Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2014) Volume 4, Issue 2
Type 1 diabetes mellitus (T1DM) is associated with the development of severe complications including cardiovascular diseases, nephropathy, retinopathy and neuropathy. The peptide Angiotensin II (Ang II), the main effector molecule of the renin angiotensin system (RAS), has been widely investigated because it plays an important role in the pathogenesis of T1DM and evidence in the literature suggests the pharmacological blockade of the RAS components as a potential therapeutic strategy to minimize the deleterious effects of T1DM by improving metabolism control, renal and cardiovascular functions.Physical exercise can also contribute to avoid the complications of T1DM by enhancing metabolism of carbohydrates and lipids, peak oxygen consumption, vascular function, autonomic response and arterial blood pressure. Furthermore, the physical exercise is able to reduce the level of tissue RAS. Thus, part of the benefits of physical exercise for prevention and treatment of metabolic and cardiovascular diseases in T1DM may be mediated by the RAS. The present review aimed to discuss the evidence regarding the involvement of the RAS in the progression of T1DM, the relevance of physical exercise to the management of T1DM and the role of physical exercise to induce adaptations in the RAS.
<Keywords: Insulin-dependent diabetes mellitus, Pancreas, Insulin, Angiotensin II, Physical exercise
Type 1 diabetes mellitus (T1DM) is a form of diabetes mellitus that results from immunologic destruction of pancreatic ß-cells, leading to a deficiency in insulin production [1]. In this condition, glucose uptake stimulated by insulin is impaired in tissues such as skeletal muscle and adipose tissue, which can induce hyperglycemia and increase in lipid and protein catabolism [2]. In the short term, the consequences of these metabolic disturbances are higher production of ketone bodies and glucose in the liver, which may induce the progression of the disease [3]. Individuals with T1DM present classical symptoms such as polyphagia, polydipsia, polyuria and weight loss [4].
According to the American Diabetes Association [5], 5% of people with diabetes mellitus have the T1DM form, which is usually diagnosed in children and young adults. The prevalence of T1DM is much lower than the type 2 diabetes mellitus (the most common form), which may explain, in part, the low number of articles published in the literature regarding the prevention, treatment and mechanisms involved in T1DM complications compared with type 2 diabetes mellitus. However, severe complications including coronary heart disease, stroke, peripheral arterial disease, nephropathy, retinopathy, and possibly neuropathy and cardiomyopathy may occur in individuals with T1DM [3], resulting in higher morbidity and mortality related to the disease [6].
Different mechanisms can induce the progression of T1DM and it is known that humoral factors seem to affect the progression of T1DM complications directly [3]. In recent years, the peptide Angiotensin II (Ang II), the main effector molecule of the renin angiotensin system (RAS), has been widely investigated because it plays an important role in the pathogenesis of T1DM [7-9]. In fact, studies involving blockade of the RAS have shed some light on the contribution of the tissue-specific RAS activity to the complications of T1DM [10,11].
Insulin therapy, diet, and physical exercise have been the basis for the treatment of T1DM for the past 80 years [12]. The metabolic and cardiovascular adaptations induced by physical exercise may help in the prevention and treatment of T1DM [13], and part of the beneficial effects may be mediated by the modulation of local and systemic RAS activity [14,15]. However physical exercise in conjuction with insulin therapy should be well designed to avoid hyperglycemia and ketosis that can occur during and after the session of physical exercise. The present review aimed to discuss the evidence regarding the involvement of the RAS in the progression of T1DM, the relevance of physical exercise to the management of T1DM and the role of physical exercise to induce RAS adaptations.
The classical RAS consists of circulating renin, acting on angiotensinogen (AGT) to produce angiotensin I (Ang I), which in turn is converted into Ang II by angiotensin-converting enzyme (ACE). Ang II, the main effector of RAS, binds to angiotensin type 1 or type 2 receptors (AT1R and AT2R) in diverse target tissues including heart, pancreas, adrenal cortex, kidney, vascular smooth muscle, adipose tissue, skeletal muscle and brain. The RAS plays an important homeostatic function controlling blood volume and salt-water balance through vasoconstriction and sodium retention, thus affecting arterial blood pressure levels and tissue perfusion. Most of the actions of Ang II are mediated by AT1R, including vasoconstriction, pro-inflammatory, pro-oxidative, proliferative and hypertrophic effects [16].
