Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2014) Volume 2, Issue 6
Adult T-cell leukemia/lymphoma (ATLL) is an incurable neoplasm of mature T-cells with a median survival time of approximately one year. The aim of this study was to compare the clinical value of soluble CD30 (sCD30) levels with soluble IL-2 receptor α chain (sIL-2R) levels in two different clinical settings of ATLL patients; before an initial therapy of chemotherapy or gastric resection (n=32), and before allogeneic hematopoietic stem cell transplantation (HSCT; n=24). All patients completed the 2-year follow-up. Both sIL-2R (p=0.016) and sCD30 (p=0.030) levels were significant predictors of overall survival before the initial therapy. The number of ATLL cells in peripheral blood (PB) was correlated with sCD30 levels (Spearman’s correlation coefficient, ρ=0.46; p=0.009) but not with sIL-2R levels (ρ=0.16; P=0.38). Patients who survived for longer than two years, and for whom the percentage of ATLL cells in PB were <5%, displayed relatively low sCD30 levels, but this tendency for low sCD30 levels was not observed in longterm survivors whose ATLL cells constituted ≥5% of PB cells. sIL-2R (p=0.041) and sCD30 (p=0.0003) values were both significant predictors of overall survival in HSCT, but sCD30 levels predicted more patients with early death than were predicted by sIL-2R levels. Combination of sCD30 and CRP levels showed high sensitivity and specificity for detection of early death (within 100 days) following HSCT (81.8% and 84.6%, respectively). These results suggest that analysis of sCD30 levels may be useful for prediction of overall survival in ATLL patients, especially before HSCT. These findings would alter the treatment strategy and improve the prognosis of ATLL.
Keywords: Soluble CD30 (sCD30); Human T-cell leukemia virus type 1 (HTLV-1); Adult T-cell leukemia/lymphoma (ATLL); Allogeneic hematopoietic stem cell tr
In 1977, Takatsuki et al. described a new disease in Japan, adult T-cell leukemia/lymphoma (ATLL) [1]. At that time, researchers all over the world had been seeking human retrovirus-associated malignant disease and the first human retrovirus, Human T-cell leukemia virus type 1 (HTLV-1) was finally isolated from patients with ATLL [2,3]. Only 2–5% of HTLV-1 carriers develop ATLL with a mean latency period of more than 50 years [4]. ATLL has one of the poorest prognoses among hematologic malignancies despite aggressive treatment [5]. ATLL patients are usually first treated with chemotherapy. In exceptional cases, in which the lesions are confined to the stomach, the patients may receive surgical resection, followed by chemotherapy [6,7]. In Japan, younger survivors after chemotherapy are candidates for allogeneic hematopoietic stem cell transplantation (HSCT) [8]. Unfortunately, the unadjusted 3-year probability of overall survival (OS) after HSCT is only 33%. Multivariable analyses demonstrated four factors that adversely affect OS: older recipient age (> 50 years), male recipient, lack of complete remission at transplantation, and transplantation of unrelated cord blood [9]. About one thousand people die of ATLL annually in Japan [10]. The reported incidence of transplantation-related mortality (TRM) is as high as 25%–64% [11].
Several biomarkers have been proposed for ATLL patients [12-14]. Of these markers, soluble interleukin-2 (IL-2) receptor α chain (sIL-2R) is considered to be the most useful and is widely used in clinical practice [15]. IL-2 is a T-cell growth factor and is essential for the survival and expansion of CD4+CD25+ activated T cells in peripheral blood (PB) [16]. The IL-2R complex is composed of α, β, and γ chains, and matrix metalloproteinase (MMP)-9 mediates cleavage of the IL-2R α chain (IL-2Rα, CD25) thereby producing sIL-2R [17]. It is known that CD25 is strongly expressed on the surface of ATLL cells and that sIL-2R levels are elevated in the sera of ATLL patients [18,19].
CD30 is a cell membrane protein of the tumor necrosis factor receptor family and is expressed on activated T-cells and B-cells, as well as on some tumor virus-infected T-cells and B-cells [20]. Soluble CD30 (sCD30) has been proposed to be a prognostic factor for an unfavorable outcome in lymphoid malignancies such as Hodgkin’s lymphoma [21], and anaplastic large cell lymphoma [22]. CD30 is of particular interest in terms of HTLV-1 infection because molecular cloning of CD30 was performed using a HTLV-1-infected cell line, Hut102 [23]. Although the cells that predominantly produce sCD30 in patients with ATLL have not been identified, a significant percentage of the ATLL cells isolated from patients is positive for CD30 expression on the cell surface [24]. Levels of sCD30 are also elevated in the serum of patients with aggressive ATLL.
