Journal of Leukemia
Open Access
ISSN: 2329-6917
ISSN: 2329-6917
Case Report - (2017) Volume 5, Issue 4
Chronic lymphocytic leukemia (CLL) is a mature B-cell neoplasm with characteristic immunophenotype. This report presents a rare case of CLL with co-expression of T-cell marker CD8. The molecular analysis confirmed clonal immunoglobulin genes and no clonal rearrangement for T-cell receptor β and γ genes. The cell morphology was atypical of CLL, with features resembling reactive T lymphocytes. The phenotypic and morphologic findings may represent a CLL variant.
Keywords: CLL; Variant phenotype; CD8; Atypical morphology
The diagnosis of chronic lymphocytic leukemia (CLL) requires a characteristic B-cell phenotype. CLL cells are identified typically by flow cytometry analysis for immunophenopic features including lymphocyte clonality as indicated by κ or λ light chain predominance, positive for CD5, CD19, CD20 and CD23, weak or negative for CD79b; and dim or low level surface immunoglobulin (sIg) [1]. The immunephenotype is essential for CLL diagnosis as well as its differentiation from other lymphoproliferative entities.
Although cell markers are used for identification of cell lineages, aberrant expression of lineage markers has been found in a range of malignancies. In particular, the finding of acute leukemia that expressed both myeloid and lymphoid antigens has been the subject of two alternative notions of “lineage infidelity” and “lineage promiscuity” [2,3]. The former refers to a deviation from lineage commitment by malignant transformation, whereas the latter suggests the malignant cells reflect the progenitor cells that co-express antigens of more than one lineage. CD8 is an antigen normally expressed on cytotoxic T cells and NK cells. However, there are occasional reports of CD8 expression in CLL and other B-cell neoplasms. Most are reports of single cases or small case series. It is not clear whether CD8 expression is associated with disease progression [4-12].
Herein we report a case of CLL with co-expression of CD8. The disease had remained stable over a period of 17 years. In addition to aberrant CD8 expression, the CLL cells also showed atypical morphology. The findings may represent a rare variant of CLL.
A 44-year-old Caucasian woman initially presented with right anterior cervical lymphadenopathy and peripheral lymphocytosis. The complete blood count showed hemoglobin of 137 g/L, WBC of 15 × 109/L with 57% lymphocytes and platelet count of 226 × 109/L. The diagnosis was made based on peripheral blood flow cytometry that showed a clonal population with CLL phenotype, positive CD5, CD19, CD23, weak CD20 and dim surface κ light chain, and negative for CD79b and FMC-7. CD38 was positive in 9% of the CLL cells. In addition, the CLL cells were clearly positive for CD8, but not other Tcell associated antigens of CD3, CD7, CD2 and CD4. Flow cytometry analysis was repeated during the follow-up and the CLL cell population retained the same phenotype, including CD8 expression (Figure 1).
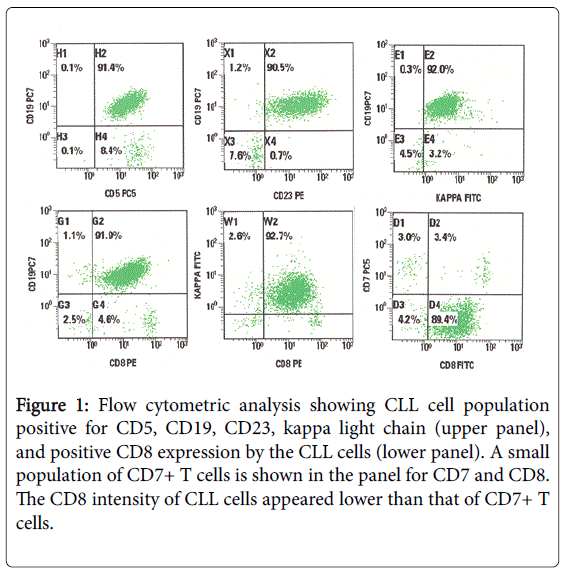
Figure 1: Flow cytometric analysis showing CLL cell population positive for CD5, CD19, CD23, kappa light chain (upper panel), and positive CD8 expression by the CLL cells (lower panel). A small population of CD7+ T cells is shown in the panel for CD7 and CD8. The CD8 intensity of CLL cells appeared lower than that of CD7+ T cells.
Notably, blood film review showed atypical morphology of CLL cells. Most cells appeared larger in size, with irregular and pleomorphic nuclei, and relative abundance of cytoplasm and scalloped cell borders (Figure 2).
