Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Case Report - (2014) Volume 2, Issue 6
Thrombosis of cerebral veins and sinuses (CVST) is a rare condition seldom affecting young adults and children. The development of cerebral sinus thrombosis as a complication of heparin-induced thrombocytopenia/thrombosis syndrome (HIT/HITT) is even rarer. We describe a case of a 17-year old female with multiple fractures, who developed CVST secondary to HIT, while being under thromboprophylaxis with low molecular weight heparin (LMWH). The patient was successfully treated afterwards with 7.5 mg fondaparinux once daily subcutaneously. Our patient’s outcome was excellent, without recurrent thrombotic or bleeding events throughout her therapy. Fondaparinux is a synthetic pentasaccharide selectively inhibiting activated factor X. Published data have shown that due to its short structure, the drug almost never causes clinical HIT/HITT, therefore it could be a useful alternative anticoagulant agent for treating HIT/HITT patients.
Keywords: Hit/Hitt Syndrome; Cerebral Vein; Sinus Thrombosis; Fondaparinux
Thrombosis of cerebral veins and sinuses (CVST) is a rare condition seldom affecting young adults and children [1]. The estimated annual incidence raises up to 3-4 cases per million of adult population and up to 7 cases per million among children. There are several risk factors for CVST mainly inherited thrombophilias and acquired prothrombotic conditions including cardiac pathologies, infections, and phrothrombotic metabolic and vascular disorders. However, the aetiology of ischemic stroke in the young remains still unknowh in more than one third of the patients [2]. CVST is associated with significant morbidity and mortality in children and antithrombotic therapy with heparin in the acute phase followed by warfarin is recommended both in children and adults. The development of CVST as a complication of heparin-induced thrombocytopenia/thrombosis syndrome (HIT/HITT), albeit rare, has been previously reported. In fact, CVST occurred in 3 (2.5%) of 105 HIT patients in one study and in 7 (1.7%) of 408 HIT patients in another, as far as the clinical presentation of the syndrome was concerned in both [3,4].
Trauma patients have an enhanced risk for thrombosis and thus anticoagulation with prophylactic heparin doses is strongly recommended [5]. Prophylaxis with low-molecular-weight heparin (LMWH) seems to be more effective than unfractionated heparin (UFH) in these patients. However, both LMWH and UFH carry a potential risk of HIT/HITT, which is a well documented immune mediated severe adverse reaction to heparin administration.
HIT/HITT syndrome results from the development of an antibody, usually polyclonal IgG, that reacts with the heparin/platelet factor-4 (Hep/PF4) complex, causing both thrombocytopenia and a hypercoagulable state, via enhanced thrombin generation [6-9]. The incidence of HIT depends on patient characteristics and heparin type, dose and administration route. The frequency of HIT/HITT is greater in surgical and trauma than in medical patients [7-9]. Overall, clinically symptomatic HIT/HITT develops in 1% of hospital patients receiving any type of heparin. Venous or arterial thromboembolic complications will develop in 30-75% of patients with HIT, unless they are treated with an alternative anticoagulant [6-9].
Fondaparinux is a synthetic pentasaccharide which selectively inhibits Factor Xa, enhancing antithrombin activity. The drug is administered once daily subcutaneously (sc) and can be used both for prophylaxis (2.5 mg/day) and treatment (5-10 mg/day, according to body weight) in a vast number of (pro)thrombotic disorders (especially for thromboprophylaxis in orthopedic patients), without monitoring of anti-Xa activity in patients with normal creatinine clearance. Considering already published data [10-13], fondaparinux could reasonably be used as an alternative anticoagulant in HIT/HITT patients.
We herein report a case of an adolescent female with multiple fractures, who was receiving LMWH thromboprophylaxis and developed a cerebral sinus thrombosis as consequence of HIT/HITT. Our patient was successfully treated with fondaparinux.
