Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Case Report - (2016) Volume 4, Issue 6
Patients with coumarin induced skin necrosis presents with painful purpura and erythematous bluish swelling of the skin complicated by blister formation, hemorrhage and immanent gangrene. Coumarin induced hemorrhagic skin necrosis occurs within one week after initiation of coumarin treatment at time of prolonged INR caused by an imbalance within the vitamin K dependent anticoagulant and procoagulant factors with severe protein C and factor VII deficiency as compared to near normal factor II, X and IX. Treatment consists of vitamin K supplementation and short-term discontinuation of coumarin. Patients with pre-existing congenital protein C deficiency or acquired protein C deficiency due to vitamin K deficiency are at increased risk for the development of coumarin skin necrosis. In this report we described a case of coumarin induced hemorrhagic skin necrosis and a case of spontaneous hemorrhagic skin necrosis during an acute episode of severe vitamin K deficiency due to cholestasis in the absence of coumarin treatment. An imbalance within anticoagulant and procoagulant vitamin K dependent factors with severe acquired protein C and factor VII deficiency but still normal values of factor II, IX and X at time of prolonged prothrombin time (INR 5.0) due to severe vitamin K deficiency could be identified as the cause of spontaneous thrombo-hemorrhagic skin necrosis.
Keywords: Coumarin skin necrosis; Coumarin; Spontaneous hemorrhagic skin necrosis; Vitamin K; Protein C deficiency
Ten years after the introduction of coumarin for the treatment of venous thrombosis and pulmonary embolism Verhagen et al. in The Netherlands draw attention to the occurrence of hemorrhagic skin necrosis in thrombosis patients featured by strongly prolonged prothrombin time in 9 Dutch cases with hemorrhagic skin necrosis in the first week after initiation of dicumol treatment [1-3]. A previous case was described by Flood et al. as an unusual case of “Thrombophlebitis migrans [4]. Verhagen published 13 cases with local hemorrhage and necrosis of the skin during anticoagulant therapy with dicumol or dicumacyl [5]. The coumarin skin necrosis suddenly developed as purpura and edema followed by hemorrhagic blisters, necrosis and gangrene of the skin. The skin necrosis rapidly occurred 3 to 10 days after intiation of coumarin treatment at time of strongly prolonged prothrombin time. Coumarine skin necrosis during long-term coumarin treatment is rare [5-8]. The localisation of hemorrhagic skin necrosis in 71 cases from the literature was the thight in 24, mammae in 16 hip in 8, flank in 4 upper arm in 3 and lower leg/ankle in 5 cases [9]. The histopathological skin lesions in the early stage of skin purpura and erythematous swelling are featured by occlusive fibrin thrombi in capillaries and venules without signs of vasculitis. Based on personal observations on the curative effect of Vitamin K supplementation at time of strongly prolonged prothrombin time (INR), Loeliger hypothesized between 1975 and 1977 that severe factor VII deficiency was an obligate prerequisite for the development of severe coumarin induced hemorrhagic skin necrosis [10,11]. With the discovery of hereditary protein C deficiency as cause of congenital thrombophila it became clear that protein C is a natural anticoagulant at the level of vessel wall endothelium in the microcirculation [12-14]. Two studies of Loeliger et al. incontrovertible demonstrated that severe protein C and factor VII deficiency as compared to the vitamin K dependent procoagulant appeared to be a good explanation for the etiology of coumarin induced hemorrhagic skin necrosis [11,14]. Vitamin K supplementation and short discontinuation of coumarin treatment for a few days in the early stage of swollen skin purpura could prevent the progression into blister formation and hemorrhagic skin necrosis [14,15]. Purpura fulminans and skin necrosis in neonates with homozygous protein C deficiency is caused by diffuse thrombosis in the microcirculation of capilaries and venules [16], similar as seen as in the early stages of coumarin induced skin necrosis [14]. Lewandowski oberved that intravenous protein C concentrate induced a rapid cure of coumarin induced skin necrosis in a patient with heterozygous protein C deficiency [17].