Early death after HSCT is a significant problem that needs to be tackled. Severe immune suppression and viral infection due to treatment and/or relapse of ATLL may be involved in such early death. A recent region-wide study in Hokkaido demonstrated for the first time that a high level of sIL-2R at HSCT was a significant risk factor for OS in HSCT [25]. In the present study, we aimed to assess and compare the clinical value of sCD30 levels with sIL-2R levels in order to predict prognosis of ATLL patients both, before the initial therapy as well as before HSCT.
Patients
The present study was a cohort study. The study protocol was approved by the Institutional Review Board of the National Hospital Organization (NHO) Kumamoto Medical Center (No. 77) on July 4, 2005. Written informed consent was obtained from all patients. This study was conducted in accordance with the ethical guidelines for epidemiological research jointly designed by the Ministry of Health, Labor and Welfare, and the Ministry of Education, Culture, Sports, Sciences and Technology, of the Japanese Government.
The subjects of this study were ATLL patients who had been referred to the Department of Hematology of our hospital between September 2005 and December 2010. ATLL was classified into four clinical subtypes according to the criteria established by the Lymphoma Study Group of the Japan Clinical Oncology Group (Shimoyama’s classification): acute, lymphoma, chronic and smoldering types [26]. This classification is based on the number of abnormal T cells in peripheral blood, serum lactic acid dehydrogenase (LDH) level, tumor lesions in various organs, and clinical course. Venous blood samples to determine sCD30 and sIL-2R levels were collected before the initial therapy or before the conditioning therapy of HSCT.
Data collection
Clinical data including age, sex, clinical subtype, Eastern Cooperative Oncology Group performance status (PS), Ann Arbor stage, Charlson Comorbidity Index [27], and laboratory findings were recorded before therapy. The simplified prognostic index, ATL-PI, was also calculated as follows, according to a previous report [28]:
Simplified ATL-PI=2 (if stage=III or IV) + 1 (if ECOG PS > 1) + 1 (if age>70 years) + 1 (if albumin<3.5 g/dL) + 1 (if sIL-2R>20000 U/mL).
Endpoint
The endpoint of the study was 2-year OS. The follow-up study ceased on the 21st December 2012, so that the last registered patient could be followed up for two years. The starting point for OS was the starting date of initial therapy (chemotherapy or total gastrectomy) and this starting point was also used for the 4 patients from our hospital who late underwent HSCT. One patient in the study died of an acute crisis before receiving chemotherapy; this case was included in the study and the starting date for survival of this case was the day of the acute crisis. In the case of HSCT, the starting point of OS was the date of transplantation. The cause of death following HSCT was categorized into disease progression or TRM. Disease progression is defined as the death in which any evidence of ATL relapse is detected. TRM is defined as the death from the adverse events of transplantation without evidence of relapse. All patients completed 2-year follow-up.
Measurement of soluble cytokine receptors
The sera of the patients before therapy were preserved at -80°C and levels of sCD30 and sIL-2R were subsequently measured using a sandwich enzyme-linked immunosorbent assay (ELISA). In some patients, serial blood samples were taken during the course of treatment if they consented to the procedures. Serum sIL-2R concentrations were measured using Cell freeN IL-2R (Kyowa Medex Co., Ltd., Shizuoka, Japan) and Determiner CL IL-2R (Kyowa Medex Co., Ltd.). Serum sCD30 concentrations were measured using Human sCD30 Platinum ELISA (eBioscience, Vienna, Austria) at the Research Laboratories of Kyowa Medex Co., Ltd., Shizuoka, Japan.
Chemotherapy
Conventional chemotherapy for aggressive ATLL was based on the Japan Clinical Oncology Group protocol and first-generation CHOP protocols containing cyclophosphamide, doxorubicin, vincristine and prednisolone, which is the standard regimen for lymphoma. The ATLL patients were treated with intensive chemotherapy with G-CSF support, such as LSG15 regimens and CHOP-V-MMV [5,29]. CHOP-V-MMV consists of CHOP plus vindesine, ranimustine and etoposide. LSG15 is a sequential combination chemotherapy consisting of three regimens: VCAP (vincristine, cyclophosphamide, doxorubicin and prednisolone), AMP (doxorubicin, ranimustine, and prednisolone) and VECP (vindesine, etoposide, carboplatin and prednisolone). We also performed modified regimens such as CHOP or THP-COP for elderly patients.
