and then on postoperative night 1 on the same CPAP setting is displayed in Figure 3. The postoperative oximetry was interpreted as consistent with sleep apnea.
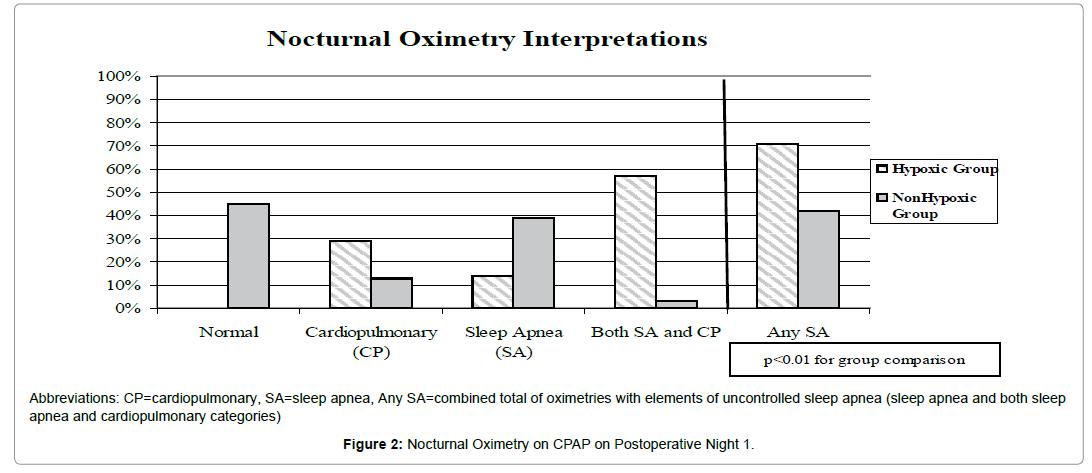
Figure 2: Nocturnal Oximetry on CPAP on Postoperative Night 1.
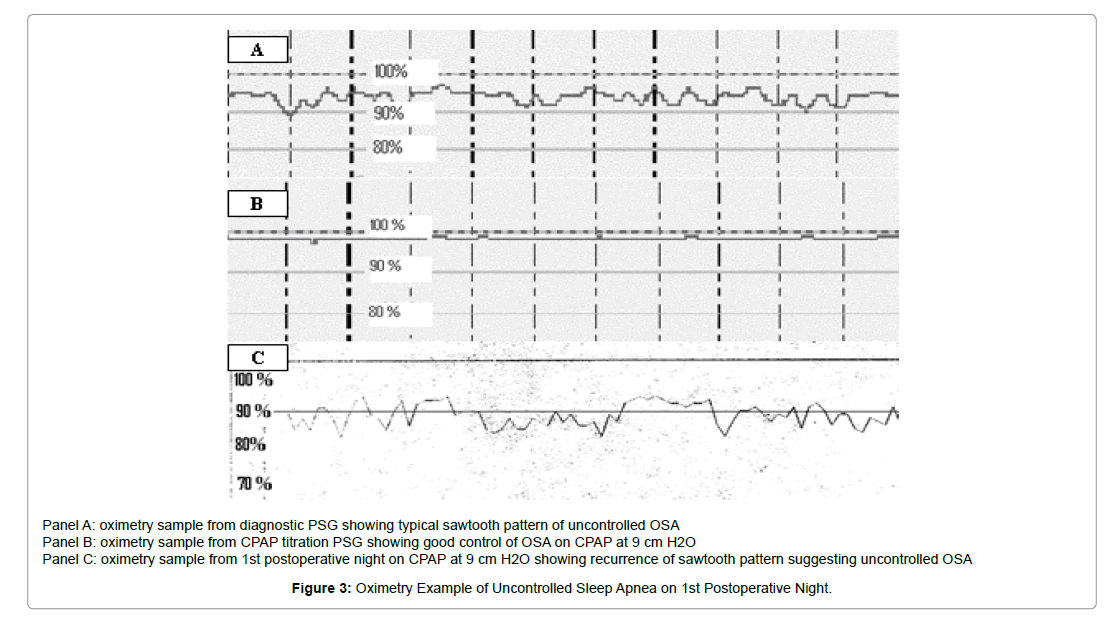
Figure 3: Oximetry Example of Uncontrolled Sleep Apnea on 1st Postoperative Night.
Use of positive airway pressure therapy has been advocated as a protective therapy for use in patients with OSA during the postoperative time [18,19] and recent guidelines agree with this approach [20-24]. However, current data are limited to case series and PAP use in OSA patients postoperatively has not been systematically studied. The results of the present study call into question the efficacy of previously determined PAP pressure settings in the postoperative setting and suggest that postoperative nocturnal oximetry monitoring may be indicated even in PAP-treated OSA patients.
While the majority of the subjects in this study were not hypoxic on the night after surgery, the duration and severity of hypoxia in a subset of subjects was significant. In some cases, the degree of nocturnal hypoxia mirrored that of untreated OSA (Figure 1) and, in the postoperative setting, could place them at risk for cardiopulmonary complications [13,22]. In this study, nursing interventions in the HG may have prevented the development of some adverse events that might otherwise be seen.