A 71 year-old man rapidly developed within a few days after resume of vitamin k antogonist (acenocoumarol) progressive painful and increasing bluish skin discolouration (purpura) of the lower leg and was acutely referred with pronounced red-bluish skin discolouration and swelling of the lower leg (Figure 1). The angiogram showed normal peripheral arteries and compression ultrasound excluded deep vein thrombosis. Ten days before admission anticoagulation was discontinued because of transurethral prostatectomy. Fourdays before admission treatment with acenocoumarol was started again. At time of hemorrhagicskin necrosis at admission the PT was prolonged, 40 seconds (normal value less than 13 seconds) (INR 3.7). Skin punch biopsy from an area of bluish disolouraed skin lesion of the lower leg showed numerous fibrine thrombi in the superficial and deeper capillaries and venules with erythrocytic extravasstions (Figure 1) clearly consistent with coumarin induced skin purpura 4 days after re-institution of coumarin treatment at time of prolonged PT (INR 3.6).
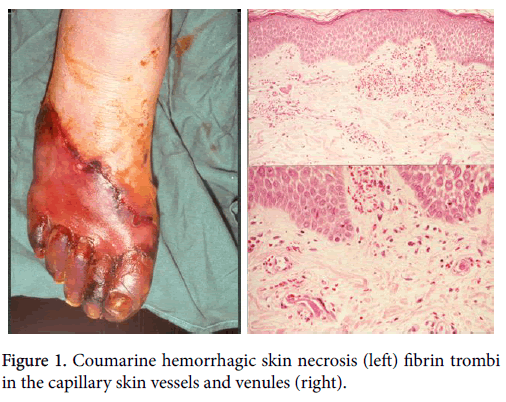
Figure 1: Coumarine hemorrhagic skin necrosis (left) fibrin trombi in the capillary skin vessels and venules (right).
A 58-year-old woman without previous thrombosis or any other disease developed within a few months period severe extrahepatic cholestasis due to an obstructive tumour in the liver hilus suspicious for sclerosing cholangitis of gall-duct carcinoma on ERCP. The liver function parameters were increased: bilirubine 514 umol/L, alkaline phosphatase 617 U/L, gamma-gt 348, SGOT 50, LDH 632 U/L. Routine coagulation investigation at admission was normal: prothrombin time (PT) 15 seconds (sec), trombotes (TT) 35 sec and normotest (NT) 43 sec (Table 1). At day 12 of admission extreme painful swelling, cyanosis and edema of the toes and forefoot developed. The peripheral arterial pulses were normal. Sings of venous thrombosis were absent. Within four days all toes, the left forefoot and the right foot became erythematousl swollen with bluish discolouration of the right foot, blister formation and immanent gangrene (Figure 2). On day 13 of admission severe vitamin K deficiency was diagnosed: APTT 56 sec, PT 61 sec (INR 5.0), TT<3%, NT<10%, factor (F) V 100%, fibrinogen 1.6 g/L, fibrin degadation products (FDP) absent, antithrombin 103%, antiplasmin 97%. The values were low for FVII, 28%, and protein C, 22% but normal for F II, 95%, and F X, 85%. After treatment with one low dose vitamin K (5 mg) the coagulation abnormalities normalized within 36 hours: APTT 27 sec, PT 15 sec, TT 110% and NT 77% (Table 1).
