Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2015) Volume 3, Issue 2
Superficial vein thrombosis is an integral part of venous thromboembolism (VTE) together with deep vein thrombosis (DVT) and pulmonary embolism (PE). The incidence of SVT is 1.6 per 1000 persons per year. The incidence of DVT is about 1.0 per 1000 persons per year in the general population, 1.8 per 1000 persons per year at age 65 to 69 years and 3.1 per 1000 persons per year at age 85 to 89 years. First episodes of DVT are in two-thirds of cases elicited by risk factors, including varicose veins, cancer, pregnancy/ postpartum, oral contraceptives below the age of 50 years, immobility or surgery. Pain and tenderness in the calf and popliteal fossa may occur resulting from other conditions labeled as alternative diagnosis (AD) including Baker’s cyst, ruptured Baker’s cyst, torn plantaris tendon, hematoma, or muscle tears or pulls. The requirement for a safe diagnostic strategy of deep vein thrombosis (DVT) should be based on an objective post-test incidence of venous thromboembolism (VTE) of less than 0.1% with a negative predictive value for exclusion of DVT of 99.99% during 3 months follow-up. Modification of the Wells score by elimination of the “minus 2 points” for AD is mandatory and will improve clinical score assessment for DVT suspicion in the primary care and outpatient medical diagnostic setting. Compression ultrasonography (CUS) for proximal DVT overlooks distal DVT and is not cost-effective enough to rule in or out DVT. Complete CUS (CCUS) does pick up alternative diagnoses (AD) like Bakers cyst, muscle hematomas, old DVT, and superficial vein thrombosis (SVT). ADs with a negative CCUS include leg edema, varices erysipelas are easily picked up by physical examination. The sequential use of CCUS followed by quantitative rapid ELISA-D-dimer testing and modified Wells’ clinical score assessment is cost-effective and objective diagnostic algorithm that can safely and effectively exclude and diagnose both DVT and AD in patients with suspected DVT. About 10 to 30% of patients with DVT develop overt PTS (CEAP, C4,5) at one year post-DVT. DVT has a recurrence rate of about 20% to 30% after 5 years. A scoring system for lower extremity venous thrombosis (LET) extension on CCUS related to therapeutic implications is presented to prevent DVT recurrence and the post-thrombotic syndrome (PTS).
Keywords: Deep vein thrombosis; Complete compression ultrasonography; Alternative diagnosis; D-dimer; Clinical score; Primary care medicine
The incidence of superficial thrombophlebitis (SVT) is approximately 1.6 per 1000 persons per year. Several studies have confirmed the association of SVT and VTE. In a systematic review of patients with SVT, 6% to 44% of cases was associated with deep vein thrombosis (DVT), 20% to 33% with asymptomatic pulmonary embolism (PE) and 2% to 13% with symptomatic PE. Assessment of risk factor in the MEGA study a history of clinical SVT was associated with a 6.3-fold risk of DVT and a 3.9 risk of PE. In a study of 263 SVT patients, 30 (11.4%) developed DVT. Among 125 patients with SVT located in the great saphena vein, 16.8% developed DVT. Out of 138 patients with isolated SVT below the knee only 4.5% developed DVT. In a lower limb ultrasound study in 2646 patients 36 (9.3%) of the patients had combined DVT and PTS. These data indicate that primary SVT should be considered an integral part of DVT. The presence of inherited hypercoagulability or venous thrombophilia in both SVT and DVT strongly supports a similar etiology and pathphysiology. In… patients with primar SVT hereditary protein C and s deficiency was detected in 6.45% in the absence of DVT and in 62.5% in SVT patient who had developed DVT. In our experience hereditary heterozygous antithrombin defiencoiency (AT) is associated with a high risk on DVT and PE not preceded by SVT. Congenital protein C (PC) or protein S (PS) deficiency in 27 DVT patients (15 males, 12 females) in 6 unrelated Dutch families had a history of SVT 19 cases (70%) as the hall mark of congenital PC/PS deficiency. The prevalence of FV Leiden, FII A20210 mutation, and PC or PS deficiency in 63 evaluated SVT patients was 16%, 906% and 10% respectively (total 36%) as compared to 3%, 2.4% and 0.6% in 537 controls. The incidence of inherited thrombophilic risk factors in patients with a first DVT is high (31%) as compared to 5 to 6% in the general population (Table 1). In 1668 patients with a first DVT in the Leiden prospective study the incidence of congenital thrombophilia was 25%. In this study 417 (25%) of 1668 patients with a first DVT were on oral contraceptives below the age of 50 years. In 400 Czech young women with VTE on oral contraceptives (distal DVT 58%, proximal DVT 16%, PE 5%, thrombosis at unusual sites 20%) inherited thrombophilia was diagnosed in 195 (49%): FV Leiden 35% FIIA20210 mutation 5%,AT,PC PS deficiency 3.6% and antiphopholipid syndrome 5.3%. We conclude that thrombophilia screening is manadatory in SVT and DVT patients and in women on contraceptive pills in particular for the education of clinicians abling them to much better counsel their SVT and DVT patients and their relatives.
| Inherited venous thrombophilia | Prevalence in general population | Prevalence in population with VTE | RR | Relative risk RR contribution OAC pill |
| Antithrombin AT | 0.07-0.16 | 1-3 rare | 20 | |
| Protein C | 0.2-0.4 | 3-5 less rare | 10 | |
| Protein S | 0.03-0.13 | 1-5rare | 10 | |
| FV Leiden | 3-15 | 20% frequent | 5 | 20fold-35 fold |
| Prothrombin | 1-2 | 4-7 | 2-3 | |
| Total venous thrombophilia | 5-6% | 31% frequent | ||
| Elevated F 8/VVF | 11 | 25% frequent | 5 | |
| Main characteristics for 1St DVT | Number | % | ||
| Varicose veins at Diagnosis | 470 | 28% | ||
| Malignancy | 137 | 8% | ||
| Surgery <3months | 357 | 21% | ||
| Minor injury Plaster cast, 3months | 405 | 24% | ||
| Oral anticonceptive pill | 417 | 25% | ||
| Hormonal replacement | 39 | 13% | ||
| Idiopathic DVT | 389 | 24% | ||
| FV leiden Mutation | 315 | 19% | ||
| Prothrombin 20210 mutation | 92 | 6% | ||
| Venous thrombophilia FV Leiden 20210 | 25& | |||
Table 1: Inherited and acquired risk factors for a first deep vein thrombosis: DVT.
Epidemiology
DVT has an annual incidence of 0.2% in the urban population [1]. The disease is rare in children under 15 year of age, but its frequency increases with age, with an incidence of about 1.0 per 1000 persons per year in the general population, 1.8 per 1000 persons per year at age 65 to 69 years and 3.1 per 1000 persons per year at age 85 to 89 years [2,3]. First-time episodes of DVT are in two-thirds of cases elicited by risk factors, including varicose veins, cancer, pregnancy/ postpartum, oral contraceptives below the age of 50 years, immobility or surgery (Table 1) [2-8]. In the past the incidence of post-thrombotic syndrome (PTS) was found to be approximately 35 to 70% at 3 years in proximal DVT and rather uncommon in calf vein thrombosis (CVT) [4,5]. Randomized controlled studies with treatment of proximal DVT by adequate anticoagulation, early mobilization and long-term elastic compression for symptomatic PTS show that skin changes or ulceration (severe PTS) develop in 4-8% during long-term follow-up [5,8,9]. In a recent large management study of 1618 patients with a first DVT, the 1 year cumulative risk of PTS was 31% in women and 17% in men (overall 25% and severe 7%) [9]. The prevalence of DVT is equal in man and women, but seems to be slightly higher in young females below the age of 50 years [9]. The prevalence of DVT is comparable in black and white adults and is low in Asian populations. The risk of recurrence of venous thromboembolism is about 60% higher in men compared to women in one study [5], but equal in another large study [10].
