Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 1
Insomnia is a major health problem, commonly leading to pharmacological treatment. During recent years, behavioural therapies have gained stronger therapeutic position, not least cognitive behavioural therapy (CBT). The aim was to investigate the effect of a CBT-based group intervention for insomnia in primary care, by means of self-reported sleep quality and duration. In addition, cortisol in saliva, as a biological marker of stress was tested. Methods: Fifty participants with primary insomnia, attending primary care, were enrolled, 35 receiving the intervention, and 15 serving as control. The intervention group was recruited during the first two study years, and controls during a following third year, without randomization. The intervention included eight CBT-based group sessions, each two-hour long and led by a psychologist, with 4-6 participants in each group. Controls were handled in accordance with ordinary clinical routine, including pharmacological intervention. Sleep onset time, duration and quality were assessed before and after the intervention, by patients filling-out the Pittsburgh Sleep Quality Index (PSQI). Insomnia severity was assessed by the Insomnia Severity Index (ISI). Also, cortisol in saliva levels were monitored. Results: In the intervention group, significant shortening of mean sleep onset time, from 60-27 min (p<0.05) was observed, and a prolongation of mean sleep duration time, from 298-358 min (p<0.05), in neither case seen in the control group, although between-group difference was not statistically significant. Both PSQI and ISI means scores were significantly improved in the intervention group, from 12.1 to 7.9 (p<0.05) and from 19.4 to 12.5 (p<0.01), respectively, in the latter case significantly more so than in the control group (p<0.05). No effect on cortisol levels was detected, in either group. In conclusion, the tested eight-session CBT-based group intervention for insomnia appears to reduce severity and duration of insomnia, and to shorten time before falling asleep, when provided in primary care.
Keywords: Insomnia severity; Sleep duration; Cognitive behavioural therapy; Primary care; Group therapy
Insomnia is a major health problem in western societies. In Sweden a prevalence of up to 30% among women and 20% among men has been reported [1]. Also, the proportion of younger adults (20-30 years of age) appears to be increasing, and was doubled during the two last decades of the 20th century. In Sweden, with a total population of about 9.5 million inhabitants, around 4.5 million yearly prescriptions of different sleep medicines, by medical doctors, are performed [2]. Sleeping disorders stand for substantial suffer for the individual involved, as well as for excessive costs for the society.
Apart from pharmacological treatment, behavioural therapies have gained a stronger position in treating insomnia during recent decades, not least cognitive behavioural therapy (CBT) [3,4]. Studies comparing the effectiveness of CBT and pharmacologic treatment have shown CBT to be more effective in the longer perspective, to higher extent leading to persistent improvement of both sleep quality and difficulties in falling asleep [3,4]. Also, negative aspects of pharmacological treatment include unwanted side effects (such as day drowsiness, delayed reaction time and others) and for some substance groups risk for drug dependence, effects that may be avoided by using behavioural therapies instead. Although not all substance groups are associated with biological dependence, an element of psychological drug dependence may still appear.
A negative aspect of CBT and other behavioural therapies is that they are rather time consuming for the provider, putting high demands on necessary resources. Therefore, adequate accessibility may be difficult to achieve. For that reason alternative models to the traditional individual therapist-to-patient concept have been tried, including group-delivered and internet based CBT, both of which have shown promising results [5], as well in comparison with individual CBT as with pharmacological treatment.
A possible positive additive effect of group intervention, reported in previous studies, is the benefits gained from interaction with the other group participants [5-7]. For a majority of patients with insomnia, primary care is likely to be the natural primary instance to seek help if suffering from insomnia, and is thus of interest and importance when exploring effective ways to provide adequate treatment that meet the An apostrophe is lacking in patients needs.
The aim of the present study was to investigate the effect of a CBT based group intervention for insomnia in primary care, by means of self-reported sleep quality and duration. In addition, cortisol in saliva, as a biological marker of stress, was tested before and after the intervention.
The study was performed at four primary health care (PHC) units in the city of Linköping, Southeastern Sweden, during January 2009 to December 2011. At all four units a CBT-based group intervention for insomnia was implemented, giving the caregiver the possibility to refer patients with insomnia for inclusion in the study.