Our patient was a 17-year old female with multiple fractures of lower extremities and soft tissue extensive injuries of upper extremities, resulted from a motor vehicle crash. She was transferred to our hospital for surgical management of her fractures and reconstructive surgeries of the above mentioned anatomic regions, after a 4-day hospitalization in a peripheral hospital. Treatment with prophylactic LMWH (enoxaparin 4000 IU once daily sc) was started on the 2nd day after her accident. No heparin flushes were administered into our patient’s central venous catheters. She also suffered from seronegative rheumatoid arthritis, which was diagnosed 2 years earlier, without need for treatment. On her 2nd day in our hospital (5th day on heparin administration), Doppler studies revealed left humeral artery thrombosis. Patient started immediately therapeutic doses of enoxaparin sc (100 U/kg of body weight twice daily). At that time, laboratory testing disclosed normal erythrocyte and leukocyte counts, but platelet count was 110 x 109/l. Unfortunately, the patient was discharged from the peripheral hospital with an unremarkable laboratory follow-up (initial platelet count was unknown). On her 7th day in our hospital (10th day on enoxaparin administration), she had severe headache, accompanied with nausea and acutely altered mental status. At this time, her platelet count was 29 x 109/l and had concurrent elevated D-Dimer levels. Trauma induced pathologic disseminated intravascular coagulation was excluded (normal fibrinogen and PT/aPTT levels, normal serum LDH level, absence of schistocytes in the peripheral blood film). A cerebral computed tomography scan (CT), along with a magnetic resonance imaging (MRI), both showed cerebral venous thrombosis involving the left transverse and sigmoid sinuses (Figure 1). Based upon platelet count fall and thromboembolic event, HITT was clinically suspected. Diagnosis was confirmed by the strongly positive enzyme immunoassay for antibodies against heparin-platelet factor 4 complex (Asserachrom HPIA, Diagnostica Stago). Enoxaparin was stopped immediately and 7.5 mg fondaparinux sodium (Arixtra®, GlaxoSmithKline, Athens, Greece) was started subcutaneously daily, because of lack of other approved nonheparin anticoagulants for HIT. The clinical status of our patient gradually improved, D-Dimer levels decreased and platelet count normalized 6 days after fondaparinux initiation (Figure 2). On 6th day of fondaparinux, acenocoumarol was started in parallel, with a target international normalized ratio (INR) between 2.0 and 3.0. Fondaparinux was stopped after a total 10-day-treatment and patient’s INR being within the target above for at least 24 hours. A follow-up MRI one month later showed normal blood flow in all cerebral sinuses, while patient had no clinical neurological sequelae (Figure 3). Patient continued acenocoumarol per os for a total period of 6 months and interrupted anticoagulation after a negative D-Dimer test, along with a negative enzyme immunoassay test for HIT-antibodies.
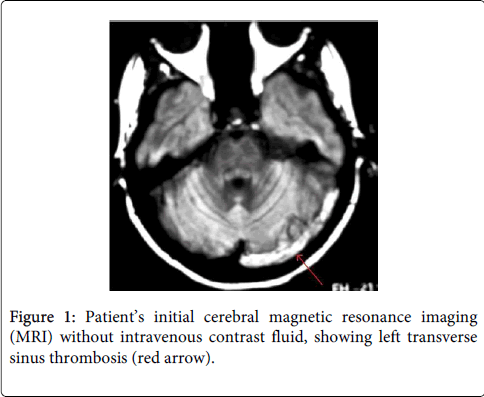
Figure 1: Patient’s initial cerebral magnetic resonance imaging (MRI) without intravenous contrast fluid, showing left transverse sinus thrombosis (red arrow).