Pathogenesis
In 1856, Virchow postulated that the main causes of thrombus formation consist of damage to the vessel wall, alterations in flow, and hypercoagulability. This conceptual model is called ‘Virchow’s triad’ and still valid today [11]. At time of thrombus formation in a leg vein which takes place under conditions as defined by Virchow, increased thrombin (IIa) generation converts fibrinogen into a fibrin clot (Figures 1 and 2) . The maintenance of the fluidity and circulation of the blood and its ability of anticoagulant factors to prevent blood to clot (thrombosis) are essential for the maintenance of life. The extremely complex homeostatic mechanisms (Figure 1) of anticoagulant and procoagulant factors in concerted actions with the blood vessel endothelial cells on top of the fibrinolytic system (Figure 2) counteracts or stabilizes the fluidity of circulating blood to prevent thrombosis (fibrin formation). The anticoagulant, procoagulant and fibrinolytic systems depend upon consecutive enzyme activity with activators and inhibitors finely balanced at every stage (Figures 1 and 2). Alterations in blood coagulability, platelet reactivity and agglutinating power, with changes in blood flow and endothelial cell damage, are the precursors of intravenous thrombosis. Of these, the loss of normal function of the vascular endothelium may be of primary importance. A number of other hereditary thrombophilia factors and acquired thrombophilic conditions and elevated FVIII predispose to venous thrombosis (Figure 1 and Table 1) [12-15]. These include protein C and S (PC, PS) deficiency, antithrombin (AT) deficiency, activated protein C resistance (which is usually associated with Factor V Leiden genetic abnormality) factor II G20210A mutation and lupus anticoagulant [2,3,13-15]. Anticardiolipin antibody is also now recognized as an important cause of thrombosis [16-18]. Screening for these congenital thrombophilic factors as well as anticardiolipin antibody should be performed in patients having sporadic or recurrent thrombosis [19-21]. The use of oral contraceptive pill is a common risk factor for venous thromboembolism in women of reproductive age and surgical operations and pregnancy remain important triggers [22-40]. Prolonged immobility as in long-haul flights and hormonal influences, such as the contraceptive pill, are also well-documented risk factors [9,20,21].
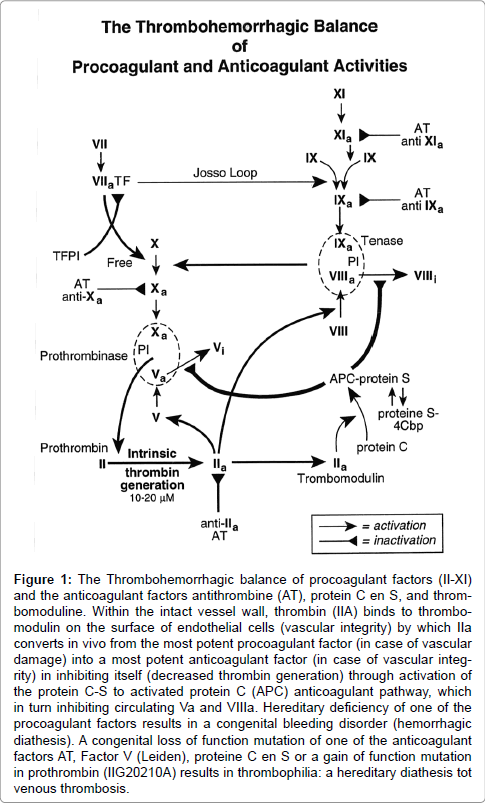
Figure 1: The Thrombohemorrhagic balance of procoagulant factors (II-XI) and the anticoagulant factors antithrombine (AT), protein C en S, and thrombomoduline. Within the intact vessel wall, thrombin (IIA) binds to thrombomodulin on the surface of endothelial cells (vascular integrity) by which IIa converts in vivo from the most potent procoagulant factor (in case of vascular damage) into a most potent anticoagulant factor (in case of vascular integrity) in inhibiting itself (decreased thrombin generation) through activation of the protein C-S to activated protein C (APC) anticoagulant pathway, which in turn inhibiting circulating Va and VIIIa. Hereditary deficiency of one of the procoagulant factors results in a congenital bleeding disorder (hemorrhagic diathesis). A congenital loss of function mutation of one of the anticoagulant factors AT, Factor V (Leiden), proteine C en S or a gain of function mutation in prothrombin (IIG20210A) results in thrombophilia: a hereditary diathesis tot venous thrombosis.
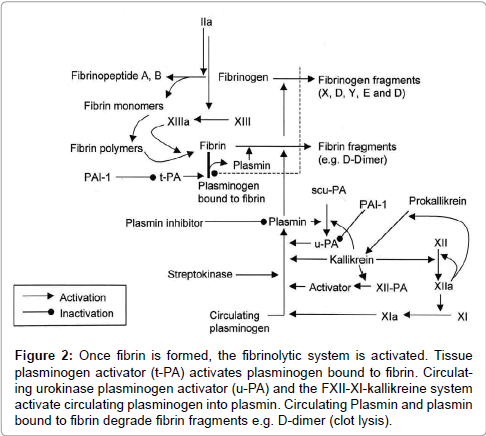
Figure 2: Once fibrin is formed, the fibrinolytic system is activated. Tissue plasminogen activator (t-PA) activates plasminogen bound to fibrin. Circulating urokinase plasminogen activator (u-PA) and the FXII-XI-kallikreine system activate circulating plasminogen into plasmin. Circulating Plasmin and plasmin bound to fibrin degrade fibrin fragments e.g. D-dimer (clot lysis).
Clinical features
The onset of a thrombosis is often ‘silent’ and may remain so. Symptomatic DVT or CVT may be the tip of a “clotted iceberg”. The cause of DVT may be idiopathic or provoked usually in the context of surgery, trauma, pregnancy and post-partum period. It commonly occurs at or about day 7 to 10 days after a surgical operation, parturition or the onset of an acute infection, concomitant with a rise in fibrinogen and platelet count. Between one-third and two-thirds of patients complain of some swelling and leg pain, usually in the calf [4]. An iliac vein thrombosis should be suspected if the whole leg is swollen and dusky in the absence of pain or cramps in the calf. Direct pressure on the calf muscles or over the course of the deep veins usually elicits direct tenderness in patients with suspected DVT or CVT. There may be a cyanotic hue to the leg and visuable superficial venous dilatation. The temperature of the leg may be raised, and edema of one ankle is an important physical sign. However, chest pain or even cardiac arrest from pulmonary embolism may be the first presentation of a DVT. Pulmonary hypertension may follow repeated small emboli, and is associated with the development of progressive dyspneu.