The existence of local RAS has been demonstrated in different tissues, such as the heart [17], vessels [18], kidney [19,20], brain [21], liver [22,23] and pancreas [24]. AGT, renin, ACE, AT1 and AT2 receptors proteins are expressed in the pancreas [25,26] (Figure 1). However, the expression of AT1 receptor is limited to the pancreatic ß-cell. In addition, pro-renin mRNA was identified in reticular fibers of islets and perivascular connective tissue and pro-renin protein was located in ß-cells [27].
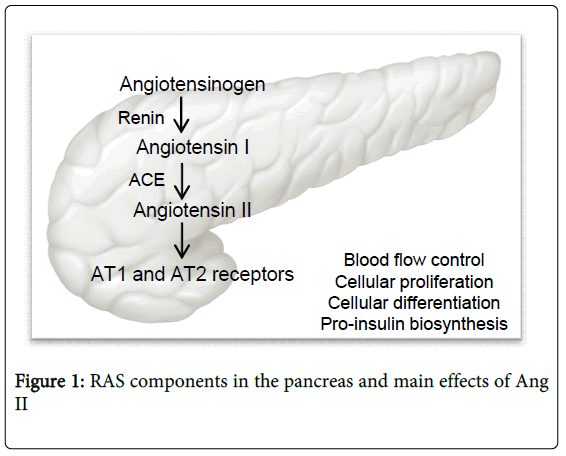
Figure 1: RAS components in the pancreas and main effects of Ang II
All RAS components are expressed in the pancreas. The starting point in the enzymatic pathway of the RAS is the angiotensinogen (AGT), which is cleaved by renin to form angiotensin I (Ang I). Ang I is converted into Ang II by angiotensin-converting enzyme (ACE), which binds to angiotensin type 1 or type 2 receptors (AT1R and AT2R). RAS has multiple functions in the pancreas.
In the pancreas, the RAS regulates local blood flow, pro-insulin biosynthesis, proliferation and differentiation of pancreatic cells (Figure 1). The hyperactivity of the RAS has been closely associated to insulin resistance [8], ß-cell dysfunction [26] and the development and progression of T1DM complications [10] Tikellis et al. [7] demonstrated that the activation of RAS in both type 1 and type 2 diabetes is accompanied by an augmentation in the oxidative stress, inflammation and free fatty acids levels, which potentially contribute to ß-cell dysfunction in diabetes. Indeed, in an experimental model of diabetes, RAS inhibition improved the function of ß-cells by decreasing oxidative stress, fibroses and apoptosis [28], which may improve islets structure and function, and reduce the T1DM complications [9]. The association between RAS and T1DM complications is summarized in Figure 2.
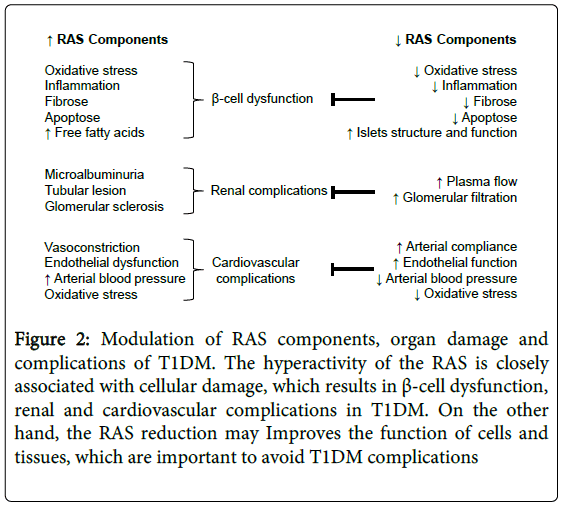
Figure 2: Modulation of RAS components, organ damage and complications of T1DM. The hyperactivity of the RAS is closely associated with cellular damage, which results in β-cell dysfunction, renal and cardiovascular complications in T1DM. On the other hand, the RAS reduction may Improves the function of cells and tissues, which are important to avoid T1DM complications
The effects of intracellular Ang II play a central role in the pathogenesis of T1DM by inducing inflammation, cell growth, mitogenesis, apoptosis, migration, differentiation, gene expression of bioactive substances and multiple intracellular signaling pathways responsible for tissue injury. Ang II may potentiate microalbuminuria [29] and tubular and glomerular lesions [30], which are associated with the development of diabetic nephropathy. Hyperglycemia seems to be a common condition that significantly enhances the production of intracellular Ang II as demonstrated by studies that found an increase in the Ang II synthesis in different cells exposed to high glucose [31,32]. In fact, hyperglycemia in T1DM increases RAS components (AGT, ACE, AT1R, Ang II) in pancreatic stellate cells [33], in human islets [34], in rat kidneys [35] and rat heart [36]. Vidotti et al. [37] showed an increase in the expression of AGT mRNA and in the Ang II synthesis in mesangial cells incubated in a medium with high glucose concentration, which may contribute to the glomerular sclerosis observed in diabetic nephropathy. Together, these data provide evidence regarding the involvement of the RAS in the progression of T1DM associated with hyperglycemia (Figure 2).