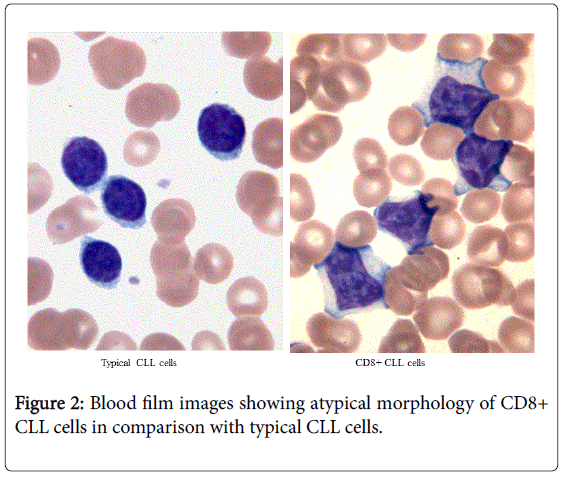
Figure 2: Blood film images showing atypical morphology of CD8+ CLL cells in comparison with typical CLL cells.
Additional investigations included cytogenetics and molecular analysis for clonality. Fluorescent in situ hybridization (FISH) showed a common CLL finding of 13q deletion. PCR-based assays showed a clonal pattern of IGH rearrangement, but no clonal rearrangement of T-cell receptor β and γ genes.
The patient gradually developed bilateral axillary, cervical, supraclavicular, hilar, and retroperitoneal lymphadenopathy. She remained well and stable, not requiring treatment for CLL for 17 years after the initial presentation. The lymphocyte counts increased slowly to 25 × 109/L, and hemoglobin of 120 g/L and moderate thrombocytopenia with platelet count of 61 × 109/L. Ultrasound demonstrated an enlarged spleen measuring 15.4 cm and no hepatomegaly.
This case demonstrated a variant CD8 expression in B-cell neoplasm. Flow cytometry showed a homogeneous pattern of CD8 expression on the CLL cell population. The cells were otherwise typical of CLL phenotype. Aberrant expression of CD8 in CLL is rare but has been reported previously. The retrospective studies revealed a frequency of 0.5-3% for the aberrant expression of CD8 in CLL [6,9]. CD8 expression was also found in other types of B-cell neoplasms, though even more rarely than in CLL. The data from a large series of 951 patients with B-cell non-Hodgkin lymphoma showed 1.89% overall frequency of CD8 co-expression. Of the 18 patients with CD8 expression, 11 were CLL/small lymphocytic lymphoma; 7 others included diffuse large cell lymphoma, follicular lymphoma, marginal zone lymphoma and lymphoplasmacytic lymphoma [6].
CD8 expression in CLL has been reported with variable clinical courses. Some reports suggested that CD8 expression was associated with a favorable prognosis either in terms of lack of progression or good response to treatment [4-12]; however, other reports suggested CD8 as a marker of aggressive disease [13,14]. Our patient showed an indolent clinical course. For a follow-up period of 17 years, the patient remained well and did not require treatment, although her CLL progressed slowly in the degree of lymphocytosis, lymphadenopathy and splenomegaly. Overall, CD8 expression appears a rare and aberrant phenotype in CLL. Its clinical significance, if any, remains to be determined. Interestingly, in our case the morphology of CLL cells was atypical. These CLL cells resembled T cells in reactive processes. Only one other case of CD8+ B-CLL with atypical morphology was reported in the literature [9]. As there were no descriptions of morphological features in most reports, further study is required to determine whether CD8 expression is commonly associated with atypical morphology of CLL.
The biological nature of CD8 expression in CLL is unknown. Normally, CD8 expression is associated with cytotoxic T-cells as well as NK cells. During T cell development, CD8 expression occurs at a later stage and it follows CD3, CD5, CD7 expression and T-cell receptor gene arrangement. As a surface glycoprotein, CD8 functions as a coreceptor with the T-cell receptor to recognize and bind class I MHC on antigen presenting cells [15]. The cytoplasmic domain of CD8 recruits the T-cell specific tyrosine kinase, p56lck, to the TCR-CD8-MHC signalling complex triggering downstream signalling for T-cell activation [16]. A previous study showed that p56lck was absent in three of four cases of CD8+ CLL, suggesting a non-functional CD8 in CLL cells [9]. In our patient, the CLL population clearly expressed CD8, but lacked the T-lineage defining antigens of CD3 and CD7. In addition, molecular analysis confirmed the B-cell clonality of IGH and IGK genes, but no clonal rearrangement of TCR genes. These findings suggest that CD8 expression did not occur as a part of lineage commitment process of T-cells, but likely an aberrant gene expression event in the transformed clonal B-cells.