Differential diagnosis
Estimates of clinical score as low, moderate, and high for the probability of proximal DVT, based on medical history and physical examination, has been advocated as the first step when DVT is suspected (Table 2). The diagnostic differentiation between DVT and alternative diagnosis (AD) by physical examination alone is problematic in routine daily practice indicating the need of objective testing by CUS to rule in and out DVT and AD. Pain and tenderness in the calf and popliteal fossa may occur resulting from other conditions labeled as alternative diagnosis (AD) including Baker’s cyst, ruptured Baker’s cyst, torn plantaris tendon, hematoma, or muscle tears or pulls. Cutaneous infection (e.g. erysipelas, cellulitis), lymphoedema, venous reflux, specially dermatitis, peripheral arterial disease, neurological and rheumatological causes should also be differentiated from DVT. Physicians in the primary care and hospital setting are faced with a extensive co-morbidity profile in patients with deep vein thrombosis (DVT) or pulmonary embolism (PE) due to a broad spectrum of disease related risk factors for DVT or venous thromboembolism (VTE) (Table 3) indicating the need to treat not only DVT but also the underlying disease to reduce the risk of DVT complications and recurrence as much as possible [2,3,9,14].
| Clinical feature | Score |
| Active cancer treatment ongoing or within previous 6 months or palliative | 1 |
| Paralysis, paresis, or recent plaster immobilization of the lower leg(s) | 1 |
| Recent immobilization for more than 3 days or major surgery within last 4 weeks | 1 |
| Localized tenderness/pain along the distribution of the deep venous system | 1 |
| Entire leg swollen | 1 |
| Calf swelling by more than 2 cm when compared with the asymptomatic leg (measured 10 cm below tibial tuberosity) | 1 |
| Pitting oedema more pronounced in the symptomatic leg | 1 |
| Collateral superficial veins (nonvaricose) | 1 |
| Total Rotterdam DVT score | 8 |
| Score 0 (asymptomatic)=low, score 1 or 2=moderate, score 3 or more=high |
Table 2: The Rotterdam modification (16,17) of the Wells’ score list (15) for predicting pretest probability for DVT.
Congenital Risk Factors for DVT (Thrombophilia)
The risk of VTE in women with factor V Leiden is 5-6 fold higher in pregnancy [20]. The prevalence of different inherited thrombophilia in the general population and in patients with VTE and its calculated relative risk (RR) are summarized in Table 1. The frequency of hereditary thrombophilia in patients with confirmed idiopathic thrombosis occurring outside the clinical setting of surgery, trauma, or cancer is approximately 25%. The most common genetic predisposition in Caucasians is activated Protein C (APC) resistance, which is caused by the Factor V Leiden mutation in about 90%. Another cause is prothrombin G20210A gene mutation. Deficiency of physiological anticoagulant factors include deficiency of antithrombin (AT), Protein C (PC) or Protein S (PS), or heparin cofactor II. Combined deficiencies of Factor V Leiden, PC, PS, AT or the prothrombin mutation G20210A have been frequently described and they lead to a higher risk of thrombosis (20). There is an important interaction of Factor V and Factor II that leads to true synergistic potentiation with other transient risk factors for VTE such as pregnancy and oral contraceptives (12.20).
Oral contraceptives in heterozygotes for Factor V Leiden mutation increases the risk of VTE by ≈20-fold (95% CI: 4-29-4.3) (26) to ≈35- fold (95% CI: 7.8-154) [27]. This risk is further increased in users of third generation oral contraceptives to ≈50-fold compared with nonusers without the mutation [27,28]. Heterozygotes for prothrombin (Factor II) variant (G20210A) on oral contraceptives have an ≈16- fold increased risk for VTE compared to an ≈6-fold increased risk of non-users (26). This variant may carry a higher ≈150-fold risk (95% CI:31-711) for the rare condition of cerebral vein thrombosis with the use of oral contraceptives [30-32]. For rare inherited thrombophilic conditions such as Protein C, Protein S or antithrombin deficiency from retrospective case review-type analyses [33-35]. Oral contraception is discouraged. Elevated Factor VIII coagulant levels (VIII:C) levels have been associated with an ≈4-fold increased risk of VTE [36-39] and this appears to increase to ≈10-fold in oral contractive users [37]. Women with thrombophilia are more likely to develop VTE early in their course of oral contraceptive use. The risk is increased 19-fold during the first 6 months and 11-fold during the first year [40].
FVIII:C, ABO blood group and DVT
Genetically defined ABO blood group influences FVIII:Coagulant (FVIII:C) levels such that both FVIII:C and von Willebrand factor (VWF) levels are significantly lower in individuals with blood group O as compared to non-O bloodgroup [41] .Blood group O blood individuals are at greater risk for bleeding and may be at lower risk for venous thrombosis. High levels of VWF and FVIII:C are associated with thrombosis risk. Thrombosis and FVIII:C levels increase with age. VWF is the carrier protein of FVIII:C. the ratio of FVIII:C and VWF equals one in controls and thrombosis patients [42,43]. The clinical relevance of ABO blood group for the risk of venous thrombosis has been evaluated in 591 patients with suspected deep vein thrombosis or pulmonary embolism (venous thromboembolism: VTE) subdivided in 355 patients with VTE, and 236 without VTE. The distribution of the blood group ABO-genotypes was significantly different with higher frequency of non-O blood group in the VTE group and higher frequency of the O-bloodgroup in the non-VTE group (O-blood group 53% in VTE and 61.8% in non-VTE group, P=<0.001) [43]. In the VTE group, mean values for FVIII:C and VWF levels in the O blood group were 122 ± 39 and 123 ± 42 IU/dL respectively, and in the non-O blood group 160 ± 45 and 179 ± 57 respectively. In the non-VTE, mean values mean values of 109 and 103 IU/dl in the O blood group and 130 and 134 IU/dl respectively in the non-O blood group. These two clinical research studies [42,43] can readily explain the higher incidences of non-O blood group in patients with venous thrombosis and in symptomatic venous thrombophilia patients including FV-Leiden mutation [44,45].
Accurate diagnosis is mandatory in patients with suspected DVT, as an untreated thrombus may lead to pulmonary embolism. Besides treatment with anticoagulats in the absence of thrombosis is irresponsible [46-48]. Because only a quarter of patients with suspected DVT actually has the disorder, it is important to safely rule out thrombosis.
Phlebography is invasive, is inconclusive in 4 to 12% of cases, overlooks alternative diagnoses like Bakers cyst and many others. A normal venogram of the leg veins in patients with suspected DVT excludes both proximal and distal DVT irrespective of clinical score with a negative predictive value (NPV) of 98.1 to 99% [47,48]. In a prospective study of 562 consecutive symptomatic patients with a first deep vein thrombosis in 35%, the distribution and extent of DVT was popliteal in 10%, popliteal-femoral in 42%, popliteal-femoral and common femoral vein in 5%, all proximal veins (popliteal femoral and common femoral) in 35% and proximal femoral or iliac vein in 8% (Figure 3) (49). Phlebography is the gold standard to exclude and diagnose DVT in randomized clinical trials and do pick up asymptomatic and symptomatic early stage distal and proximal DVT (50). Due to its invasive nature phlebography has not become a routine test for DVT diagnosis and exclusion, and has been replaced by compression ultrasonography (CUS) [49,50].