Allogeneic hematopoietic stem cell transplantation
In general, relatively young patients of 65 years or less who completed chemotherapy were usually scheduled to receive HSCT unless their general conditions worsened or the disease progressed [30]. Most of the patients for HSCT had received chemotherapy in other hospitals.
The most common conditioning regimens for HSCT were: cyclophosphamide at 60 mg/kg with total body irradiation (TBI, 1200 cGy); cyclophosphamide 60 mg/kg with busulfan (BU) 1 mg/kg (both myeloablative); and fludarabine at 30 mg/m2 from days -7 to -2 with BU at 4 mg/kg from days -5 to -4 with or without TBI 200 cGy (reduced intensity).
Patients scheduled for a sibling- or family-matched HSCT received prophylaxis for graft-versus-host disease (GVHD) comprised of cyclosporine (3 mg/kg) and methotrexate (day 1, 10 or 15 mg/m2; day 3 and 6, 7 or 10 mg/m2). Cyclosporine doses were adjusted according to renal function and daily cyclosporine levels. Patients receiving matched unrelated donor transplants received tacrolimus (0.03 mg/kg) and methotrexate (day 1, 10 or 15 mg/m2; day 3 and 6, 7 or 10 mg/m2).
Statistical analysis
Statistical analysis was performed using Prism software (GraphPad Prism 5.0, San Diego, CA). OS was plotted using the Kaplan-Meier method. Univariate analysis using the log-rank (Mantel-Cox) test was conducted to identify differences in OS. The cut-off points were set at the points in which minimal P values were obtained. The effects of clinical factors were evaluated using hazard ratios (HRs) and corresponding 95% confidence intervals (CI). Statistical analysis of differences in soluble cytokine receptors between independent groups was performed with a Mann-Whitney U test. Correlation between continuous variable and ordinal variable was analyzed by Spearman’s rank correlation (ρ) (IBM SPSS statistics 20.0, Armonk, NY). Two-tailed p values<0.05 were considered statistically significant.
Study profile
From September 2005 to December 2010, a total of 52 ATLL patients were enrolled as aggressive ATLL requiring therapy. Of these patients, 32 patients were from our hospital and were scheduled for initial therapy. The baseline characteristics of these patients are shown in Table 1. The 32 patients that were scheduled for initial therapy included 29 patients scheduled for chemotherapy, one patient who died before any therapy, and two patients who were scheduled for total gastrectomy followed by chemotherapy. For these 32 patients, the median age was 70 years old and the majority of the patients had multiple comorbidities. Acute type patients had significantly higher values of sCD30 than lymphoma type patients (p=0.025), while there were no differences in sIL-2R values between the two subtypes (p=0.24). The 2-year survival rate after the initial therapy was 22% (7 of 32 patients). All patients completed the 2-year follow-up with a median follow-up period of 4.8 months (range, 0.0 to 59 months). Four of these 32 patients underwent HSCT following chemotherapy and the other 28 patients could not undergo HSCT due to death during chemotherapy or due to their age. We also analyzed the 24 patients scheduled for HSCT (Table 1), which included the above 4 patients from our hospital and another 20 patients that were transferred from other hospitals to our hospital for HSCT. For these HSCT patients, the 2-year survival rate after HSCT was 29% (7 of 24 patients). Compared with the results before initial therapy, the serum levels of the soluble cytokine receptors were generally low in these patients after chemotherapy, before the start of conditioning therapy for HSCT, although some patients with lymphoma-type ATLL who underwent HSCT had high levels of sIL-2R.
| Characteristics | Before initial therapya | Before HSCT |
| (n=32) | (n=24) | |
| Median age, y (range) | 69.5 (43–86) | 54.5 (43–61) |
| Gender, % male | 53 | 58 |
| Subtype, n; Acute : Lymphoma : Chronic | 20:10:02 | 14:09:01 |
| Performance status, n; 0 : 1: 2 : 3 | 1 : 9 : 9: 7 | 9 : 12 : 3 : 0 |
| Charlson comorbidity indexb | 2 (0–10) | 0 (0–3) |
| ATLL cells in PB, Cells/μLb | ||
| Acute | 9697 (55–169405) | 12 (0–6063) |
| Lymphoma | 0 (0–64) | 0 (0–40) |
| Chronic | 2622, 11928 | 0 |
| Serum level of soluble IL-2R, U/mLb | 21330 (478–500691) | 927 (319–98314) |
| Acute | 23535 (478–500691) | 764 (319–27302) |
| Lymphoma | 15511 (1928–104001) | 2081 (538–98314) |
| Chronic | 5643, 11368 | 3270 |
| Serum level of soluble CD30, U/mLb | 1251 (13–21566) | 79 (14–2789) |
| Acute | 1895 (13–21566) | 74 (14–2789) |
| Lymphoma | 159 (18–3354) | 76 (38–932) |
| Chronic | 313, 1251 | 720 |
Table 1: Clinical characteristics of ATLL patients prior to initial therapy and allogeneic hematopoietic stem cell transplantation (HSCT). aThe patients included 29 patients who had undergone chemotherapy, one who had been scheduled for chemotherapy but died before therapy, and two who had undergone total gastrectomy followed by chemotherapy. bData are shown as median values (range). HSCT: allogeneic hematopoietic stem cell transplantation; PB: peripheral blood.
