Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 5
Objective: Recently few studies have described presence of cervical spine anomalies in obstructive sleep apnoea syndrome (OSAS) patients. It is also reported that some cases of cervical spine pathologies and osteophytes producing obstructive sleep apnea. We aim to investigate the prevalence of facet joint arthrosis and degenerative disc disease (DDD) in cervical spine using computed tomography (CT) in OSAS patients.
Materials and Methods: We studied on thirty patients with OSAS who had cervical spine CT. Facet joints were evaluated in four grades and scored in 1-4 points by using multiplanar CT images. Disc levels was evaluated by using two-point subjective scale for loss of height, posterior osteophytes, endplate sclerosis, and spinal canal stenosis to determinate DDD. Degeneration of anterior atlanto-odontoid joint (AAOJ) were classified into four grades. Tomographic findings were compared with those for thirty control subjects.
Results: The mean degeneration scores of C2-T1 facet joints and C2-C5, C7-T1 disc spaces were significantly higher in the cases of OSAS group than the cases of the control group. There were no significant differences in the mean degeneration scores for C5-6 and C6-7 cervical intervertebral disc levels between the groups. Degeneration scores of the facet and disc for whole cervical spine in the cases of the OSAS group was significantly higher than in cases of the control group (P<0.001 and P=0.002). AAOJ degeneration degrees showed differences between the groups. Statistically significant correlations were found between the OSAS degrees and the intervertebral disc degeneration (R=0.338, P=0.007) and facet joint degeneration (R=0.543, P=0.000) for all cervical vertebrae.
Conclusions: The cervical spine of the OSAS patients has more severe disc degeneration and facet joint and AAOJ arthrosis, compared to subjects without OSAS. This findings may contribute to clinic evaluation of OSAS patients with servical pain and limited movement.
Keywords: Cervical spine, Intervertebral disc degeneration, Facet joint, Multidetector computed tomography, Sleep apnea, Obstructive
Obstructive sleep apnea syndrome (OSAS) is a variety of sleepdisordered breathing characterized by repetitive episodes of upper airway obstruction during sleep. These episodes are associated with recurrent oxyhemoglobin desaturations, and they give rise to intermittent hypoxemia, hypercapnia, acidosis, sympathetic nervous system activation and arousals from sleep [1]. It has been shown that the frequency of repeated apnea episodes is correlated with the cardiovascular and cerebrovascular complications in patients with OSAS [1-4]. The pathophysiology of the disease has not been fully identified yet. However, obesity and upper airway tissue abnormalities decreasing width of the upper respiratory tract may increase the predisposition to OSAS [5,6]. It has been described some craniofacial abnormalities such as thicker soft palate, bigger neck circumference, more inferior localization of the hyoid bone, large cranio-cervical angle and more extended head posture in OSAS patients [1,3,6,7]. Recently, presence of cervical spine anomalies including posterior arch deficiency and fusion anomalies in OSAS patients have been reported in some studies [8-10]. Additionally, it has been observed that OSAS patients with block fusion in the cervical vertebrae differ significantly in craniofacial profiles (such as larger anterior face height, greater mandibular length) from the other OSAS patients [9]. It is also reviewed that some cases of cervical osteophyte may predispose patients to OSAS [11]. On the other hand, to our knowledge, there is no information about the frequency and distribution of cervical spine degeneration in OSAS patients. Therefore, the aims of the present study were to investigate the prevalence of facet joint arthrosis and degenerative disc disease in cervical spine using multidetector computed tomography (CT) in adult patients with OSAS and to compare those of the cervical spine in a group of adult subjects with no history of OSAS.
This study protocol was approved by our institutional ethics committee (registration number: KOÜ KAEK 2015/60). We performed a retrospective study of adult OSAS patients who had apnea/ hypopnea index (AHI) ≥ 5 per h according to overnight polysomnography in sleep center of our hospital, Kocaeli (Turkey).