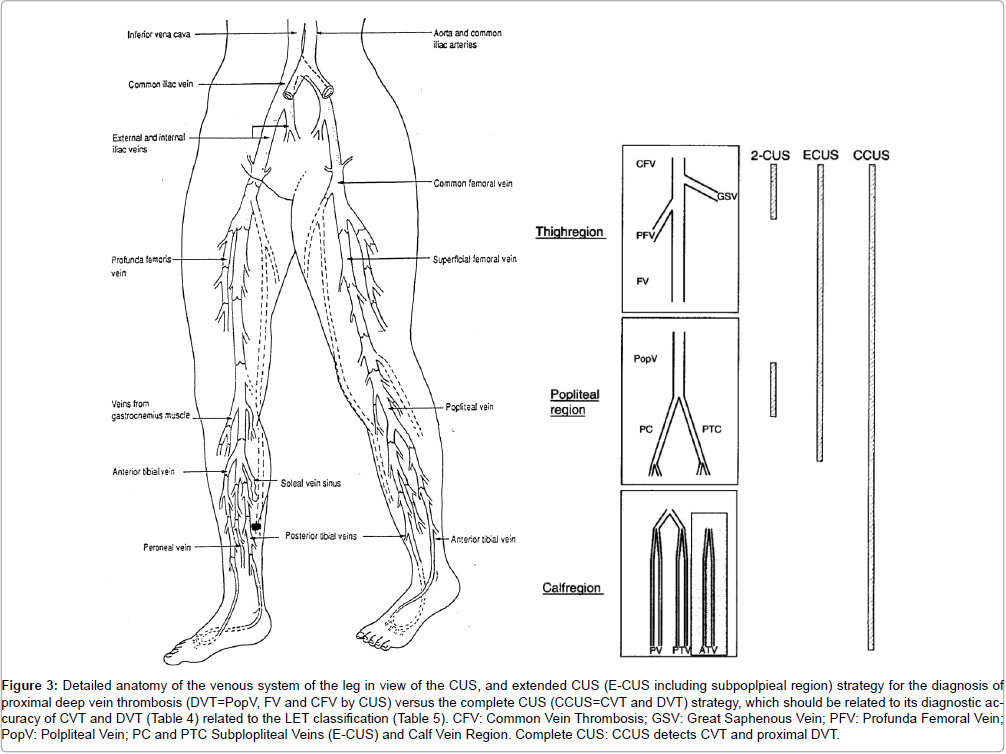
Figure 3: Detailed anatomy of the venous system of the leg in view of the CUS, and extended CUS (E-CUS including subpoplpieal region) strategy for the diagnosis of proximal deep vein thrombosis (DVT=PopV, FV and CFV by CUS) versus the complete CUS (CCUS=CVT and DVT) strategy, which should be related to its diagnostic accuracy of CVT and DVT (Table 4) related to the LET classification (Table 5). CFV: Common Vein Thrombosis; GSV: Great Saphenous Vein; PFV: Profunda Femoral Vein; PopV: Polpliteal Vein; PC and PTC Subplopliteal Veins (E-CUS) and Calf Vein Region. Complete CUS: CCUS detects CVT and proximal DVT.
As compared to phlebography as the reference gold standard to exclude and diagnose proximal DVT, the sensitivity of compression ultrasound (CUS) is 97% for proximal DVT [50]. CUS has many advantages over phlebography [49-51]. It is noninvasive, simple, easy to repeat, relatively inexpensive, and free of complications. It is safe to limit CUS estimation to the sub-popliteal, popliteal, and femoral veins for the diagnosis of symptomatic proximal DVT [49,50], but there are two main pitfalls (disadvantages) of proximal CUS [51]. First, calf vein thrombosis will be overlooked by CUS in the popliteal and femoral region. About one fourth to one third of calf vein thrombosis (CVT) may progress to proximal DVT within one week indicating the need to repeat CUS after one week. Second, isolated thrombi in the iliac and femoral veins within the adductor canal are relatively rare but difficult to detect and therefore overlooked by CUS in symptomatic patients with suspected DVT (Figure 3). In 1072 outpatients with a first suspicion of DVT in 5 management studies, the incidence of DVT on a venogram ranged from 26 to 46% for proximal DVT (popliteal and upper leg) and from 4 to 10% for CVT [48,51]. About a fourth of CVT extends into the proximal veins within a few days to 1 week. In 1998, Cogo et al and others extended CUS to all segments of the common femoral, femoral poplplitea and subpopliteal regin (E-CUS, Figure 4) [51,52]. After a first negative CUS overlooking CVT in routine daily practice, a repeated CUS iin prospective management studies will become positive in 2 to 3% within 1 week [53]. Five management studies indeed showed that the posttest incidence of VTE after a first negative CUS ranged from 1.7 to 3.0% indicating a NPV 98.3 to 97% [48,50].
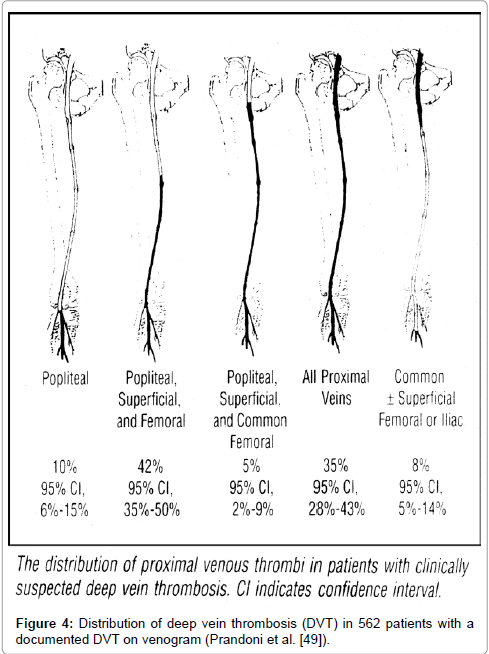
Figure 4: Distribution of deep vein thrombosis (DVT) in 562 patients with a documented DVT on venogram (Prandoni et al. [49]).
Clinical score
The distribution of the Wells clinical score estimates of DVT in the different clinical score groups from 10 studies of outpatients with suspected DVT revealed that the proportion of patients belonging to the low clinical score group was the highest when the overall prevalence of DVT was the lowest (<20%) and vice versa [47,48]. The overall prevalence of DVT ranged from18 to 14%. The relative frequency of documented DVT by CUS in the low, moderate and high Wells score ranged from 2.6-14%, from 17-56%, and from 32-76% respectively [47,48,51]. Accurate differentiation between alternative diagnosis (AD) and DVT or the absence of both in outpatients with suspected DVT by clinical assessment according to Wells scores is subjective, depends on experienced supervision by highly specialized clinicians in carefully controlled clinical settings, and appears absolutely not to be reproducible in multidisciplinary settings in hospitals or in multicenter clinical trials. Consequently we decided in 1998 the elimination of the “score of minus 2 for AD (Table 2) in our prospective DVT management study of more than 2000 outpatients with suspected DVT referred to our medical diagnostic center in Rotterdam between 2005 and 2012 to exclude or diagnose DVT and AD (Figures 5-7, manuscripts in preparation). In these prospective DVT studies we used the Rotterdam clinical score assessment as a fill-in form (Table 2) at time of DVT and AD exclusion and diagnosis in the primary care setting of a medical diagnostic laboratory (equivalent to outpatient hospital setting). ADs) like Baker’s cyst etc. has been scored in 1997 by Wells et al as minus 2 points (AD-2). This AD-minus 2 scoring procedure is not reproducible in daily clinical hospital and outpatient practice and unreliable as compared to complete CUS (CCUS) evaluation [47,48,51-56]. According to the Rotterdam modification a score of 0 (asymptomatic) means a low probability, a score of 1 or 2 a moderate probability, and a score of 3 or more a high probability for DVT (Table 2).