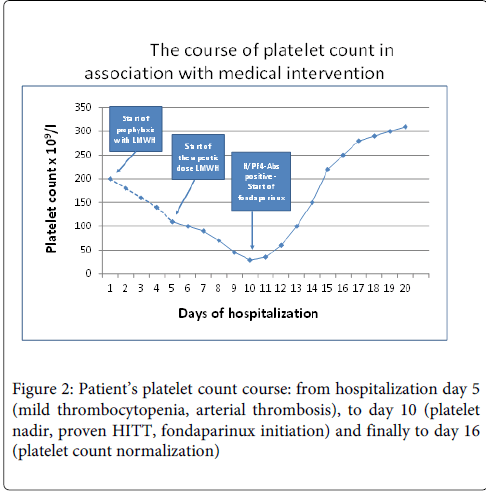
Figure 2: Patient’s platelet count course: from hospitalization day 5 (mild thrombocytopenia, arterial thrombosis), to day 10 (platelet nadir, proven HITT, fondaparinux initiation) and finally to day 16 (platelet count normalization)
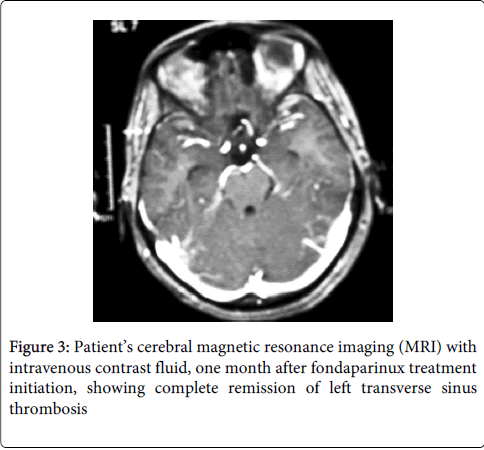
Figure 3: Patient’s cerebral magnetic resonance imaging (MRI) with intravenous contrast fluid, one month after fondaparinux treatment initiation, showing complete remission of left transverse sinus thrombosis
The reported incidence of venous thromboembolism (VTE) after trauma varies from 7% to 58% in various studies depending upon the patients demographics, the site and nature of injuries, the diagnostic method used for detection of VTE and the type of prophylaxis used in the study population [5,14]. Without thromboprophylaxis, patients with multisystem or major trauma have a deep venous thrombosis (DVT) risk that exceeds 50%, while pulmonary embolism (PE) is the third-leading cause of death in those who survive beyond the first day of hospitalization [5]. Lower extremity fractures and the need for a surgical procedure are both independent predictors of VTE in trauma patients [5,14].
Heparin induced thrombocytopenia/thrombosis syndrome (HIT/HITT) is a rare and serious adverse reaction to heparin administration, which shares thrombocytopenia and enhanced thrombin generation. Without immediate alternative anticoagulation, HIT/HITT has a mortality rate from 18.8% to 50%. Syndrome usually occurs 5-10 days after heparin initiation, but an early onset may be seen in patients who have a previous exposure to heparin, usually during the last 100 days. The hallmark of HIT/HITT is the formation of a polyclonal (usually IgG) antibody against heparin-platelet factor 4 (Hep/PF4) complex, which is accompanied with thrombocytopenia (=50% platelet count fall due to platelet aggregation and consumption) and/or arterial or venous thrombosis (HIT and/or HITT respectively) [6-9]. In orthopaedic patients who are under prophylactic doses of heparin, the incidence of HIT ranges between 5% in patients under UFH and 0.5% in those under LMWH [15]. HIT can occur in 0.5% to 1% of patients who receive lower doses of heparin (sc or heparin flushes). HITT-related venous or arterial thrombosis can occur even before or in the absence of thrombocytopenia. Other symptoms observed in children include acute thoracic pain, respiratory distress, anaphylactic shock and prolonged fever [16]. CVST as a complication of HIT/HITT has already been reported [3,4,17,18]. In the majority of cases, CVST is associated with hypercoagulable states and is a rather frightening event, because of the severity of clinical manifestations and high mortality rate, estimated between 5 to 30 percent of patients. Clinically, CVST presents with a wide range of symptoms, including headache, focal deficits (motor or sensory), dysphasia, seizures and impaired consciousness [1].
The management of HIT/HITT syndrome includes both discontinuation of heparin therapy and use of an alternative anticoagulant, such as direct thrombin inhibitors (DTI, lepirudine and argatroban) or heparinoids (danaparoid) [7,9]. Unfortunately, these agents were not available in Greece this period. Furthermore their usefulness is limited, first because they are administered by continuous intravenous infusions, second because of frequent activated partial thromboplastin time (aPTT) monitoring requirement and third because they prolong both aPTT and international normalized ratio (INR), thus complicating transition of HIT-patients to per os anticoagulation with vitamin K antagonists (VKAs, acenocoumarol, warfarin) [19,20].