After providing their informed consent, subjects with OSAS underwent overnight polysomnographic recording (Embla N 7000). The polysomnography included electroencephalogram, electrooculogram, chin and leg electromyography, electrocardiography, snoring, oronasal thermistor, nasal pressure transducer, finger pulse oximeter, thoracic and abdominal respiratory movements, and body position. Apnea was defined as ≥ 90% decrease from baseline in the oronasal thermistor signal amplitude for at least 10 seconds, and hypopnea was defined as ≥ 50% decrease from baseline in the nasal cannula signal amplitude at least for 10 seconds. The apnea/hypopnea index (AHI) was defined as the number of occurrences of apnea/ hypopneas per hour (/h) during sleep. Patients with AHI of 5-15 per h was considered mild, AHI of 15-30 per h was considered moderate, and AHI ≥ 30 per h was considered severe OSAS.
The controls were diagnosed as non-OSA subjects based on clinical criteria, which means they did not present a medical history of snoring or sleep apnea symptoms. The control subjects also did not have any sleep testing or complete questionnaires regarding sleepiness.
Both of the groups were selected from patients who underwent cervical CT because of neck pain without neurologic deficits. Subjects with congenital spinal disease, scoliosis, inflammatory arthropathy, history of trauma or fracture or spinal surgery, severe obesity (BMI>30), severe diabetes mellitus, and history of metabolic disease were excluded from both OSAS and control groups. All cervical spine images were taken with a 16-multidetector computed tomography device (Activion 16; Toshiba Medical Systems). All of the OSAS patients and control subjects were in the supine position. Continuous axial sections with 2 mm thickness were obtained from the base of the cranium to the first thoracic vertebrae (T1) level. Coronal and sagittal reformatted images were created by using bone algorithm. Images were evaluated by two radiologists to assess interobserver reliability. The second radiologist had no prior knowledge about patients’ clinical information. All the images were examined in three categories in terms of cervical spine degenerative changes. 1) Degenerative arthrosis of bilateral facet joints between the C1-T1 vertebrae; 2) findings of degenerative disc disease in C2-T1 intervertebral disc spaces; and 3) degeneration findings in anterior atlanto-odontoid joint (AAOJ).
Facet joints were evaluated in four categories according to the grading system which was suggested by Park et al. [12]: Grade I, normal; Grade II, degenerative changes including joint space narrowing, cyst formation, small osteophytes without joint hypertrophy; Grade III, joint hypertrophy secondary to large osteophytes without fusion; Grade IV, bony fusion of the joint. Then, the facet joints in each intervertebral level was scored with the following scoring system: grade I: 1 point, grade II: 2 points, grade III: 3 points, grade IV: 4 points. When each facet joint in the same disc level had different degeneration grades, the grade value, which showed the higher degeneration of facet joint, was taken into consideration for disc level. Facet joint degeneration score for whole cervical spine was created by adding the facet degeneration scores at seven intervertebral disc levels (C1-C2, C2-3, C3-4, C4-5, C5-6, C6-7, and C7-T1).
To evaluate degenerative disc disease, we used a scoring system described by Walraevens et al. [13] on lateral cervical graphies with a simplified version of its. On sagittal CT images, each intervertebral disc space (C2-3, C3-4, C4-5, C5-6, C6-7, and C7-T1) was evaluated for a ‘loss of height’, ‘posterior osteophytes’, ‘endplate sclerosis’, and ‘spinal canal stenosis due to posterior osteophytes’ (anterio-posterior diameter of the spinal canal was <12 mm in the midsagittal images) by using a two-point subjective scale (0 point: absent; 1 point: present). At last, each intervertebral disc had degeneration score ranging between 0 and 4. Total score of degenerative disc disease for whole cervical spine was created by adding the disc degeneration scores at six intervertebral disc levels (C2-3, C3-4, C4-5, C5-6, C6-7, and C7-T1).
The degeneration of the AAOJ were evaluated according to Lakshmanan et al. [14] by using axial and sagittal CT images. The degenerative changes were graded as: none (Grade 0), normal joint space with no osteophyte formation; mild (Grade 1), narrowed joint space or normal joint space with osteophyte formation; moderate (Grade 2), obliterated joint space with or without osteophyte formation; and severe (Grade 3), ankyloses of the joint with excrescences either in the joint or transverse ligament calcification, or both.