| Day of admission | 1 | 13 | 13.5 | 15 | 17 | Normal values |
|---|---|---|---|---|---|---|
| Bilirubin | 514 | 624 | 640 | 2-12 mmol/L | ||
| Alkaline phospatase | 671 | 1278 | 392 | 25-75 U/L | ||
| Gamma gt | 348 | 954 | 444 | 5-35 U/L | ||
| SGOT | 68 | 232 | 144 | 5-30 U/L | ||
| SGPT | 50 | 93 | 41 | 5-30 U/L | ||
| LDH | 732 | 2024 | 1590 | 160-320 U/L | ||
| Vitamin K1 | ||||||
| Trombocytes | 133 | 109 | 5 mg | 83 | 81 | 150-350×109/L |
| APTT | 56 | 27 | 22-45 sec | |||
| Protrombin time | 61 | 15 | 15-19 sec | |||
| Trombotest | 35 | <23 | 77 | 110 | 65-110% | |
| Normotest | 43 | <11 | 85 | 77 | 65-110% | |
| Trombin time 10E 5E | 14 | 13 | 9-13 sec | |||
| 21 | 26 | 16-23 sec | ||||
| Factor V | >1.00 | >1.00 | 0.80-1.40 U/L | |||
| Fibrinogen | 1.6 | 1.2 | 1.6-2.3 g/L | |||
| FDP | <40 | 40-80 | <40 | |||
| Antitrombin | 1.20 | 1.03 | 0.88 | 0.80-1.25 U/ml | ||
| Antiplasmin | 0.89 | 0.87 | 0.77 | 0.80-1.20 U/ml | ||
| Factor VII | ||||||
| Ca dependent | 0.16 | 0.65-1.40 U/ml | ||||
| Ca independent | 0.28 | 0.65-1.25 U/ml | ||||
| Protein C antigen | 0.22 | 0.65-1.25 U/ml | ||||
| Factor II antigen | 0.97 | 0.65-1.25 U/ml | ||||
| Factor X antigen | 0.87 | 0.65-1.25 U/ml | ||||
| The coagulation disturbances of anticoagulant and procoagulant factor at diagnosis of spontaneous hemorrhagic skin necrosis (day 13) was consistent with severe vitamin K deficiency caused by extrahepatic cholestasis in the absence of coumarin treatment. Measurement of the vitamin K dependent factors showed very low levels for F VII and protein C and still completely normal values for F II and F X. After treatment with one oral dose of vitamin K1 5 mg the coagulation abnormailites were completely normal again within 2 days. This observation is diagnostic for severe vitamin K deficiency as the cause of spontaneous hemorrhagic skin necrosis in this case.(Figure 2 ) [14,15]. |
||||||
Table 1: Results of liver function test and coagulation investigations before and during the episode of spontaneous hemorrhagic skin necrosis en after treatment of severe vitamin K deficiency with vitamin K1.
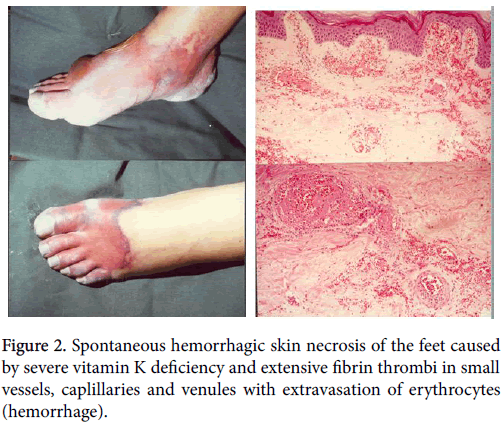
Figure 2: Spontaneous hemorrhagic skin necrosis of the feet caused by severe vitamin K deficiency and extensive fibrin thrombi in small vessels, caplillaries and venules with extravasation of erythrocytes (hemorrhage).
Skin wedge excisions and liver biopsy were performed on day 20 of admission at time of complete correction of the coagulation defect by vitamin K 5 mg/day was not followed by secondary bleedings. Histopathology of two skin wedge excision from areas of erythematous lesions and skin necrosis revealed the presence of extensive fibrin thrombi in small blood vessels, capillaries and venules and extravasation of erythrocytes (Figure 2) without vasculitis.
The liver biopsy showed extensive infiltration of biliary duct carcinoma with pronounced cholestasis of liver parenchym. The findings in this case of well documented case of hemorrhagic skin necrosis caused by severe vitamine K deficiency in Figure 2 are identical to coumarin induced skin necrosis in Figure 1. The rapid induction of severe acquired protein C and FVII deficiency with completely normal values of F II and F X by coumarin or severe vitamin K deficiency can be regarded as the cause of hemorrhagic skin necrosis (Table 1).
Teepe et al. desribed recurrent coumarin induced skin necrosis in a 56 year old woman with acquired protein C deficiency [15]. The patient was treated in 1984 with phenprocoumon for mitralis insufficiency and atrial fibrillation. Four episodes of coumarin necrosis at time of strongly prolonged INR (Figure 3).