To be included the patients had to be aged >18 years and to suffer from insomnia, diagnosed by either a medical doctor or a psychotherapist at any of the involved PHC units. The insomnia could be newly debuted or having existed for a longer time (months to years), but should have persisted for at least one month, and could be either idiopathic or associated with perceived stress, mental exhaustion or overload. Ongoing pharmacological treatment for insomnia was no hinder for inclusion. However, if the patient had no ongoing sleep medication and was enrolled for the CBT group intervention, concomitant pharmacological treatment should not be initiated.
Insomnia directly associated with different pain conditions was an exclusion criterion, as was other diseases commonly followed by secondary sleeping disorder, including narcolepsy, obstructive sleep apnea syndrome (OSAS), restless legs syndrome, alcohol overconsumption, depression, primary anxiety conditions and depression. In addition to a clinical judgment of depression, all patients to be included were to fill-out the MADR-S (Montgomery-Åsberg Depression Rating Scale) form in order to exclude possible cases of depression not primarily identified by the doctor or the psychotherapist.
Participants for inclusion in the study group (given the intervention) were recruited consecutively during the first two years of the study. During the following final year, participants were instead recruited for inclusion in a control group, by the same inclusion criteria. Thus, no randomization between intervention and control was performed.
The CBT group intervention
Each group consisted of four to six patients. The CBT group intervention was led by a psychologist/psychotherapist (one of the authors, E.H.), and included eight two-hour long group sessions, the first four sessions held once a week, and the last four sessions two weeks apart.
The more frequent meetings during the first part of the intervention aimed to promote motivation and to enhance the process of change, while the latter part gave more time for exploring new habits, and to establish new ways of how to think and relate towards sleep. In case of drop-outs, no new participants were included in each group after initialization. The group sessions comprised a knowledge part, based on information on sleep related factors, a follow-up part with review of completed home tasks, and a final part introducing new tasks for completion until next session.
During the first half of the intervention, the goals were to map and describe the participants’ sleep disturbances, and to identify possible underlying reasons or circumstances contributing to maintaining them. To their assistance, the participants recorded sleep diaries, behaviour and activity diaries, thoroughly registering daily life activities.
In the second half of the intervention, individual goals and targets regarding measures that could contribute to improved sleep were set, and the sleep diaries used as a basis for group discussion and evaluation of effect. Finally, an individual maintenance plan, in which each participant described what they considered as the most important steps in their process of change, a document intended for them to be able to get back to in case the sleeping problem should return.
Control group
The participants in the control group consisted of patients who were prescribed a sleep medication for insomnia, either if the prescription was new for the patient (i.e. the patient had no ongoing sleep medication) or if a change in a previously prescribed sleep medication was decided (increase of dose or change to/addition of another medication).
Measurements
Prior to the CBT group intervention, the participants graded their sleep time and quality by filling-out the Pittsburgh Sleep Quality Index (PSQI) form [8,9], and estimated the severity of their sleeping problems by filling-out the Insomnia Severity Index (ISI) [10]. In both cases, measurement was then repeated directly (within maximum one week) and two months after the final group session, i.e. after having completed the intervention.
Apart from sleep estimation, cortisol in saliva was also measured before and directly after the intervention, as a possible biomarker of stress. Since the normal biological pattern for blood cortisol (reflected also in saliva) is a natural peak in the morning, at about half an hour after awakening, the saliva test was at each occasion taken twice: 1) directly after awakening, and 2) half an hour after awakening. An absence of a ≥50% increase in saliva cortisol level from the initial to the half-hour measurement was seen as an indication of possible stress [11,12].
The test was taken by the participants themselves, using the SalivaBio Oral Swab sample equipment (Salimetrics Inc., London, UK) by placing a saliva collection swab sublingually for two minutes, and then closing it in the sample tube. The samples were then to be brought to the PHC unit laboratory within three days, and should if not brought in during the same day be kept in refrigerator. After arrival to the laboratory, the test was centrifuged and frozen at -20° Celsius until analysis.
Fifty-six participants were initially enrolled in the study, 41 in the intervention group and 15 in the control group. Of the participants in the intervention group, six interrupted the intervention after one or two group sessions and were thus excluded from the study. Of the remaining 35 participants in the intervention group, 28 were women and seven were men, and in the control group the corresponding gender distribution was eleven women and four men.