SPSS v.20.0 statistical software was used for statistical analysis (IBM; Chicago). The level of statistical significance was P<0.05. The Mann - Whitney U -test and Pearson’s chi-square test were used to analyze the variables. Pearson’s r correlation coefficients were used to investigate the linear correlation between OSAS degrees and facet joint degenerations, and between OSAS degrees and cervical disc degenerations. The effect of gender on severity of disc degeneration was assessed by univariate analysis, adjusting for men and women. Kappa statistics were used to compare interobserver reliability. Kappa values<0 were interpreted as poor agreement, between 0.0-0.20 as slight agreement, between 0.21-0.40 as fair agreement, between 0.41-0.60 as moderate agreement, between 0.61-0.80 as substantial agreement, and between 0.81-1.00 as almost perfect agreement.
A total of 30 patients (18 male and 12 female) with fulfilling the criteria for OSAS and 30 control subjects (14 male and 16 female) were included in the study (P=0.12). There were more women in the control group and gender was not a statistically important demographic factor associated with disc degeneration. The mean age was 52.43 years ± 11.55 years (34 years - 77 years, median: 52) in OSAS group, and 57.13 years ± 11.27 years (34 years - 73 years, median: 57) in control subjects (P=0.72). The mean BMI was not statistically different between the groups (P=0.46) (Table 1). As we not studied in obese patients (BMI>30), our findings may not be applicable to patients with high BMI. According to AHI scores, nine patients had mild, four patients had moderate and seventeen patients had severe OSAS.
| Variable | OSAS (Mean ± S.D; n = 30) | Group C (Mean ± S.D; n = 30) | P value |
|---|---|---|---|
| Age (years) | 52.43 ± 11.55 | 57.13 ± 11.27 | 0.72 |
| BMI (m/kg2) | 22.33 ± 3.91 | 21.57 ± 4.15 | 0.46 |
| Gender | 18 M, 12 F | 14 M, 16 F | 0.12 |
| M: male, F: female, Group C: control subjects | |||
Table 1: Parameters of OSAS and control group.
The numbers of facet joints with degeneration grades at the seven cervical intervertebral levels which are consisting of OSAS and control cases are shown in Table 2. We evaluated totally 210 bilateral facet joints of seven intervertebral levels in thirty subjects of each group (Figures 1 and 2). The mean degeneration scores of facet joints at C2-3, C3-4, C4-5, C5-6, C6-7, C7-T1 cervical intervertebral disc levels were significantly higher in the cases of OSAS group than in the cases of the control group (P=0.000, P=0.050, P=0.001, P=0.000, P=0.000, P=0.000, respectively). There was no significant difference between the groups in terms of the mean degeneration scores of the facet joints at C1-2 intervertebral disc levels (P=0.078). The total score of facet degeneration in all cervical vertebrae was significantly higher in the OSAS group, compared to the control group (P=0.000) (Table 3).
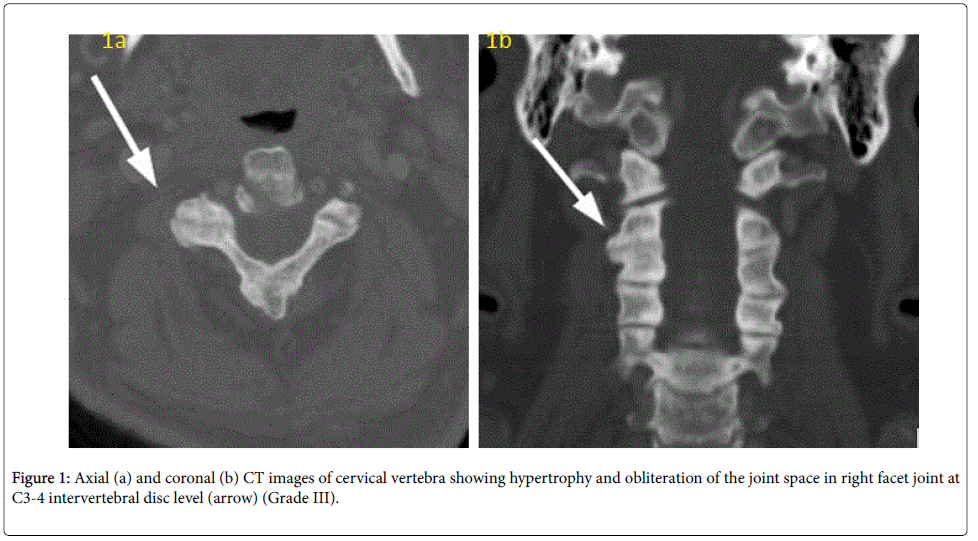
Figure 1: Axial (a) and coronal (b) CT images of cervical vertebra showing hypertrophy and obliteration of the joint space in right facet joint at C3-4 intervertebral disc level (arrow) (Grade III).