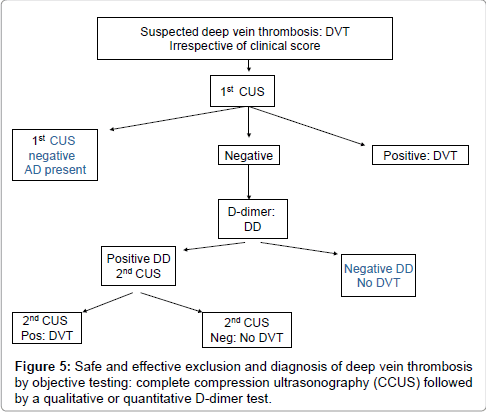
Figure 5: Safe and effective exclusion and diagnosis of deep vein thrombosis by objective testing: complete compression ultrasonography (CCUS) followed by a qualitative or quantitative D-dimer test.
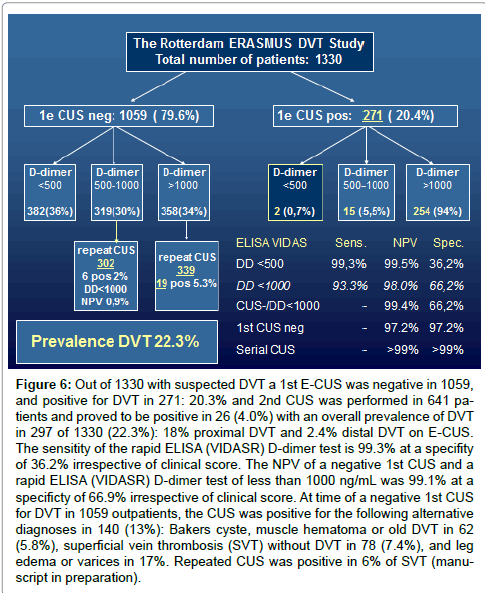
Figure 6: Out of 1330 with suspected DVT a 1st E-CUS was negative in 1059, and positive for DVT in 271: 20.3% and 2nd CUS was performed in 641 patients and proved to be positive in 26 (4.0%) with an overall prevalence of DVT in 297 of 1330 (22.3%): 18% proximal DVT and 2.4% distal DVT on E-CUS. The sensitity of the rapid ELISA (VIDASR) D-dimer test is 99.3% at a specifity of 36.2% irrespective of clinical score. The NPV of a negative 1st CUS and a rapid ELISA (VIDASR) D-dimer test of less than 1000 ng/mL was 99.1% at a specificty of 66.9% irrespective of clinical score. At time of a negative 1st CUS for DVT in 1059 outpatients, the CUS was positive for the following alternative diagnoses in 140 (13%): Bakers cyste, muscle hematoma or old DVT in 62 (5.8%), superficial vein thrombosis (SVT) without DVT in 78 (7.4%), and leg edema or varices in 17%. Repeated CUS was positive in 6% of SVT (manuscript in preparation).
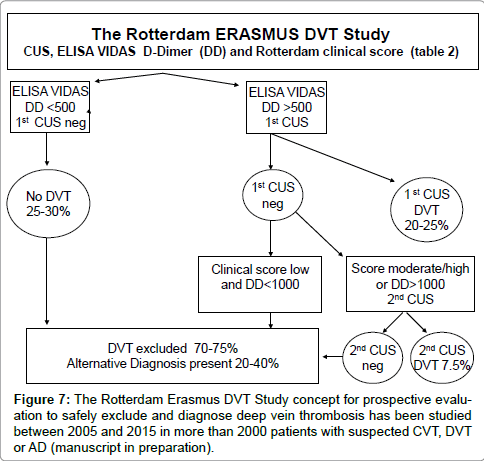
Figure 7: The Rotterdam Erasmus DVT Study concept for prospective evaluation to safely exclude and diagnose deep vein thrombosis has been studied between 2005 and 2015 in more than 2000 patients with suspected CVT, DVT or AD (manuscript in preparation).
During thrombus formation in a leg vein, thrombin (IIa) activates FXIII (XIIIa) and degrades fibrinogen into fibrin peptides (A and B) and fibrin monomers, which spontaneously form polymers, from which FIIIXa mediated firm fibrin clots are formed (Figure 2, [57]). Once fibrin (venous thrombosis) is formed the fibrinolytic process is initiated by endogenous tissue plasminogen (t-PA, urokinase plasminogen activator (u-PA)and and the FXII-XI-kallikreine system. T-PA activates plasminogen bound to fibrin (thrombus) (Figure 2), Whereas u-PA and the FXII-XI-kallikreine system activates circulating plasminogen. Plasmin degradation of cross-linked fibrin results in fibrin fragment E and D-dimer, which consist of two covalently bound D-domains. D-dimer is a final and stable degradation product of a cross-linked fibrin clot (Figure 2) [57].
Determination of the D-dimer level is a must in the diagnosis and treatment of patients with venous thrombotic disease (Figure 5). D-dimer measurement has gained a prominent role for ruling out DVT because of its high sensitivity [47,48,58,59]. The specificity of D-dimer is low because its concentrations can be raised in various other conditions, such as inflammation, pregnancy, or cancer [60-72]. The qualitative D-Dimer test SimpliRed has a sensitivity of 89%, a specificity of 77% and a NPV of 96% for the exclusion of DVT [67]. In three large prospective studies of 2239 outpatients with suspected DVT, the sensitivity of a normal quantitative ELISA VIDAS D-dimer test (cut-off level <500 ug/L) varied between 98% and 99.9% irrespective of clinical score [63-65] (Figure 6). The quantitative ELISA VIDAS test at a cut of level of 1000 ug/ml has a sensitivity of 88% to 89%, a specificity of 56% to 68% and a NPV of 96% in two large studies [47,48,68]. In large outcome studies, the sensitivity of a normal turbidimetric assay (Tinaquant, cut-off <500 ug/L for the exclusion of DVT varied from 91% to 98% and the specificity from 44% to 51% [64-66]. In this study (Figure 6) at time of a negative 1st CUS for DVT in 1059 outpatients, the CUS was positive for the following alternative diagnoses: Bakers cyste, muscle hematoma or old DVT in 62 (5.8%), for superficial vein thrombosis (SVT) without DVT in 78 (7.4%), and for leg edema or varices in 17% (Figure 6). Repeated CUS was positive in 6% of 78 SVT patients (manuscript in preparation).The sequential use of a sensitive quantitative D-dimer test, clinical score and E-CUS have been extensively studied and recommended to be a safe and the most cost-effective diagnostic work-up of DVT (Figures 7 and Table 2) [47,48,51,60,65,68].