Pharmacological blockade of the RAS components through ACE inhibitors [11] and AT1 receptor antagonists [38] has been recommended as a therapeutic strategy to minimize the deleterious effects of diabetes by improving renal function (renal plasma flow and glomerular filtration) and cardiovascular function (increases in arterial compliance and endothelial function; reductions in arterial blood pressure) [39,40]. According to Oak and Cai [41], RAS down-regulation significantly reduces the incidence of vascular complications of diabetes. In an experimental model of T1DM (streptozotocin-induced diabetes), RAS blocked prevents the increase in Ang II levels in cardiac myocytes protecting against the oxidative stress and cardiac dysfunction [42]. Furthermore, the benefits can also be observed in the liver, where the glucose uptake was increases in response to insulin administration [43].
The identification of the RAS as a potential therapeutic target for prevention and treatment of the complications associated with diabetes opens an avenue for improving the quality of life of individuals with T1DM. However, it is important to consider that the association between the RAS and the progression of T1DM is complex, and pharmacological blockade seems to be efficient to improve the endocrine effects elicited by Ang II. Future studies are still necessary to better understand the mechanisms and possible repercussions associated with the activation/deactivation of intracellular tissue-specific RAS in the treatment of metabolic and cardiovascular diseases.
The goals of treating T1DM are to control blood glucose levels and decrease the risk of developing future complications. Furthermore, an efficient treatment should allow proper growth and development, and promote quality of life, Including nutritional strategies and physical exercise. In this context, the use of physical exercise as a non-pharmacological adjuvant therapy to treat T1DM has been extensively recommended because it can enhance the metabolic control and protect against the complications of T1DM [44,45].
Although the complications of T1DM are typically described in target organs such as heart, kidney, retina, vessels, evidence in the literature also demonstrates that disturbances in the skeletal muscle collectively designed as diabetic myopathy are associated with the complications of T1DM [46]. Damages in skeletal muscle oxidative metabolism, reduction in the number of capillaries and type 1 muscle fibers, muscular atrophy and intolerance to physical exercise are presented in diabetic myopathy and can be associated with poor metabolic control and reduced quality of life [46-48]. In addition, raises in White Adipose Tissue (WAT) lipolytic activity are observed in T1DM, which result in high free fatty acid levels and may lead to ketosis and lipotoxicity in peripheral tissues [49].
The benefits of physical exercise are extensive (Figure 3). Evidence in the literature showed that physical exercise can enhance oxidative metabolism and the ability of skeletal muscle to handle the excess of free fatty acids, which can contribute to better metabolic control and to prevent diabetic myopathy. The metabolic effects of physical exercise are extensively described in the literature, including increased levels of oxidative enzymes activity [50,51], fatty acids carrier proteins in skeletal muscle [52], mitochondrial biogenesis [53,54], and augment in type 1 muscle fibers, which are predominantly oxidative [55]. These adaptations favor fatty acid oxidation instead of storage, which can prevent lipotoxicity and metabolic acidosis associated with the excess of ketone bodies.