The mean age was 54 years, ranging between 21 to 85 years. Main characteristics of the study population is shown in Table 1.
| Intervention group(n=35) | Control group(n=15) | Total(n=50) | |
|---|---|---|---|
| Gender (n):Female | 28 | 11 | 39 |
| Male | 7 | 4 | 11 |
| Mean age (years):Total | 54 | 54 | 54 |
| Females | 55 | 54 | 55 |
| Males | 48 | 56 | 51 |
| Baseline sleep characteristics: | Mean value (±SD) | Mean value (±SD) | Mean value (±SD) |
| Mean estimated time before falling asleep (minutes) | 60 (± 50) | 58 (±65) | 59 (±54) |
| Mean estimated total sleep time (minutes) | 298 (±62) | 325 (±54) | 306 (±61) |
| Mean PSQI score | 12.1 (±2.2) | 11.2 (±2.7) | 11.8 (±2.3) |
| Mean ISI total score | 19.4 (±3.7) | 17.3 (±4.7) | 18.7 (±4.1) |
Table 1: Main study population characteristics, by means of age and gender distribution, and characteristics of sleep estimates at baseline.
Sleep onset and duration
In Figure 1, the mean value of the participants estimated time before falling asleep, before and after the intervention, is presented. In the CBT intervention group, there was a significant shortening of the mean time interval (p<0.05). In the control group there was also a shortening of the mean time interval, however not as pronounced, and not statistically significant. Although there was a marked difference in mean time before falling asleep at follow up between the two groups, this showed not to be statistically significant.
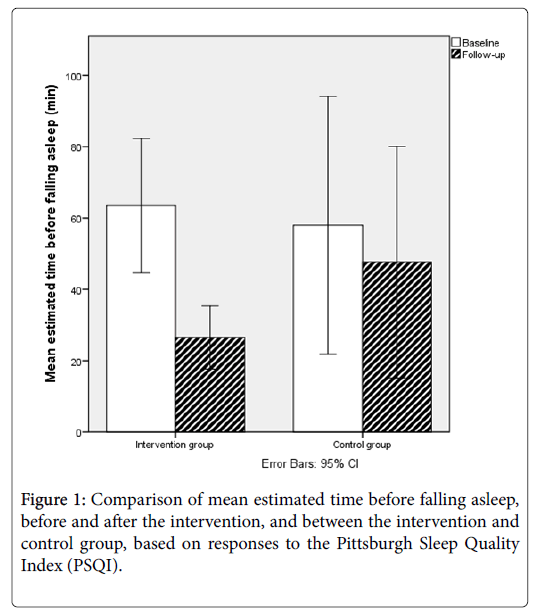
Figure 1: Comparison of mean estimated time before falling asleep, before and after the intervention, and between the intervention and control group, based on responses to the Pittsburgh Sleep Quality Index (PSQI).
Figure 2 shows the mean value of the participants’ estimated total sleeping time, before and after the intervention. In the CBT intervention group, the participants reported significantly prolonged duration of night sleep at follow-up (p<0.05). A corresponding, less pronounced and non-significant prolongation of sleeping time was seen in the control group. Neither was the difference between the groups statistically significant.
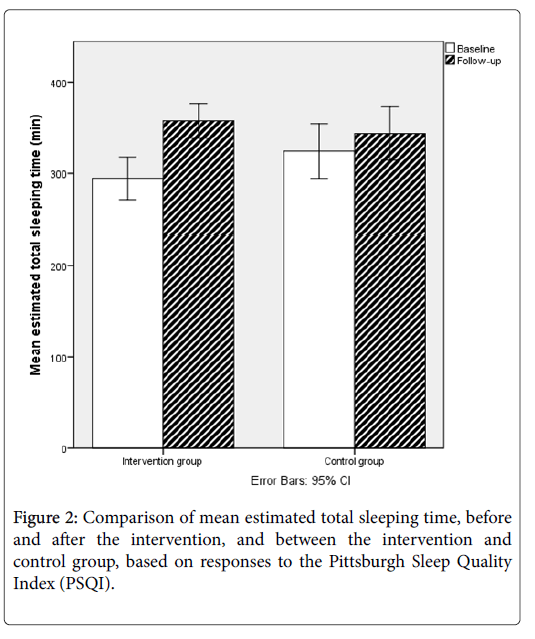
Figure 2: Comparison of mean estimated total sleeping time, before and after the intervention, and between the intervention and control group, based on responses to the Pittsburgh Sleep Quality Index (PSQI).