Oudega and his team of primary care investigators assessed in 2008 the diagnostic accuracy of five point of care D-dimer assays for the exclusion of DVT (N=200, Table 4). In 200 primary care patients with suspected DVT of whom 24 (12%) had DVT on CUS both CUS results and the results of all D-dimer assays were available. At the manufaturer’provided threshold, the sensitivity and negative predictive value of the rapid ELISA D0dimer test were 100% at a specificity of 40.3% whereas all other D-dimer assays showed sensitivities of 95.8% or lower at negative predictive values somewhat higher than 98% simple because of the low prevalence of DVT (12%) (Table 4)
| D-Dimer assay | Cut –off value | Sensitivity %(CL) | Specificity %(CL) | NPV %(CL) | ROC area %(CL) |
| Vidas | 500ng/ml FEU | 100(93-100) | 40.3(33-48) | 100(97-100) | 0.89(0.83-0.95) |
| Pathfast | 0.57 µg/ml FEU | 95.8(88-100) | 34.7(28-42) | 98.4(95-100) | 0.89(0.83-0.96) |
| Cardiac | 0.5 µg/ml FEU | 95.8(88-100) | 56.8(50-64) | 99.0(97-100) | 0.87(0.80-0.94) |
| Triage | 0.35 µg/ml D-DU | 95.8(88-100) | 47.7(40-55) | 98.8(97-100) | 0.87(0.79-0.95) |
| Simplify | N.A | 91.7(81-100) | 63.1(56-70) | 98.2(96-100) | N.A |
Table 4: Diagnostic accuracy of five point of care D-dimer assays for the exclusio of deep vein thrombosis (DVT) in the primary care setting in a cohort of 200 patients with suspected DVT and a prevalence of DVT of 12% on a first compression ultrasonography (CUS) and repeated CUS within one week. V28-42. FEU: Fibrin Equivalent unit; N.A: Not applicable; D-DU: D-Dimer Unit, Cl: 99% Confidence. Interval; NPV: Negative Predictive Value; n: Number of Patients.
The advantage of (CCUS) is that it does pick up alternative diagnoses (AD) like Bakers cyste, muscle hematomas, old DVT, and superficial vein thrombosis (SVT). Other alternative diagnosis with a negative CUS include leg edema, varices, erysipelas etc (Figures 6 and 7). The NPV of CCUS by experienced specialists in the medical diagnostic laboratory setting or outpatient ward in 3 large management studies with a prevalence of DVT from 14 to 33% is high, 99.5% [54-56]. As compared to CUS and CUS-D-dimer strategy, CCUS reduces the number of CUS significantly 170 and 130 to 100 per 100 cases with a suspicion on CVT, DVT AD (Table 5). CCUS in a prospective clinical study of 623 patients with suspected DVT detected a total of alternative diagnoses in 248 cases (60.5%) [54]. An underlying disease and abnormal CCUS was found in 172 (42%), with venous reflux in 93, muscular lesion in 20, hematoma in 24, and Baker’s cyst in 35 (8 ruptured) [54]. In addition an underlying disease and normal CCUS was found in 77 (18.5%) including peripheral artery disease, cutaneous infection, neurologic/rheumatologic disease and lymphedema [54]. These clinical observations [54-56] indicate that CCUS is far superior to CUS and E-CUS (Figure 5) and should become the first objective step for the diagnosis and exclusion of CVT, DVT and AD (Figure 7).
| Series | Patients | Prox DVD Prevalence | CUS(n)per 100 patients | 3monthTE Risk(%95%CL) |
| Proximal DUS | 1st/2nd DUS | NO. Plus D-di | ||
| Cogo 1998 | 1702 | 23%/1% | 176.no | 0.7(0.3-1.2) |
| Birdwell 1988 | 404 | 14%/2% | 170,no | 0.6(0.-2.1) |
| Bernadi 1998 D-di | 946 | 22% /5.7% | 109 D-di | 0.4(0-0.9) |
| Wells 1997(VIDAS) | 593 | 14%/1.8% | 128 D-di | 0.6(0.1-1.8) |
| Kraaijenhagen,2002(Simplired) | 1756 | 22%/ 3% | 131 D-di | 0.7(0.3-1.6) |
| Pooled estimate Prox+DistalDVT | 5876 | 23% | ; - | 0.5(0.2-0.7) |
| Complete DUS | Proc/Dist DVT | |||
| Elias, 2003 | 623 | 18%/15% | 100 | 0.5(0.1-1.8) |
| Schellong, 2003 | 1646 | 7%/5% | 100 | 0.3(0.-0.8) |
| Stevens, 2004 | 445 | 9.4%/4.3% | 100 | 0.8(0.2-1.3) |
| Subramaniam,2005 | 526 | 22%/12% | 100 | 0.2(0.01-0.3) |
| Pooled estimate Prox+DistalDVT | 3240 | 10%/10%20% | 100 | 0.3(0.1-0.6) |
Table 5: Comparison of the CUS and CUS D-dimer strategy (CUS in figure) for the diagnosis of proximal deep vein thrombosis in 5 prospective management studies and the complete CUS (CCUS in figure 4) strategy in 4 prospective management studies. The CUS strategy overlooks calf vein thrombosis indicating the need to repeat CUS within one week. The CCUS picks up all CVT and proximal DVT allowing to treat both CVT and DVT thereby reducing the risk on DVT recurrence and the development of the post-thrombotic syndrome (PTS, (Table 6). Michieles et al. Sem thromb Hemostas 2000, 26: 657-667 and 2006, 32: 679-693 Righini M JTH, 2007: 55-59.
Based on personal experiences and evidence-based objective diagnostic tools we developed the Rotterdam concept (Figures 6 and 7) to safely exclude and diagnose deep vein thrombosis [47,48,51] because of the following reasoning. First, a negative CCUS and a negative VIDAS test (<500 ng/ml) exclude DVT with a sensitivity and specificity of 99.99% irrespective of clinical score assessment. After a first negative CCUS the prevalence of DVT in routine daily practice is uniformly low, 2% to 3% [47,48,69-72]. The general application of two non-specific and rather insensitive methods for DVT and AD exclusion by the combination of a negative SimpliRed (Simplify) and low clinical score should be estimated as not safe enough mainly because the prevalence of DVT in the low clinical score group may vary widely (3% to 12%) [48,65]. According to our experiences and analysis of literature findings [48,73] the safest and most effective and sensitive approach for DVT and AD exclusion is to start with objective testing with CCUS, followed by a qualitative or less sensitive D-dimer test without the use or need of clinical score assessment (Figures 4 and 7). A first negative CCUS and a negative ELISA VIDAS test (<500 ug/mL) excludes DVT irrespective of clinical score assessment (left arm, Figure 7). The combination of a negative CCUS, a low clinical score and a D-dimer level of ELISA VIDAS <1000 ug/ml, Tinaquant <800 ug/ml or negative SimpliRed (Simplify) will safely exclude deep vein thrombosis with a NPV of more than 99% in 4 prospective outcome studies (middle arm Figure 5) and surely will reach a safety near to 100% (>99.99%) in the low Rotterdam clinical score group. Those patients with a clear cut suspicion of DVT with a moderate to high Rotterdam clinical score and with pronounced increased D-dimer levels (ELISA D-dimer (VIDAS >1000 ug/ml, Tinaquant >800 ug/ml) or a positive qualitative D-dimer SimpliRed or Simplify) are candidates for a repeated CUS of the legs after one week right arm., Figure 7), simply because the prevalence of DVT on repeated CUS may be 3 to 5% of the patients [48,50].