Overall survival in initial therapy
Univariate analysis of prognostic factors of overall survival in patients with initial therapy indicated 11 significant variables for OS in addition to the soluble cytokine receptors. These variables were: PS ≥ 3 (HR=8.9, 95% CI 3.2–25, p<0.0001), creatinine ≥1.05 mg/dL (HR=33, 95% CI 5.9–185, p<0.0001), the Charlson comorbidity index ≥ 4 (HR=126, 95% CI 15–1063, p<0.0001), BUN ≥ 45 mg/dL (HR=56606, 95% CI 1119–2864000, p<0.0001), thrombocyte count ≤ 65000 /μL (HR=73, 95% CI 7.5–705, p=0.0002), total bilirubin ≥ 3.5 mg/dL (HR=13, 95% CI 2.0–87, p=0.007), serum calcium level ≥ 10 mg/dL (HR=3.2, 95% CI 1.4–7.5, p=0.008), AST ≥ 60 IU/L (HR=3.6, 95% CI 1.3–10, p=0.012), CRP ≥ 2.5 mg/dL (HR=3.5, 95% CI 1.2–9.9, p=0.020), albumin ≤ 3.2 g/dL (HR=2.7, 95% CI 1.1–6.6, p=0.028), and age ≥ 78 years (HR=3.5, 95% CI 1.1–11, p=0.038).
Clinical values of sCD30 and sIL-2R in initial therapy
We compared the relationship between sIL-2R or sCD30 values of the 32 patients before initial therapy and OS (Figure 1). Kaplan-Meier curves showed that patients with sIL-2R ≥ 5500 U/ml (Figure 1A) had a significantly worse OS after therapy than those with sIL-2R<5500 U/ml (HR=3.2, 95% CI 1.2–8.4, p=0.016). Similarly, patients with sCD30 ≥ 140 U/ml (Figure 1B) before initial therapy had a significantly worse OS after therapy than those with sCD30<140 U/ml (HR=2.6, 95% CI 1.1–6.3, p=0.030). We also found that sCD30 levels were correlated with the significant prognostic index ATL-PI which includes sIL-2R in the index (ρ=0.41; p=0.019).
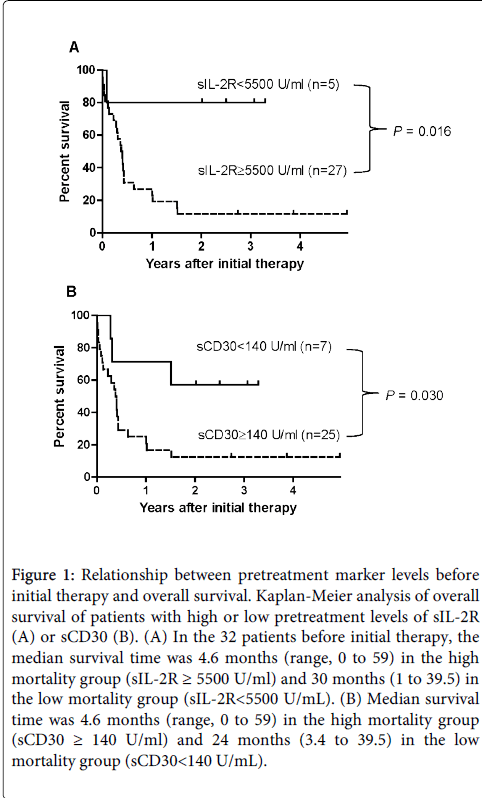
Figure 1: Relationship between pretreatment marker levels before initial therapy and overall survival. Kaplan-Meier analysis of overall survival of patients with high or low pretreatment levels of sIL-2R (A) or sCD30 (B). (A) In the 32 patients before initial therapy, the median survival time was 4.6 months (range, 0 to 59) in the high mortality group (sIL-2R ≥ 5500 U/ml) and 30 months (1 to 39.5) in the low mortality group (sIL-2R< 5500 U/mL). (B) Median survival time was 4.6 months (range, 0 to 59) in the high mortality group (sCD30 ≥ 140 U/ml) and 24 months (3.4 to 39.5) in the low mortality group (sCD30< 140 U/mL).