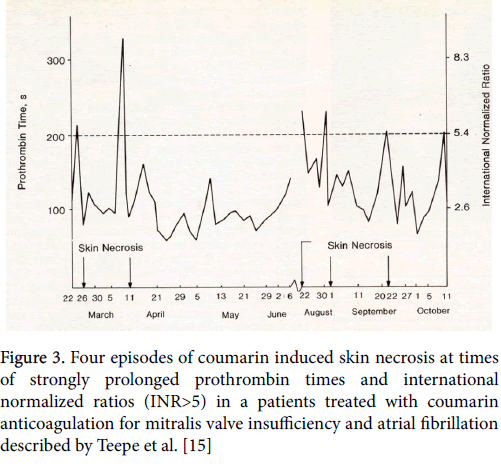
Figure 3: Four episodes of coumarin induced skin necrosis at times of strongly prolonged prothrombin times and international normalized ratios (INR>5) in a patients treated with coumarin anticoagulation for mitralis valve insufficiency and atrial fibrillation described by Teepe et al. [15]
The first episode of coumarin necrosis on march 22 at an INR of 5.8 was treated with 10 mg vitamin K and discontinuation of phenprocoumon. Multiple painful ecchymoses of the skin of the tight and forefoot developed after 2 days complicated by hemorrhagic blisters 3 days later. After correction of the INR by vitamin K, phenprocoumon was started again after one week and the skin lesions spontaneously disappeared. One week later on April 9 the INR was suddenly strongly prolonged (Figure 3). Anticoagulation with phenprocoumon was discontinued for 1 week and the INR was corrected again with vitamin K. Two days later large painfull erythromatous indurated swelling and purpara of the skin (10 × 20 cm) on both lower legs developed followed by hemorrhagic blister formation and necrosis. Phenprocoumon was started again on april 16. On august 22 a strongly prolonged INR of 6.3 was rapidly follwed by small painful (2 × 3 cm) hemorrhagic skin leasions, which rapidly disappeared after treatment of vitamin K and transient discontinuation of phenprocoumon. On September 20 a strongly prolonged INR of 5.4 was followed by multiple small skin necrosis on the lower legs, which again disappeared after treatment with vitamin K and transient discontinuation of phenprocoumon (Figure 4).

Figure 4: Warfarin 5 mg/day induced within 4 to 5 days after start a strongly prolonged INR associated with gangrene of the skin and extremily low protein C (PC) level of 0.05 and 0.02, which could be corrected by vitamin k supplementation on the basis of which the only diagnosis possible is coumarin necrosis.
In this study, the vitamin K dependent procoagulant and anticoagulant factors were measured at two time points of strongly prolonged INR of 6.3 on august 22 and 4.7 on September 20 (Table 2).
| Anticoagulant factors | 22-081986 | 20-09-1986 | Normal values |
|---|---|---|---|
| Proteïne C antigen | 0.38 | 0.26 | 0.67-1.40 IU/ml |
| Proteïne C activity | 0.02 | 0.11 | 0.61-1.32 IU/ml |
| Proteïne S antigen | 0.35 | 0.50 | 0.67-1.25 IU/ml |
| Procoagulant factors | |||
| Factor VII activity | 0.07 | 0.12 | 0.65-1.50 IU/ml |
| Factor X antigen | 0.46 | 0.57 | 0.65-1.45 IU/ml |
| Factor II antigen | 0.37 | 0.41 | 0.65-1.45 IU/ml |
| Factor II activity | 0.21 | 0.26 | 0.65-1.45 IU/ml |
| Trombostest | 233 | 158 | 44 seconden |
| INR | 6.3 | 4.7 | 2.5 ± 0.5 (anticoagulation) |
Table 2. Results of coagulation investigations in a case of recurrent hemorrhagic coumarin skin necrosis in the study of Teepe et al. [15].