Below-knee stockings appear to be as effective as thigh-length stockings for relief of swollen acute DVT legs and for symptomatic relief of the post-thrombotic syndrome (PTS). In acute DVT patients (21,41,73,74 MECS may also be used for symptomaticrelief of swollen acute DVT legs combined with low-molecular weight heparins (LMWH) followed by vitamin K antogonists (VKA) or novel oral anticoagulants (NOACs). Pneumatic compression therapy has been proved to be effective, but is probably only realistic in post-operative circumstances, and it has shown to be effective in for example elective knee or hip replacement [21,41,74].
Clinicians should be aware of co-morbidity as risk factors for DVT, particularly in elderly bedridden inpatients with widespread skin disease, infection, or other co-morbidities (Table 3). The incidence of DVT among general medical patients with reduced mobility ranges from 10 to 26% [74]. Prolonged sitting is as harmful as lying. Active exercise and early mobilization is desirable when possible. All hospitalized general medical patients should be assessed for venous thromboembolism risk factors [21]. Those patients classified to be at moderate at high risk should be given thrombosis prophylaxis with LMWH (4000 U or more once daily).
| Advancing age Obesity Previous venous thromboembolism Family history of venous thromboembolism Surgery, especially procedures lasting more than 30 min. Trauma, especially of the spine or legs Active cancer Acute medical ilnesses, e.g. acute myocardial infarction, heart failure, respiratory failure, infection Inflammatory bowel disease Antiphospholipid syndrome Dyslipoproteinaemia Nephrotic syndrome Paroxysmal nocturnal haemoglobinuria Myeloproliferative diseases Behçet’s syndrome Varicose veins Superficial vein thrombosis Congenital venous malformation Pulmonary embolism Long-distance travel Immobilization: Prolonged bed rest after trauma or surgery, Hospitalization, Limb paresis, paralysis, Chronic care facility stay Pregnancy/puerperium Oral contraceptives Hormone replacement therapy Heparin-induced thrombocytopenia Other drugs Chemotherapy Tamoxifen Thalidomide Antipsychotics Central venous catheter Vena cava filter Intravenous drug use |
Table 3: Co-morbidity profile in patients with deep vein thrombosis (DVT) or pulmonary embolism (PE) and disease related risk factors for DVT or venous thromboembolism (VTE) (2,3,9,14).
Surgical patients may be classified as having a low, moderate, or high thrombosis embolic risk. Low risk patients are patients under 60 years of age without any other risk factors for venous thromboembolism undergoing minor surgery (e.g. laparoscopic surgery, transurethral surgery, or out-patient surgery). These patients should be mobilized early and no additional thrombosis prophylactic regimen is required. The group of moderate risk patients consist of patients older than 60 years undergoing minor surgery, and patients younger than 60 years who undergo major surgery, but have no additional risks. These patients should be treated with LMWH (≤ 3400 U daily) or NOACs. Patients with high bleeding risk may be treated by MECS or intermittent pneumatic compression alone. High risk patients for venous thromboembolism are patients undergoing major surgery and being over 60 years of age, or having additional risk factors. These patients should be treated with LMWH (>3400 U daily). MECS may be used as additional treatment for symptomatic elief of swollen legs [21,74].
Patients undergoing major orthopedic surgery face an overall DVT rate ranging from 40 to 60% and a proximal DVT rate between 10 to 30% without thrombosis prophylaxis. The general consensus is that these patients should receive adequate thrombosis prophylaxis with LMWH, or one of the novel oral anticoagulants (NOACs). Patients receiving prolonged treatment duration (4 to 5 weeks) in hip surgery showed a significant reduction of DVT rate [21,74]. The introduction and use of the novel oral anticoagulant (NOAC) Xa or IIa inhibitors are out of scope in this review.
The diagnosis DVT should be confirmed as soon as possible by compression ultrasound if a DVT is suspected. Initial treatment with a LMWH is given subcutaneously once a day (150 to 200 IU/kg). LMWH is effective in an outpatient setting [3,21]. As soon as the diagnosis of DVT is confirmed, vitamin K antagonists (VKA e.g. warfarin) should be added to the heparin. VKA decrease the functional vitamine-K dependent procoagulant factors II, VII, IX en X to a therapeutic level of about 1/3 of normal (anticoagulation degree of INR 2.5-3) (Figure 1). LMWH inhibits via binding to AT the activated factors Xa en IIa (Figure 1). The new oral Xa-inhibitors selectively inhibit bloodcoagulation at the critical location (Xa) of the common place where the intrinsic and extrinsic coagulation pathways (Figure 1) with the ultimate consequence of decreased prothrombinase activity and decreased thrombin (IIA) generation (adequate anticoagulation without the need of laboratory monitoring).
Monitoring of anticoagulation is done by the prothrombin time, expressed in terms of the international normalized ratio (INR). A ratio between 2.0. and 3.0 should be achieved for the most adequate anticoagulation, and the lowest risk of bleeding. Heparin can be discontinued after 5 to7 days, as long as the INR is stable and 2.0 or greater [3,41]. Idiopathic venous thromboembolism is generally treated for 6 months, but anticoagulation may be for life for those with continuing risk [75]. LMWH and oral anticoagulants should be combined with ambulatory compression therapy or medical elastic stockings (MECS). Once edema has been reduced completely, class II MECS (23 to 32 mm Hg at B measurement) are prescribed to be worn for a period of 2 years. If, during the use of MECS, edema is still present, class III MECS (34 to 46 mm Hg at B measurement) are prescribed [76]. In about half of the acute DVT patients leg swelling disappears with no signs PTS at 3 to 6 months post-DVT obviating the need to wear MECS. Vena cava filters are effective in preventing the short-term incidence of pulmonary embolism in patients with proximal DVT, but they do not affect mortality. Vena cava filters are thrombogenic and double the recurrence risk of DVT, or after recurrent DVT [3].