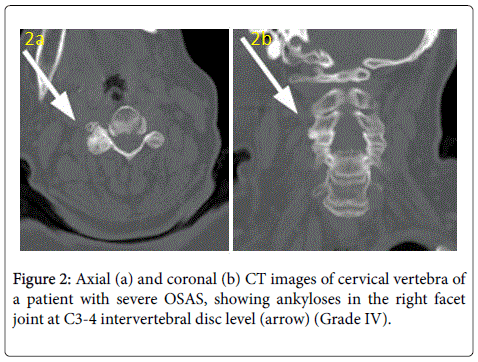
Figure 2: Axial (a) and coronal (b) CT images of cervical vertebra of a patient with severe OSAS, showing ankyloses in the right facet joint at C3-4 intervertebral disc level (arrow) (Grade IV).
| OSAS | Group C | |
|---|---|---|
| Grade | n (%) | n (%) |
| I | 79(37.6) | 175 (83.3) |
| II | 78 (37.2) | 24 (11.5) |
| III | 34 (16.2) | 11 (5.2) |
| IV | 19 (9.0) | 0 (0) |
| Group C: Control subjects | ||
Table 2: The total number of bilateral facet joints in seven cervical intervertebral levels according to degeneration grades.
| OSAS Mean ± S.D | Group C Mean ± S.D | P value | |
|---|---|---|---|
| C1-2 | 1.10 ± 0.30 | 1.00 ± 0.00 | 0.078 |
| C2-3 | 1.90 ± 0.84 | 1.17 ± 0.46 | 0.000* |
| C3-4 | 1.83 ± 0.95 | 1.40 ± 0.72 | 0.050* |
| C4-5 | 2.03 ± 0.96 | 1.30 ± 0.65 | 0.001* |
| C5-6 | 2.20 ± 0.92 | 1.27 ± 0.58 | 0.000* |
| C6-7 | 2.30 ± 0.83 | 1.20 ± 0.48 | 0.000* |
| C7-T1 | 2.27 ± 0.90 | 1.20 ± 0.40 | 0.000* |
| Total facet joint degeneration score for whole cervical spine | 13.63 ± 4.52 | 8.56 ± 1.85 | 0.000* |
Table 3: Comparison of degeneration grading scores for cervical intervertebral facet joints and total facet joint degeneration score for whole cervical spine between OSAS and control subjects.
When degenerative disc disease of the cervical spine was analyzed, the mean degeneration scores for C2-3, C3-4, C4-5, C7-T1 intervertebral disc levels were significantly higher in cases of the OSAS group than in cases of the control group (P=0.023, P=0.001, P=0.049, P=0.005, respectively).
There were no significant differences in the mean degeneration scores for C5-6 and C6-7 cervical intervertebral disc levels between the groups (P=0.230, P=0.176, respectively).
On the other hand, the total mean disc degeneration score for whole cervical spine in the cases of the OSAS group was significantly higher than in cases of the control group (P=0.002). The comparison of mean scores at the C2-3, C3-4, C4-5, C5-6, C6-7 cervical intervertebral disc levels and mean total scores for whole cervical spine between the groups is shown in Table 4.