Soluble CD30 levels and blood ATLL cell number
As shown in Table 1, the serum levels of sCD30 in acute type ATLL were 10 times higher than those in lymphoma-type ATLL. We therefore hypothesized that sCD30 levels might be associated with the percentage of ATLL cells in PB. For analysis of this hypothesis we used a cutoff value of 5% ATLL cells in PB, because this condition identifies monoclonal proliferation of ATLL cells in PB.
In the typical smoldering type, chronic type and acute type ATLL, more than 5% of the blood cells in PB are ATLL cells. On the other hand, in lymphoma-type or other special primary extra nodal types of ATLL such as primary gastric ATLL, the percentage of ATLL cells in PB is less than 5%. As shown in Figure 2, sIL-2R levels in patients with ≥ 5% ATLL cells in PB (the PB rich group) were similar to those in patients with <5% ATLL cells in PB (the PB sparse group) (Median, range: 22525, 3987–500691 vs. 19062, 478–104001; p=0.23). In contrast, levels of sCD30 were significantly different between the two groups (Median, range: 1971, 94–21566 vs. 172, 13–3354; p=0.001). When the cytokine levels of the long-term survivors in each group were analyzed, sIL-2R and sCD30 levels were relatively low in the PB sparse group but were not always low in the PB rich group. Thus, sCD30 levels in three of the four long-term survivor cases in the PB rich group exceeded 1000 U/mL. Furthermore, there was a significant correlation between the number of ATLL cells in PB and sCD30 levels (ρ=0.46; p=0.009), but not between the number of ATLL cells and sIL-2R levels (ρ=0.16; p=0.38).
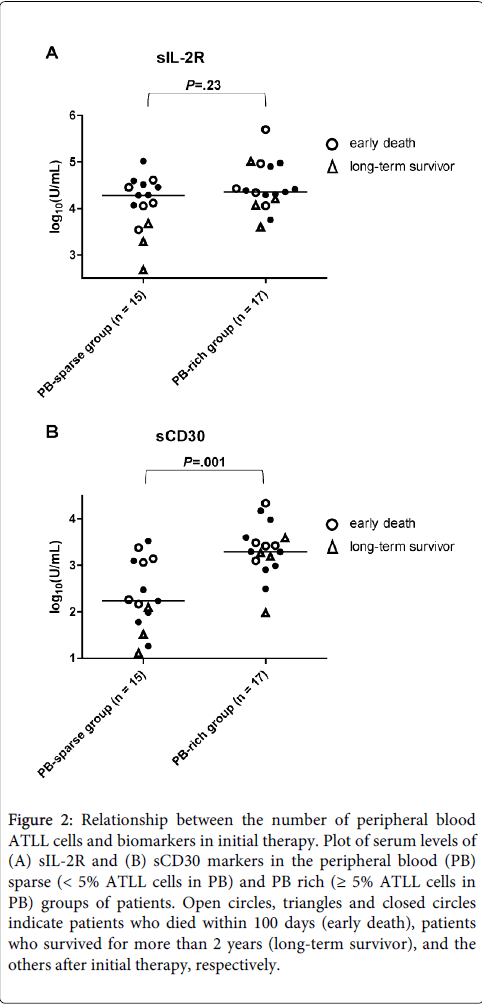
Figure 2: Relationship between the number of peripheral blood ATLL cells and biomarkers in initial therapy. Plot of serum levels of (A) sIL-2R and (B) sCD30 markers in the peripheral blood (PB) sparse (< 5% ATLL cells in PB) and PB rich (≥ 5% ATLL cells in PB) groups of patients. Open circles, triangles and closed circles indicate patients who died within 100 days (early death), patients who survived for more than 2 years (long-term survivor), and the others after initial therapy, respectively.