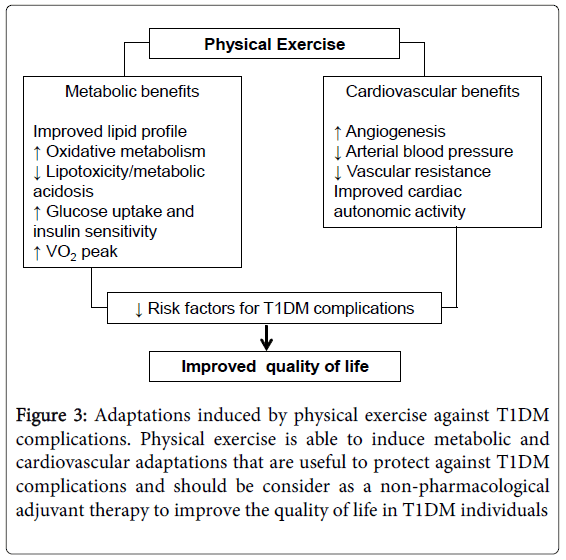
Figure 3: Adaptations induced by physical exercise against T1DM complications. Physical exercise is able to induce metabolic and cardiovascular adaptations that are useful to protect against T1DM complications and should be consider as a non-pharmacological adjuvant therapy to improve the quality of life in T1DM individuals
The benefits of physical exercise are also observed in glucose metabolism. Evidence in the literature shows increases in glucose uptake and insulin sensitivity in skeletal muscle and white adipose tissue induced by physical exercise [6,56]. During skeletal muscle contractions, glucose transport mediated by glucose transport proteins (Glut 4) can be stimulated by AMP-activated protein kinase (AMPK), which is a central sensor of cell energy states and regulates the balance between substrates oxidation and storage [57,58].
The activation of AMPK is induced by the augment in cellular energy turnover associated with a reduction in ATP/AMP and ATP/ADP ratios. In its activated state, AMPK stimulates glucose and lipid catabolism and prevents the expression of lipogenic enzymes such as FAS (fatty acid synthase) and ACC (acetyl-CoA carboxylase) in WAT and skeletal muscle [58]. Reductions in AMPK activity were observed in WAT [59], skeletal muscle [60] and liver [61] of obese and diabetic rodents and humans, suggesting that impaired AMPK activity can be associated with insulin resistance in many peripheral tissues [62]. In contrast, it has been shown that physical training activates AMPK in adipose tissue [63] and skeletal muscle [64], which improves the rates of lipolysis and free fatty acid delivery into the mitochondria [63,65], enhances insulin sensitivity and reduces glucose levels [66,67]. In addition, AMPK increases the expression of genes involved in angiogenesis and mitochondrial enzymes production such as citrate synthase and cytochrome c oxidase in the skeletal muscle [68].
According to Hayat et al. [69], 80% of deaths in diabetic patients are associated with cardiovascular diseases that can be induced by atherosclerosis, hypertension, chronic hyperglycemia, microvascular disease and autonomic neuropathy. In this context, the T1DM patient needs not only to improve the metabolism control but also prevent hypertension and atherosclerosis. Effective drugs are useful to treat dyslipidemia and hypertension, however physical exercise can contribute to improving the health status. Laaksonen et al. [70] demonstrated that patients with T1DM submitted to 12- to 16-wk aerobic exercise training have a significantly augmented oxygen consumption peak (VO2 peak) and an improved lipid profile (decrease in total and low-density lipoprotein (LDL) cholesterol and apolipoprotein (apo) B and increase in the high-density lipoprotein (HDL)/apo A-I ratio). While body mass index, percent body fat and hemoglobin A1c did not change, physical exercise was able to reduce risk factors responsible for T1DM complications.
It is well described that increases in physical exercise produce beneficial effects on the cardiovascular system including decreases in arterial blood pressure [71], vascular resistance [72] and sympathetic nervous system activity [73]. Lucini et al. [74] observed positive autonomic effects in T1DM adolescents submitted to physical exercise. Recently, Shin et al. [75] showed a significant reduction in arterial blood pressure and improvement in cardiac autonomic nervous system activity in T1DM children after a period of physical exercise, suggesting that physical exercise may play a primary role in the management and treatment of autonomic neuropathy among individuals with T1DM.