| OSAS | Group C | P value | |
|---|---|---|---|
| Mean ± S.D | Mean ± S.D | ||
| C2-3 | 0.63 ± 1.12 | 0.10 ± 0.54 | 0.023* |
| C3-4 | 1.67 ± 1.57 | 0.50 ± 0.93 | 0.001* |
| C4-5 | 2.23 ± 1.40 | 1.47 ± 1.54 | 0.049* |
| C5-6 | 3.00 ± 1.39 | 2.50 ± 1.77 | 0.230 |
| C6-7 | 2.00 ± 1.57 | 1.40 ± 1.81 | 0.176 |
| C7-T1 | 1.40 ± 1.49 | 0.40 ± 1.10 | 0.005* |
| Total disc degeneration score for whole cervical spine | 10.93 ± 6.22 | 6.36 ± 4.39 | 0.002* |
Table 4: Comparison of mean scores for each cervical intervertebral disc levels and total disc degeneration score for whole cervical spine between OSAS group and control subjects.
When the degeneration of AAOJ were analyzed, twenty-five cases (83.3%) had grade 1 and five cases (16.7%) had grade 2 degeneration in OSAS group (Figure 3). Neither grade 0 nor grade 3 degeneration of AAOJ was observed in OSAS group. In the control group, eleven subjects (36.7%) had grade 0, eighteen subjects (60.0%) had grade 1, one subject (3.3%) had grade 2 degeneration of AAOJ. None of the subjects in the control group had grade 3 degeneration of AAOJ. There was a significant difference in AAOJ degeneration percentages between the OSAS group and the control group (P=0.001). The comparison of AAOJ degeneration percentages between both groups is shown in Table 5.
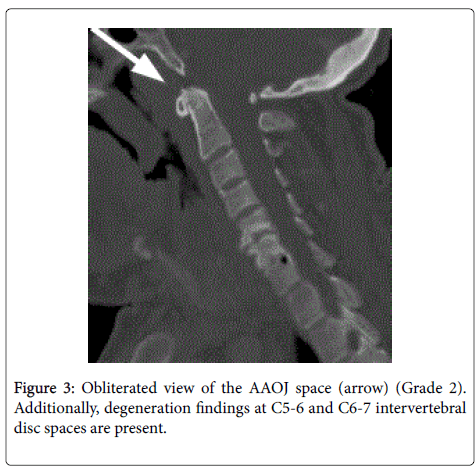
Figure 3: Obliterated view of the AAOJ space (arrow) (Grade 2). Additionally, degeneration findings at C5-6 and C6-7 intervertebral disc spaces are present.
| Atlanto-odontoid joints | OSAS n (%) |
Group C n (%) |
|---|---|---|
| Grade 0 | 0(0.0) | 11 (36.7) |
| Grade 1 | 25(83.3) | 18(60.0) |
| Grade 2 | 5(16.7) | 1(3.3) |
| Grade 3 | 0(0.0) | 0 (0.0) |
Table 5: Comparison of grading of degenerative changes in AAOJ between OSAS group and control subjects.
We investigated the correlation between the degree of OSAS and intervertebral disc degeneration or facet joint degeneration values for all cervical vertebrae. Statistically significant correlations were found for the OSAS degrees with the intervertebral disc degeneration of all cervical vertebrae (R=0.338 P=0.007). Statistically significant correlations were also found for the OSAS degrees with facet joint degeneration levels of all cervical vertebrae (R=0.543, P=0.000). To evaluate the AAOJ, the kappa value for interobserver reliability test was 0.973, which corresponds to almost perfect agreement. To evaluate cervical vertebra disc degeneration and facet joint degeneration, the kappa values for interobserver reliability test were 0.827 and 0.812, respectively, which correspond to almost perfect agreement again.
In the present study, we showed that facet joint arthrosis and intervertebral disc degeneration of the cervical spine existed in more severe grades in patients with OSAS, compared to control subjects. In addition, AAOJ degeneration was more advanced in OSAS group, compared to control subjects.