Analysis of overall survival in HSCT
Besides sCD30 and sIL-2R levels, seven other variables significantly differentiated OS in univariate analysis after HSCT including LDH ≥ 340 IU/L (HR=36, 95% CI 5.3–247, p=0.0002), the Charlson comorbidity index ≥2 (HR=142, 95% CI 4.7–4270, p=0.0044), CRP ≥ 0.15 mg/dL (HR=4.7, 95% CI 1.5–16, p=0.0097), BUN ≥ 17 mg/dL (HR=65, 95% CI 2.7–1545, p=0.01), HLA-mismatch (HR=3.6, 95% CI 1.1–12, p=0.034), peripheral blood stem cell transplantation (PBSCT) (HR=2.9, 95% CI 1.0–8.3, p=0.044), and thrombocytopenia (platelets ≤ 50000) (HR=16, 95% CI 1.1–245, p=0.0046). Although graft versus host disease (GVHD) occurs after HSCT, no acute GVHD or severe acute GVHD (grade III and IV) was associated with unfavorable prognosis in contrast to the favorable prognosis associated with grade I and II (HR=8.2, 95% CI 2.4–28, p=0.0007).
Clinical value of sCD30 and sIL-2R pre HSCT
We analyzed the relationship between sIL-2R or sCD30 and OS of the patients who underwent HSCT (Figure 3). Survival after HSCT sharply declined in patients with sIL-2R ≥ 16000 U/mL (Figure 3A) compared to survival in patients with sIL-2R <16000 U/mL (HR=5.8, 95% CI 1.1–31, p=0.041). A similar sharp decline in patient survival was observed in patients with sCD30 ≥ 170 U/mL (Figure 3B) compared with patients with sCD30 <170 U/mL (HR=13, 95% CI 3.2–49, p=0.0003). However, importantly, sCD30 detection of early death was much better than that of sIL-2R (detection of 8 vs. 4 early deaths respectively). The 2-year survival rates were 44% (7/16) for patients with sCD30 <170 U/mL and 35% (7/20) for patients with sIL-2R <16000 U/mL.
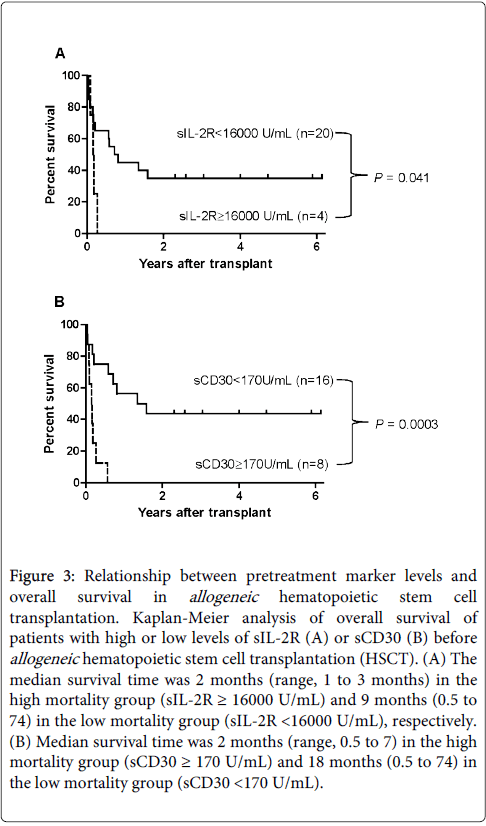
Figure 3: Relationship between pretreatment marker levels and overall survival in allogeneic hematopoietic stem cell transplantation. Kaplan-Meier analysis of overall survival of patients with high or low levels of sIL-2R (A) or sCD30 (B) before allogeneic hematopoietic stem cell transplantation (HSCT). (A) The median survival time was 2 months (range, 1 to 3 months) in the high mortality group (sIL-2R ≥ 16000 U/mL) and 9 months (0.5 to 74) in the low mortality group (sIL-2R < 16000 U/mL), respectively. (B) Median survival time was 2 months (range, 0.5 to 7) in the high mortality group (sCD30 ≥ 170 U/mL) and 18 months (0.5 to 74) in the low mortality group (sCD30 < 170 U/mL).
Cause of early death within 100 days post HSCT
Table 2 shows the characteristics of patients that died with the first 100 days following HSCT (n=11). Both sIL-2R and sCD30 marker levels are shown as well as the levels of CRP, since CRP showed a high HR value in univariate analysis. Three patients were categorized as disease progression, since there was evident relapse. The other patients did not show any evidence of recurrence and were categorized as TRM. Six cases (Cases 1,4,5,6,8 and 10) died of diffuse pulmonary infiltrates and/or interstitial pneumonia within 76 days. Five of these six patients showed high levels of sCD30 (≥ 170 U/mL) before the conditioning therapy, but only two of these six patients showed high sIL-2R levels ≥ 16000 U/mL.