Protein C activity was strongly decreased as compared to protein C and S antigen levels. At time of strongly prolonged INR, Factor (F) VII activity was more pronounced decreased as compared to F II activity and strongly decreased as compared to F II and F X antigen levels. Dr Loeliger concluded in 1986 that rapid induction of a strongly prolonged INR is associated with severe acquired deficiency of protein C activity as compared to FII activity and as compared to F II, X, PC and PS antigen levels can be regarded as the cause of thrombotic skin necrosis and that severe deficency F VII activity contrinutes to the hemorrhagic (erythrocyte extravasation) complications of coumarin skin necrosis. Pabinger et al. observed in 1986 hemorrhagic skin necrosis of the toes in a patient with heterozygous protein C deficiency (protein C: Ag 32% and protein C activity 30%) on the 4th day of coumarin treatment overlapping with effective intravenous anticoagulation with heparin [16]. The rapid and very low protein C and F VII levels at strongly prolonged INR within one week of vitamin K antagonist is the cause of hemorrhagic skin necrosis after initiation of coumarin treatment in case 1 and also at time of rapid induction of severe vitamin K deficiency in our case 2 of spontaneous hemorrhagic skin necrosis. Such extensive coumarin skin necrosis is frequently associated with features of activated diffuse intravascular coagulation. The diagnosis of coumarin necrosis is usually overlooked in routine clinical and laboratory medicine since one low dose of vitamin K rapidly corrects the severe FVII within 12 hours and because PC deficiency and because skin punch biopsy to diagnose coumarin skin necrosis are never performed. Such overlooked coumarin skin necrosis is usually complicated by local infections and unexplained bleedings and frequently misdiagnosed as diffuse intravascular coagulation. Consequently the diagnostic strategy is mainly focused on the differential diagnosis of diffuse intravascular coagulation, atypical vasculitis, heparin induced thrombocytopenia (HIT), which frequently starts after having neglected the possibility of coumarin necrosis [16]. This is illustrated by the recent initial misinterretation of warfarininduced venous limbs ischemia/gangrene as a novel clinically distinct syndrome complicating cancer patients. In the first case of Warkentin et al, two episodes of coumarin necrosis: (episode 1 as phlegmasia alba dolens and episode 2 as gangrene) were preceded by rapid prolongation of INR within 6 days after start of warfarin (Figure 5) [16].
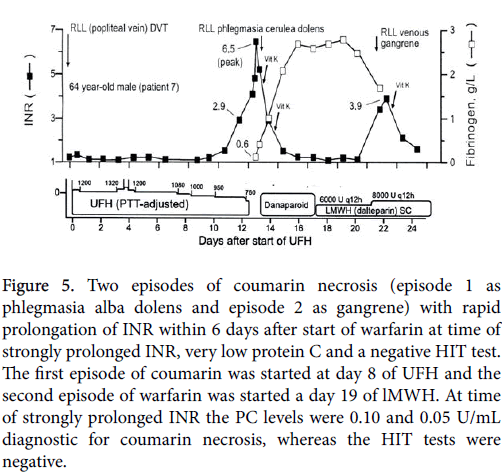
Figure 5: Two episodes of coumarin necrosis (episode 1 as phlegmasia alba dolens and episode 2 as gangrene) with rapid prolongation of INR within 6 days after start of warfarin at time of strongly prolonged INR, very low protein C and a negative HIT test. The first episode of coumarin was started at day 8 of UFH and the second episode of warfarin was started a day 19 of lMWH. At time of strongly prolonged INR the PC levels were 0.10 and 0.05 U/mL diagnostic for coumarin necrosis, whereas the HIT tests were negative.
The first episode of coumarin was started at day 8 of UFH in (Figure 5) and the second episode of warfarin was started a day 19 of LMWH in (Figure 5). At time of phlegmasia cerula dolens and at time of gangrene the INR was strongly prolonged INR, which was associated with very low protein C as the cause of the very prolonged INR but with a negative HIT test. In retrospect, the strongly prolonged INR and the very low protein C (PC) levels at time of strongly prolonged INR were very low, 0.10 and 0.05 U/mL, and pathgnomonically diagnostic for coumarin necrosis as the cause of phlegmasia alba dolens (episode 1) and gangrene of the skin (episode 2) in (Figure 5). In the second ilustrated case of Warkentin shown in Figure 5, warfarin 5 mg/day induced within 4 to 5 days after start a strongly prolonged INR associated with gangrene of the skin and extremely low protein C (PC) level of 0.05 and 0.02, which could be corrected by vitamin k supplementation on the basis of which the only diagnosis possible is coumarin necrosis [16,17]. The recently described warfarin-induced venous limb ischemia/gangrene complicating cancer by Warkentin et al. [17] is not a novel syndrome but has all features of coumarininduced thrombo hemorrhagic skin necrosis and ischemia.