To our knowledge, there is only a few studies described the morphology of the cervical spine in patients with OSAS in the previous literature [8-10]. In these studies, the authors examined the morphological characteristics in the cervical spine into two categories: ‘posterior arch deficiency’ and ‘fusion anomalies’. Posterior arch deficiency was consisted of partial cleft and dehiscence and fusion anomalies were consisted of fusion, block fusion, and occipitalization. Fusion is defined as fusion of one unit with another at the articulation facets, neural arch or transverse processes in that studies. The prevalence of fusion anomalies in patients with OSAS taken with standardized lateral skull radiography was found out 46% and 43% in the two studies [8,9]. They showed that the fusion anomalies occurred as fusions between C2 and C3, C3 and C4, or C4 and C5 and as block fusions between C2, C3, and C4, C2, C3, C4, and C5, or C3, C4, and C5. They also exposed that the craniofacial profile of OSAS patients with block fusions in the cervical vertebrae and fusion of two vertebrae differed significantly from the craniofacial profile of other OSAS patients [9]. Then, the researchers suggested the associations between craniofacial morphology including the cranial base and fusion of the cervical vertebral column, and they also have explained these relations with the early embryogenesis. In the early embriyogenetic period, when the notochord determinates the development of the vertebral bodies and the basilar part of the occipital bone in the cranial base, it also induces the formation of the para-axial mesoderm forming the vertebral arches. Before the notochord is surrounded by bone tissue and disappears, by means of a kind of signalling from the notochord to the neural crest, bilateral neural crest cells migrate to the craniofacial area to create the mandible, maxilla and lastly the nasofrontal region [15]. Then, in a later study, Sonnesen et al. [15] reported the incidence of fusion anomalies as 21.1% (fusion 10.5%, block fusion 8.8%, and occipitalization 1.8%) in the OSAS patients, when used cone beam CT to overcome the superposition of structures in the cervical vertebrae. In our study, we defined fusion of the facet joint as bony fusion of the joint, seen in grade IV facet degeneration on coronal and axial images. We found that the prevalence of the grade IV degeneration was 9% in OSAS patients, our result is consistent with the findings of Sonnesen et al. [10]. Moreover, we also found that the degeneration grading scores of facet joints in C2-3, C3-4, C4-5, C5-6, C6-7, C7-T1 cervical levels was higher in OSA patients, compared to control subjects. There was a positive correlation between facet joint degeneration and the degree of OSAS. Having evaluated the images, we detected more or less the classic radiographic hallmarks of facets arthrosis, including osteophyte formation and hypertrophy of the articular process, in addition to fusion in grade IV degeneration. Therefore, we suggest that fusions anomalies itselfs or its leading to biomechanical alterations can be a contributing factor for increasing in the degeneration grades for facet joints in OSAS patients.
It is well known that prevalence of cervical facet joint degeneration is associated with aging. Pathological studies on fresh frozen cervical spine specimens, as well as tomographic studies, have shown that the prevalence of cervical facet joint degeneration increases with age [12,16,17]. In the literature, the rate of facet joint degeneration for C2- C7 intervertebral levels have been reported 91.3% in Grade I, 2.9% in Grade II, 5.2% in Grade III, and 0.6% in Grade IV in normal subjects between 40-79 years old [12]. The prevalence of facet joint degeneration in our control group were consistent with values reported in the literature. Our results suggest that the aging process does not contribute significantly to the elevated the rates of facet joint degeneration in patients with OSAS.
In this study, we chose multislice CT imaging to examine degenerative changes of the cervical spine. Because reformatted CT images of the spine with bone algorithms is excellent to demonstrate degenerative changes such as reduced height of the intervertebral space, osteophytes, sclerosis of the adjacent cartilaginous endplates, facet joint arthrosis, calcifications and narrowing of the spinal canal [18,19]. Although the grading system for the cervical facet joint arthrosis on CT images were defined in the literature before, in this study we could not find a appropriate grading and scoring system for tomography to compare findings of disc degeneration in both groups. Therefore, we used a scoring system based on three criteria-i.e. disc height loss, posterior osteophytes and endplate sclerosis, which was defined by Walverens et al. [13] on lateral roentgenograms. We however created a new version of this scoring system by adding the fourth scoring criteria, ‘spinal canal stenosis due to posterior osteophytes’, and then applied its simplified version on the sagittal tomography images.