Evidence in the literature shows that physical exercise is able to reduce the level of tissue RAS, and thus part of the benefits of physical exercise to prevent and treat metabolic and cardiovascular diseases may be mediated by the RAS [76,77]. Limited data are available regarding the effects of physical exercise on RAS in T1DM, however there is evidence that the modulation of RAS by physical exercise can contribute to possible mechanisms involved in the prevention and treatment of T1DM complications.
Evangelista and Krieger [50] studied the effect of swimming training in transgenic mice harboring one to four functional copies of the ACE gene, which are correlated with the level of tissue and systemic ACE. Mice with a lower ACE level (only 1 copy of the gene) have better improved citrate synthase activity enzyme compared to mice with a higher ACE level (4 copies of the gene). The association between lower ACE levels and higher efficiency of skeletal muscle metabolism after physical training is described in the literature [78,79] and the higher oxidative response shown by mice with one copy of the ACE gene is consistent with previous evidence correlating improved muscular capacity with aerobic physical training associated with the insertion/deletion (I/D) polymorphism of ACE gene (genotype II) and low ACE activity [78-80]. Interestingly, these same transgenic animals (streptozotocin-induced diabetes) submitted to physical training, only mice with one copy of the ACE gene show a significant reduction in fasting blood glucose, suggesting that the effect of physical training on metabolism control in T1DM may be associated with the RAS modulation (data not published).
The adaptations induced by physical exercise have been extensively studied in patients with cardiovascular disease and the association between RAS activity and functional capacity is well established. The polymorphism of ACE gene and insulin sensitivity response after physical exercise in hypertensive subjects were studied by Dengel et al. [15] found that individuals with genotypes II (low ACE level) were more sensitive to insulin than individuals with DD genotype (high ACE level). Moreover, physical exercise induces significant reductions in blood pressure only in individuals with genotypes II and ID and not in individuals with DD genotype [15]. In an experimental model of heart failure, Kemi et al. [81] observed that losartan (AT1 receptor antagonist) treatment paired with physical exercise reduces the endothelial dysfunction assessed in aortic segments and improves exercise capacity. Agarwal et al. [14] showed that physical exercise prevents renal oxidative stress, inflammation and increase in circulating Ang II levels in an experimental model of hypertension. These studies revealed that physical exercise combined with reduction in RAS activity can be a good strategy for the prevention of T1DM complications.
The potential of Ang II to increase T1DM complications is clear, but the intrinsic mechanisms need to be better understood. A possible mechanism discussed in the literature is the ability of Ang II to inhibit AMPK activity, resulting in changes in the energy metabolism of cells [82,83]. Decreases in AMPK are associated with the metabolic impairment observed in diabetes and obesity [63,84], but can be reversed by the activation of AMPK. In fact, the activation of renal AMPK inhibits the action of lipogenic enzymes and prevents fat accumulation, reduces oxidative stress and apoptosis [84,85], which can reduce renal damage. Moreover, increases in AMPK in adipose tissue by physical exercise was associated with the improvement of glucose metabolism and the level of serum adiponectin, an important protein secreted by adipose tissue that regulates insulin sensitivity and tissue inflammation [63].
The use of physical exercise as an adjuvant tool in the treatment of T1DM has been studied in the literature. According to the American Diabetes Associaton [86], all levels of physical exercise, including leisure activities, recreational sports, and competitive professional performance, can be performed by people with T1DM who do not have complications, have good blood glucose control and are able to adjust their therapeutic regimens accordingly. However, the great problem for T1DM patients performing physical exercise is the risk of hypoglycemia during and after exercise [12,87,88], which can be influenced by factors such as duration and intensity of physical exercise, level of metabolic control, type and dose of insulin administered before exercise, site of injection, timing of previous insulin injection and food intake relative to the exercise, as described in an elegant review about the management of insulin therapy during exercise in individuals with T1DM [12]. A brief summary with considerations for exercise prescription is described in the Table 1.