Fondaparinux has an average half-life of 18 hours, being suitable for once-daily sc administration. The risk of major bleeding from fondaparinux was not found to be significantly higher than LMWH when used for VTE-prevention or treatment (at 2,5 mg and 5-10 mg per day respectively), in patients without serious renal impairment. The structure of fondaparinux is identical to the main anticoagulant pentasaccharide domain of UFH. Previous reports have shown the presence of HIT-antibodies in the plasma of patients who are receiving fondaparinux (HIT-seroconversion), however its complex with PF4 is short enough, so HIT-antibodies against it almost never cause clinical HIT/HITT. No episode of HIT was reported in the large phase 2 and 3 fondaparinux clinical trials [10,11], strongly indicating that drug rarely cross-reacts with HIT-antibodies in vivo and in vitro [12]. It has also been shown that fondaparinux cannot stimulate platelet serotonine release, nor activate platelets in the presence of HIT-patients sera [13]. Published data on fondaparinux in HIT is limited to case reports, small case series and one open-label prospective pilot study [21-26]. However fondaparinux is increasingly being used on the basis of successful clinical experience [25,27].
Our patient had multiple fractures of lower extremities with need for surgical management. Furthermore, she had a history of rheumatoid arthritis, which is an autoimmune disease. According to a recent study [28], the risk of VTE in hospitalized patients with rheumatoid arthritis was approximately twice the risk of VTE in non- rheumatoid arthritis patients. Therefore, our patient had multiple factors associated with increased risk of VTE, which raised the need for thromboprophylaxis use. The same risk factors are well-known to be associated with HIT, as well. Despite the risk factors, the diagnosis of HIT was delayed mainly because trauma patients often present with multifactorial thrombocytopenia. Additionally, in our patient the pre-heparin platelet count was unknown. She displayed mild thrombocytopenia (110 x 109/l) on 5th day of heparin treatment, when upper extremity arterial thrombosis was diagnosed. By that time, the suspicion of HIT was missed and LMWH rose to therapeutic dose. HIT/HITT was strongly suspected when her platelet count fell furthermore (to 29 x 109/l), along with CVST manifestation. At that time, although current guidelines strongly suggest lepirudin, argatroban, or danaparoid administration in HITT patients, whereas fondaparinux is only weakly suggested as a therapeutic option due to its (albeit very low) potential to cause HIT/HITT itself, we decided to use Arixtra®, because it was the only available nonheparin anticoagulant. Furthermore it has facile administration (once daily sc) and unrequired monitoring of its anti-Xa activity, as far as the patient had normal serum creatinine levels. Our patient had an uneventful outcome with successful antithrombotic effect. The overlapping use of coumarin and fondaparinux did not result in major bleeding or venous limb gangrene.
The management of CVST still remains a challenge. Despite aggressive therapy, CVST-associated mortality has been reported as high. If CVST is suspected or presented in a patient who is currently using or has recently used heparin, HITT must be ruled out, since this condition represents an absolute contraindication to further heparin administration and an absolute indication for an alternative anticoagulant drug initiation. As this case illustrates, fondaparinux may be a valuable alternative option. To our knowledge, there are limited data in the literature for the use of fondaparinux in HITT-patients with CVST. Thorsteinsson et al [29] reported a case of successful fondaparinux use in an 18-year-old male who displayed a CVST during ulcerative colitis relapse and developed HITT while on heparin treatment.
In conclusion, we report a safe and effective use of fondaparinux in a HITT-patient who presented with CVST. However, three case reports of possible fondaparinux-related thrombocytopenia/thrombosis [30,31], a report of fondaparinux-associated thrombocytopenia in a previous LMWH-associated HIT [32] and another report of in vivo and in vitro probable cross-reactivity of fondaparinux with HIT-antibodies [33] suggest that its safety needs to be further elucidated via randomized double-blind multicenter controlled clinical trials.
Authors need to thank our Department’s Molecular Biologist Mrs Anastasia Chaikali for her expert laboratory assistance concerning HIT/HITT-diagnosis. Also, we need to thank our colleagues from Orthopaedic Department and ICU Department for their cooperation in Patient’s diagnosis and treatment, as far as in proper recording and collecting essential clinical and laboratory information about her hospitalization and follow-up period.