Cervical intervertebral disc degeneration initially starts in the nucleus pulposus. Once, nucleus pulposus undergoes progressive dehydration with resulting loss of height of the disc space, disc becomes brittle and fibrotic and is unable to provide the necessary elasticity for the maximum loadcarrying capacity, and then apophyseal joints start to grow osteophytes [20]. Osteophytic projections rarely can cause compression of the pharynx, esophagus or upper airway [11]. Some cases with anterior osteophytes have reported that causing obstruction in the retropharyngeal area and lead to sleep disorders [21,22]. On the other hand, airway obstruction due to pressure by large osteophytes and dysphagia has been reported in a few patients with diffuse idiopathic skeletal hyperostosis, who were previously diagnosed with OSAS [23]. In our study, we did not determine too large osteophytes to narrow or pressure on airway in the images of the all subjects. However, degeneration scores at the C2-3, C3-4, C4-5 and C7-T1 intervertebral disc levels and total degeneration score of whole cervical spine were significantly higher in patients with OSAS, compared to the control group. Additionally, there was a positive correlation between disc degeneration grades and severity of OSAS grades. On the other hand, we did not observe statiscally difference for the scores of degeneration at C5-6 and C6-7 cervical intervertebral disc levels between two groups. Previous studies have represented that C5-6 intervertebral disc space has the highest prevalence of disc degeneration and the C6-7 disc space has the second highest prevalence in the cervical spine in a population aged between 21 and 97 years old [24]. These findings of the present study indicated that different mechanisms can have effects on the increase of degenerative changes in upper and lower intervertebral disc levels except the degenerative effects due to aging in OSAS patients. As it is known during sleep, repetitive episodes of airway occlusion, with consequent hypoxemia and hypercapnia and dramatic changes in intrathoracic pressure, elicit a wide variety of autonomic, hemodynamic, humoral, and neuroendocrine responses patients with OSAS [25]. Accordingly, we can suppose that the increase in facet joint degeneration gives rise to abnormal loading to intervertebral disc spaces, or changes in metabolic status in OSAS patient may play a role in increased cervical disc degeneration scores in the OSAS group. Interestingly, the electrophysiological studies of OSAS patients using motor evoked potentials by Transcranial Magnetic Stimulation (TMS) have found a global hypoexcitability of the stimulated motor cortex and a decrease in cortico-spinal conductivity [26,27]. Lanza et al. [27] offered TMS can be considered an additional tool for the understanding of clinical and pathophysiological aspects of sleep disorders, and possibly for the evaluation of the effect of therapy. As the descending motor pathways run primarily in the lateral columns of the spinal cord, coexistence of cervical disc degeneration and decrease in motor evoked potentials in OSAS patients, requires an understanding to differentiate clinically important signal changes.
Our findings showed considerably amounts of Grade 0 (0%), 1 (83.3%) and Grade 2 (16.7%) AAOJ degeneration in patients with OSAS whereas 36.7%, 60% and 3.3% consecutive Grade 0, 1 and 2 degenerative changes determined in control subjects. This article demonstrated that the prevelance of AAOJ degeneration was significantly higher in OSAS group. Previous studies have shown that degenerative changes of AAOJ may contribute to pain and limitation in motion [14,28]. Furthermore, besides the growing effect of age on degeneration, degeneration of the AAOJ may have an effect on potentiating injury in OSAS.
There are some limitations of our study. First, the community evaluated in present study consisted of patients who sustained a neck pain that required a cervical spine CT. This population does not necessarily reflect a general OSAS population and could bias our findings. However, the subjects of the control group also have a neck pain. Since we must take into account the radiation dose for the subjects with minimum level, we designed this study retrospectively. Prospective studies may be investigated for evaluation of the early degenerative changes and spinal cord lesion in randomly selected subjects from OSAS patients using magnetic resonance imaging. Second, the control subjects did not undergo polysomnography. According to their retrospective clinical histories, these subjects did not report sleep disorders.
In conclusion, this study indicates that patients with OSAS have higher degeneration of cervical spine in terms of degeneration in disc spaces, AAOJ and facet joints when compared to normal subjects. To our knowledge, this is the first study to document degenerative changes of cervical spine of OSAS patients.
We would like to emphasize that the presence of cervical vertebrae degeneration has to be considered when evaluating the clinical findings of patients with OSAS. We also think that the symptoms of disc and facet joint degeneration should be investigated prospectively in larger populations of patients with OSAS.