The American Academy of Sleep Medicine’s most recent (2003) clinical practice review on the perioperative care of individuals with OSA recommended PAP use postoperatively in those with known OSA on PAP prior to surgery, and that “patients should be monitored for evidence of impaired gas exchange and upper airway obstruction (following surgery).” [20]. The duration of this monitoring was not specified. The current study suggests that oximetry monitoring for at least the first postoperative night may be indicated. The American Society of Anesthesiologists Task Force recommendations (2006) also advocated the use of PAP therapy postoperatively for patients with PAP-treated OSA, and felt that continuous pulse oximetry monitoring was warranted in patients who are “at increased perioperative risk from OSA” [21]. Details regarding who is at “increased perioperative risk” were not stated.
More recently, a postoperative management algorithm recommended continuous oximetry monitoring in OSA patients using PAP therapy postoperatively, though only in those noncompliant with PAP therapy preoperatively, those with severe OSA (defined as an AHI >30), and those with “recurrent respiratory events” in the PACU (recurrent hypoxia, episodes of bradypnea, a witnessed apnea or pain-sedation mismatch) [23]. These recommendations do not take into account the baseline supine AHI, postoperative fluid balance, and narcotic dose, factors associated with the development of nocturnal hypoxia in the present study.
The etiology for the hypoxia noted in some of the subjects could not be fully determined in this study. Based on the oximetry waveforms, uncontrolled sleep apnea appears to play a role, though it is unclear if it is due to uncontrolled obstructive apneas or the development of central apneas, which could result from the use of narcotics. It is noteworthy that 42% of the nonhypoxic group had evidence of uncontrolled sleep apnea on their oximetry tracings (Figure 2). It is possible that either the residual effects of anesthesia (especially in those undergoing afternoon surgeries) and/or the use of narcotic analgesics postoperatively may have resulted in worsening of the baseline sleep apnea and thus a lack of control on the subject’s home PAP setting. Another consideration is that the subject’s sleep apnea is no longer controlled on their home PAP settings as the titration studies were performed, on average, 1-2 years prior to their surgery. Weight did increase in both groups, though not significantly and thus this possibility cannot be excluded. However, it should be noted that there are no current guidelines recommending a repeat PAP titration prior to elective surgery in OSA patients on PAP therapy at home. Significant PAP mask leak, while not noted by the nursing or respiratory personnel, could also contribute to the appearance of uncontrolled sleep apnea. Further study with formal PSG testing will be required to determine the nature of the respiratory events and the potential role of air leaks. Alternative PAP therapies, such as autoadjusting CPAP (for OSA) or adaptive servo ventilation (for central apnea), may be useful in postoperative OSA management.
Some of the nocturnal hypoxia seen may also have been related to anesthetic / narcotic-induced hypoventilation. Arterial blood gas analysis and CO2 monitoring were not performed in this study, and thus this possibility cannot be excluded. Future studies should include CO2 monitoring as hypoventilation may influence the choice of PAP therapy. The increased positive net fluid balance and rates of clinically determined atelectasis in the hypoxic group could have also contributed to hypoxia postoperatively by a mechanism unrelated to the upper airway.
Use of CPAP postoperatively appears feasible. A 2009 study noted that 63% of patients using CPAP preoperatively were placed on CPAP the night after surgery [24]. In the present study, subjects were required to use CPAP following surgery and over 90% tolerated it without significant difficulty. This suggests that CPAP use should be encouraged postoperatively in patients accustomed to using PAP therapy at home.
There are some limitations to this study. Oximetry recording does not reveal the cause of hypoxemia and thus studies with PSG and CO2 monitoring are needed. Oximetry recordings also do not allow for sleep-wake differentiation and some of the hypoxia noted may represent wake-time hypoxia. On the other hand, the ODI is determined by the number of desaturations divided by the recording time, not sleep time, and thus the ODI is likely underestimated. Another limitation is the lack of objective pre and postoperative CPAP compliance data. Subjective compliance was required to enroll in the study, though subjective reporting typically overestimates use. Postoperatively, CPAP use was documented by nursing and respiratory personnel, but objective timeon- pressure data was not available. Likewise, objective leak data was not obtained, which could be an important factor in poorly controlled sleep apnea. And finally, the number of subjects in the study was small and larger studies with more advanced monitoring are needed.
In summary, this study provides evidence supporting the use of routine oximetry monitoring in OSA patients following surgery, even in those treated with PAP therapy. It is hoped that by doing so, adverse events may be avoided, though larger studies are needed to confirm this. The mechanism(s) for the hypoxia noted, and how best to manage it, warrant further investigation.
Dr. Brar: contributed to the study design, data collection, analysis and manuscript preparation. Dr. Sharma: contributed to the study design, data collection and manuscript preparation. Dr. Khanna: contributed to data collection and manuscript preparation. Dr. Auckley: contributed to study design, analysis and manuscript preparation. Dr. Auckley takes responsibility for the integrity of the work as a whole.