| No | CRP (mg/dL) | sIL-2R (U/mL) | sCD30 (U/mL) | OS (days) | Condition before death (relapse site) | Cause of death |
| 1 | 2.2 | 3270 | 720 | 14 | IP, DPI | TRM |
| 2 | 0.18 | 575 | 43 | 15 | MOF | TRM |
| 3 | 0.02 | 713 | 81 | 19 | MOF | TRM |
| 4 | 0.1 | 1943 | 173 | 30 | IP, DPI, MOF | TRM |
| 5 | 0.73 | 19375 | 2384 | 32 | IP, DPI, MOF | TRM |
| 6 | 0.32 | 2630 | 442 | 55 | IP | TRM |
| 7 | 0.12 | 618 | 66 | 61 | aGVHD | TRM |
| 8 | 17 | 98314 | 932 | 59 | DPI, Relapse (PE) | Disease progression |
| 9 | 0.16 | 27302 | 2789 | 64 | Relapse (LN) | Disease progression |
| 10 | 0.23 | 319 | 14 | 76 | IP, IPS | TRM |
| 11 | 0.21 | 16835 | 808 | 99 | Relapse (LN) | Disease progression |
Table 2: Biomarkers of early death of adult T-cell leukemia/lymphoma after allogeneic hematopoietic stem cell transplantation. Values above the cutoff levels are indicated by underlines. OS: overall survival following transplantation; IP, interstitial pneumonia; DPI, diffuse pulmonary infiltrates; MOF, multiple organ failure; aGVHD, acute graft versus host disease; PE, pleural effusion; LN, lymph node; IPS, idiopathic pneumonia syndrome; TRM, transplantation-related mortality.
Of the four patients with sCD30 <170 U/mL (Cases 2,3,7 and 10), two patients (Cases 2 and 3) died from a coagulation abnormality. One of these patients (Case 2) died of multiple organ failure (MOF) with ascites from disseminated intravascular coagulation. The other patient (Case 3) died of MOF with bone marrow and renal failure from veno-occlusive disease. Of the other two patients, one patient (Case 7) died from severe acute GVHD (grade III). The sCD30 level of this patient was elevated to 467.4 U/mL at the peak of GVHD. The other patient (Case 10) died on day 76 from HSCT. This patient had achieved complete remission of the primary ATLL in the lung but the patient developed idiopathic pneumonia syndrome after HSCT. The sCD30 levels of this patient were elevated to 147 U/mL during the conditioning regimen. All four of these cases (Cases 2,3,7 and 10) were negative for sIL-2R. Cases 3 and 7 were negative for CRP, sIL-2R and sCD30.
Of the remaining cases, 3 cases (Cases 1, 4 and 6) were sIL-2R negative and sCD30 positive, and the causes of death of these patients were classified as TRM. The four remaining cases (Cases 5, 8, 9 and 11) showed high levels of both sIL-2R (≥ 16000 U/ml) and sCD30 (≥ 800 U/mL) and 3 of these cases (Cases 8, 9 and 11) died from relapse (2 lymphoma-type and 1 acute type). These 4 patients were also positive for CRP.
Levels of sCD30 ≥ 170 U/mL and CRP ≥ 0.15 mg/dL were implicated in early death (sensitivity and specificity: sCD30, 63.6% and 92.3%, respectively; CRP, 72.3% and 92.3%, respectively). Furthermore, the combination of sCD30 ≥ 170 U/mL and/or CRP ≥ 0.15 mg/dL showed higher sensitivity for early death (sensitivity 81.8% and specificity 84.6%). No additional effects on sensitivity or specificity were observed if sIL-2R levels were added to this combination.
In this study, we evaluated and compared the clinical value of serum levels of sCD30 and sIL-2R for ATLL patients. Although both sCD30 and sIL-2R were significant predictors of OS before the initial therapy, the number of ATLL cells in PB was correlated with sCD30 levels but not with sIL-2R levels. Therefore, sCD30 may be a good marker when there are few ATLL cells in PB. sCD30 showed a better predictive power than sIL-2R in HSCT. Furthermore, the combination of sCD30 and CRP demonstrated high sensitivity and specificity for early death within the first 100 days following HSCT. To our knowledge, this is the first report to demonstrate the clinical value of sCD30 in ATLL patients.
A previous study identified independent prognostic factors for untreated ATLL, which included poor PS, high LDH, age ≥ 40 years, total number of involved lesions, and hypercalcemia before chemotherapy [31]. Recently, another study identified factors such as Ann Arbor stage (III and IV), PS (2 to 4), age, serum albumin, and sIL-2R as independent prognostic factors of chemotherapy [28]. These authors also proposed a new prognostic index for acute and lymphoma-type ATLL (ATL-PI). We found that sCD30 significantly correlated with ATL-PI. Therefore, sCD30 might be a clinical marker in ATLL patients undergoing initial therapy, similar to its reported ability to act as a marker for B-cell and T-cell lymphomas [21,22,32,33]. In addition, we found that sCD30 levels were higher when more than 5% of PB cells were ATLL cells. It is possible that ATLL cells in PB might produce higher levels of sCD30 than ATLL cells in the lymph nodes or the stomach. Therefore, analysis of the serum level of sCD30 may be useful for detection of the aggressiveness of disease in the PB sparse group.