| Goals | Procedures |
|---|---|
| Blood glucose control | Design of physical exercise duration and intensity Insulin therapy adjustment: type and dose used before exercise, site of injection, timing of previous insulin administration and food intake relative to the exercise Self-monitoring of blood glucose level: before, during and after physical exercise |
| Diagnostic studies | Evaluation of the health status to identify risk factorfor coronary artery disease, peripheral arterial disease, retinopathy, nephropathy and neuropathy |
Table 1: Considerations for physical exercise prescription for T1DM individuals
Reductions in blood glucose can be associated with physical exercise intensity in individuals with T1DM. Guelfi et al. [88] observed that intermittent high-intensity exercise (activity involving short repeated bouts of intense activity) on a bicycle ergometer over a 30 min period, causes smaller decreases in blood glucose compared with moderate- intensity exercise during physical exercise and recovery in T1DM individuals that were on a multiple or twice-daily injection treatments with short-acting insulin and intermediate-acting insulin at bedtime. The possible mechanisms involved in these responses were the high increase in endogenous glucose production during exercise and diminished glucose utilization during exercise and recovery. Furthermore, the intensity of physical exercise can improve the level of catecholamine and growth hormone that could blunt the fall in glucose concentrations [88].
The risk of hypoglycemia associated with postprandial physical exercise can be reduced in T1DM individuals on intensive insulin therapy with the basal-bolus insulin regimen with ultralene (basal insulin) and insulin lispro (premeal insulin) by decreasing the premeal insulin administration. Rabasa-Lhoret et al. [87] showed that full dose of insulin lispro increases the risk of hypoglycemia associated with physical exercise, independent of the intensity and duration. However, when the dose of premeal insulin was reduced by 50% and 75%, the incidence of exercise-induced hypoglycemia was significantly decreased in three different intensities of exercise (25%, 50% and 75% VO2max).
The self-monitoring of blood glucose level is strongly recommended for T1DM patients engaging in physical exercise [89]. Pre-exercise blood glucose levels are individualized, however it is recommended to keep fasting glucose above 100 mg/dl (5.6 mmol/L) and below 250mg/dl (13.9mmol/L, if ketosis is present) to 300mg/dl (16.7 mmol/L, with no ketosis). Physical exercise should be delayed when blood glucose levels are above 300mg/dl whether or not ketosis is present. Moreover, if glucose levels are below 100 mg/dl, the consumption of carbohydrate is recommended. During and after physical exercise, blood glucose monitoring must be continuous and carbohydrate-based foods should be readily available to avoid hypoglycemia.
Considering that during physical exercise, skeletal muscle contractions increase glucose uptake to produce energy, it is recommended to avoid insulin injection in body regions which are involved in the exercise [89]. In fact, Koivisto et al. [90] observed that patients receiving insulin injections in the arm or abdomen have diminished exercise-induced hypoglycemia compared with patients who received the insulin injection in the leg.
General recommendations for physical exercise can be obtained in published studies and position statements, however the ideal adjustments must be made individually. Furthermore, prior to engaging in any physical exercise program, an medical examination of physical condition and medical history should be conducted, with special consideration for symptoms and signs associated with T1DM such as risk factor for coronary artery disease, vascular disease, neuropathy, nephropathy, retinopaphy and the time of disease.
The data reported in this review support the hypothesis that the RAS plays a key role in the development and progression of T1DM, and that the metabolic and cardiovascular effects of physical exercise may confer additional health benefits to individuals with T1DM and may be a well established therapeutic tool to prevent and to treat the complications associated with T1DM. Furthermore, considering that physical exercise is able to reduce the level of tissue RAS, the benefits induced by physical exercise may be partly mediated by the RAS. However, future studies are still necessary to unveil the effects of physical exercise on RAS in individuals with T1DM.
The studies described in this review were supported by grant from São Paulo Research Foundation (FAPESP) to F.S. Evangelista (#2001/08592-7; #2009/52904-5 and #2011/02126-6). We thank Dr. Laura A. Szymanski for the English proof-reading of this manuscript.