Pulmonary embolism, post-thrombotic syndrome (PTS) and recurrent thrombosis are the main complications of DVT. If proximal DVT is left untreated, clinical pulmonary embolism will occur in 26 to 67% of the cases, and is associated with a mortality rate of 11 to 23% [77,78]. The incidence of pulmonary embolism decreases to 5% and the mortality to less than 1% under treatment [77]. About 10 to 30% of patients with DVT develop overt PTS (C4,5) at one year post-DVT. DVT has a recurrence rate of about 20% to 30% after 5 years, but the rate varies depending on the presence of risk factors and prolonged anticoagulation if indicated [78-82]. PTS is a chronic condition that affects the deep venous system, may extend to the superficial venous system of the legs in patients with a documented history of deep vein thrombosis and has been discussed in our review on DVT, DVT and PTS: bridging the gap [83,84]. In 2012 Arnoldussen and and Wittens proposed a simple scoring system for lower extremity venous thrombosis (LET) extension on CCUS [85]. The LET score can be used to expand and standardize the documentation of DVT localization and extension at time of DVT diagnosis to predict DVT recurrence rate and the risk on PTS. The LET score is helpful to identify optimal treatment options in patients with acute DVT in the primary care and hospital setting (Figure 8) [85-87]. In 2013/2014, Strijkers, Moossdorff and Michiels designed and performed the DVT-PTS Bridging the Gap pilot study and could prove the feasability to study the LET concept (Figure 8) in a large prospective evaluation on DVT and DVT recurrencein rate to reduce PTS in the primary care and hospital setting. The preliminary results in 30 newly diagnosed DVT patients produced good evidence that complete recanalization of DVT in the calf (LET Class I) and in the popliteal/femoral region (LET Class II) is predicted to occur in about one third of DVT at 3 months post-DVT with no RVT on CUS [88-90]. This will be associated with no or low risk on DVT recurrence, no reflux on DUS and low risk on PTS obviating the need of wearing stockings and no need for extended anicoagulation (Figure 8). When the recanalisation of the popliteal-femoral region is delayed and incomplete at 3 months post-DVT with RVT and/or reflux on CUS due to valve destruction in the polpiteal/femoral region at time points 3 months post-DVT will be associated with a high risk of DVT recurrence as the cause of PTS [88-90] indicating the need to extend anticoagulation preferentially with NOAC (Figure 8) [53-55]. Extension of proximal popliteal/femoral DVT into the ileofemoral region or isolated acute ileofemoral DVT with a swollen lower and upper DVT leg are candidate for Catheter Accelerated thrombolysis Versus Anticoagulation(CAVA) as the risk of severe PTS by anticoagulation alone in LET Class III/IV DVT patients alone is irreversible and high (Figure 8) [85-87].
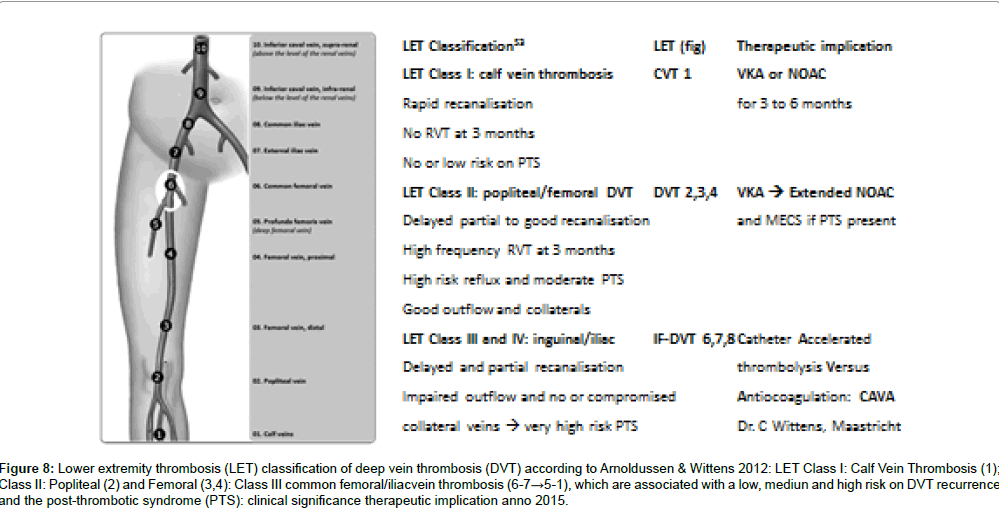
Figure 8: Lower extremity thrombosis (LET) classification of deep vein thrombosis (DVT) according to Arnoldussen & Wittens 2012: LET Class I: Calf Vein Thrombosis (1); Class II: Popliteal (2) and Femoral (3,4): Class III common femoral/iliacvein thrombosis (6-7→5-1), which are associated with a low, mediun and high risk on DVT recurrence and the post-thrombotic syndrome (PTS): clinical significance therapeutic implication anno 2015.
A possible prospective study design on DVT and PTS bridging the gap in shown in Table 6. A clinical examination of the assessment of the risk on PTS by DUS should be performed in routine clinical practice at 1 month, 3 and 6 months, 1 year, and 2 years post-DVT to determine whether there is still a need for wearing MECS in symptomatic PTS, and to see whether additional treatment is necessary (Table 6 and Figure 8). About one third of DVT patients have normal DUS 3 months post-DVT and do not develop PTS after 3–9 months post- DVT obviating the need to wear MECS and anticoagula tion (study arm 1, Table 6). In the event that RVT at 3 months post-DVT and reflux of the deep venous system is found at and after 3 months post-DVT, wearing MECS and anticoagulastion with vitamin K antagonist (VKA) or novel oral anti coagulants (NOAC) should be continued (study arm 2, Table 6). Three months post-DVT appears to be the appropriate time points to determine the group of patients who do not have RVT and the group who do have RVT and are at high risk for DVT recurrence and develop PTS. Patients with PTS CEAP 2, 3 and 4 at 3 to 6 months post-DVT seems to us candidates for long-term extended anticoagulation preferentially with low dose Direct Oral Anticoagulant (NOAC) inhibitors similar as used in the post-operative orthopedic surgery setting (Study arms 3 and 4, Table 6). There is a need for shortterm anticoagulant treatment of symptomatic calf vein trombosis (CVT) to prevent DVT extension because CVT potentially extends into the proximal popliteal and femoral veins, which can obstruct the deep venous system and place the patient at higher risk of pulmonary embolism and more severe post-thrombotic morbidity (Figure 8). About one fourth of distal vein or CVT wil extend into the popliteal and femoral region within 1 or 2 weeks, which is associated with increased risk of DVT recurrence and PTS. Extended anticoagulation is mandatory in the event of reflux with or without PTS at 6 months, 12 months, and 24 months post-DVT to prevent DVT recur rence as the cause of PTS or increase of PTS severity. This has to be demonstrated in a large prospective cost-effective, safety outcome study (Table 6 and Figure 8).
| Months | Months | Years | |||||
| 0 | 3 | 6 | 6 | 1 | 2 | 3 | 4 |
| All post DVT Patents (100%) | Study arm 1: No RVt , No PTS, Recanalisation and No reflux: no stockings | ||||||
| Symptomatic Acute DVT: | Study arm 2: | ||||||
| Medical Elastic comprehension | Extended NOAC>DOX a> 2 yrs | ||||||
| Stockings: MECS | Study arm 3: | ||||||
| Venous pressure >Stockings | |||||||
| Ar 1 to 3DUS → Evaluation for PTS | Study arm 4: Moderate PTS Obstruction=No recanalisation→ Stockings |
||||||
Table 6: 2015 rottedrdam Approach to diagnise and treat DVT anbd prevent DVT recurrence and post thrombotic syndrome.
The present report was initiated and written by Dr. Michiels in his position of Senior Investigator, Phlebology and Thrombosis, at the Department of Dermatology, Erasmus University Medical Center Rotterdam, The Netherlands, in the period between January 1, 2007 and January 1, 2014 in a joint venture with Dr. HA Martino Neumann, Rotterdam, The Netherlands and Dr Strijkers in his position of Clinical Investigator on DVT and PTS 2011-2014, Department of Vascular Surgery University Medical Center, Maastricht.