Regarding OS in HSCT, a previous study identified five significant variables that are related to poor OS including advanced age, male sex, failure to attain complete remission, poor PS, and transplantation from unrelated donors [34]. Furthermore, a high level of sIL-2R was recently demonstrated to predict worse HSCT outcome [25]. In the present study, our results suggest that sCD30 has a better predictive power than sIL-2R for detecting unfavorable prognosis.
TRM and relapse also occurred frequently following HSCT. We showed that combination of sCD30 and CRP analysis may be a powerful tool for prediction of the early death of patients undergoing HSCT. It is possible that the observed elevations in sCD30 levels and CRP values are associated with a proinflammatory state before the immunosuppressant therapy. Conditioning therapy probably activates tissue macrophages leading to a cytokine storm and activation of HTLV-1-infected cells. The CRP level is controlled by circulating IL-6 levels, which are elevated in ATLL patients [35,36]. This high IL-6 level may be the reason why STAT3, which is downstream of IL-6 signaling, is constitutively activated in ATLL cells in vivo [37]. Therefore, HSCT might be ineffective and dangerous for ATLL patients with sCD30 ≥ 170 U/ml and/or CRP ≥ 0.15 mg/dL before conditioning regimens. Additional therapy including IL-6/Jak/STAT3 signaling inhibitor and anti-CD30 monoclonal antibody might be considered for concrete treatment of the proinflammatory state in such patients [38,39]. Otherwise, alternative therapy might be effective for these patients [40,41]. Our data suggest that sCD30 elevation before the conditioning therapy is associated with diffuse pulmonary lesions or relapse. The pathophysiology of these pulmonary lesions will be elucidated in the future.
The main limitation of this study is the small number of patients that was analyzed, which meant that we were unable to perform multivariate analysis. Although HTLV-1 is endemic in the Kyushu region of Japan, the incidence of ATLL is very low and there is a long latency period between HTLV-1 infection and development of ATLL. It is therefore difficult to obtain a large number of samples. A multicenter cohort study is needed to confirm our results in the future.
In conclusion, we investigated sCD30 and sIL-2 levels in ATLL under 2 different clinical settings; before initiation therapy and before HSCT. Our results suggest that sCD30 may be a prognostic factor before the initial therapy. However, since sCD30 levels are correlated with the number of ATLL cells in PB, analysis of their levels may not be useful for prediction of overall survival when PB is rich in ATLL cells. Our results suggest that sCD30 may be a useful biomarker before HSCT therapy, because a high sCD30 level before HSCT was implicated in early death after HSCT. In ATLL patients with an sCD30 level ≥ 170 U/ml and/or CRP ≥ 0.15 mg/dL, HSCT may not be a suitable therapy. Early diagnosis and treatment of the proinflammatory state could reduce the morbidity and mortality of patients undergoing HSCT. Hopefully, the use of these markers will help to reduce the early deaths and TRM of HSCT.
We thank Ms. Megumi Fujsaki in the Clinical Laboratory and the staff of the Hematology Department of NHO Kumamoto Medical Center for supporting this project. We also thank Dr. Okada for critical reading of the manuscript.
This study was supported in part by research funding from Kyowa Medex Co., Ltd., Tokyo, Japan (to S. Takemoto).
Contribution: R. Pornkuna designed the research, analyzed the data, interpreted the data, and drafted the manuscript; S. Takemoto designed the research, acquired data, interpreted the data, and revised the manuscript; M. Hidaka and F. Kawano provided clinical samples, interpreted the data and revised the manuscript; Y. Haga interpreted the data, revised the manuscript critically for important intellectual content. All authors read and approved the final version of the manuscript.
S. Takemoto received research funding from Kyowa Medex Co., Ltd. (Tokyo, Japan) and Kyowa Hakko Kirin (Tokyo, Japan). Only the funding source from Kyowa Medex Co., Ltd. was used to perform sCD30 and sIL-2R measurements. No funding source affected the study design, data collection, data analysis, data interpretation, or writing of the report. All samples were handled anonymously. The remaining authors declare no competing financial interests.