Sleep quality
The mean PSQI scores before and after the intervention is shown in Figure 3. In both the intervention and control group, the participants reported a significant improvement of sleep quality, reflected in a lowered PSQI score (p<0.05). Although seemingly somewhat more pronounced change in the CBT intervention group, the difference between the groups was not statistically significant.
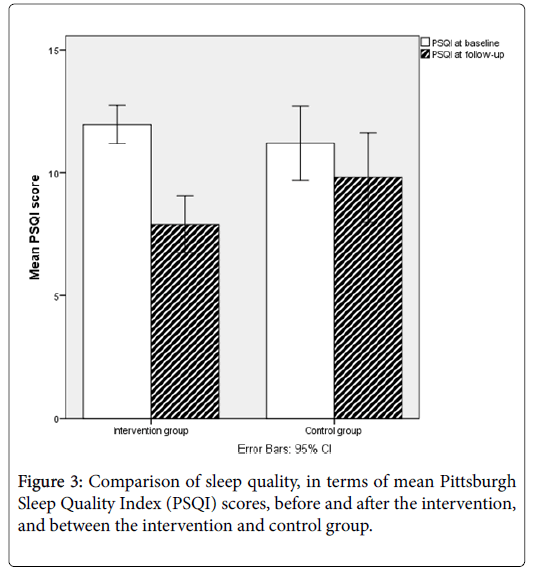
Figure 3: Comparison of sleep quality, in terms of mean Pittsburgh Sleep Quality Index (PSQI) scores, before and after the intervention, and between the intervention and control group.
Insomnia severity
The mean ISI scores before and after the intervention are shown in Figure 4. In the CBT intervention group, the participants reported a significantly lowered severity degree after the intervention (p<0.01). No corresponding difference was seen in the control group, and when comparing the ISI scores at follow-up, the ISI scores were significantly lower in the CBT intervention group than in the control group (p<0.05).
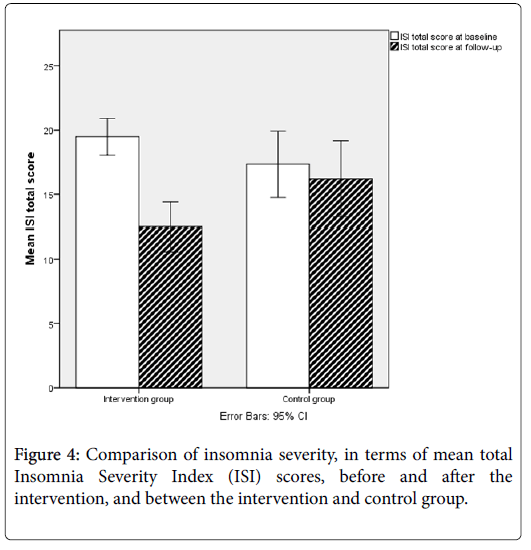
Figure 4: Comparison of insomnia severity, in terms of mean total Insomnia Severity Index (ISI) scores, before and after the intervention, and between the intervention and control group.
Regression analysis
In Table 2, odds ratios (OR) for improvement of sleep onset and duration, sleep quality (by means of PSQI score) and insomnia severity (by means of ISI score), when analyzed in a binary logistic regression model, using group, gender, age and baseline outcome within each field as covariates, in order to adjust for possible confounding effects of these. As seen in the table, being in the intervention group was the only variable significantly associated with improvement of any of the fields, namely insomnia severity, for which the OR against the control group was 15.5 (1.4-172.3 95% C.I.).
| Shortened sleep onset time OR(95% C.I.) | Prolonged total sleep time OR(95% C.I.) | Improved PSQI score OR(95% C.I.) | Improved ISI score OR(95% C.I.) | |
|---|---|---|---|---|
| Group (intervention group) | 3.1(0.6-16.5) | 3.5(0.8-16.4) | 4.9(0.8-20.9) | 15.5(1.4-172.3) |
| Gender (female) | 0.4(0.04-3.2) | 5.9(1.1-30.6) | 0.8(0.1-5.3) | 1.3(0.15-11.9) |
| Age (increasing) | 1(0.9-1.1) | 1(0.9-1.1) | 1(1.0-1.1) | 1(0.9-1.1) |
| Baseline value (less favourable) | 1.1(1.0-1.1) | 1(0.9-1.9) | 1.2(0.8-1.7) | 1.3(1.0-1.7) |
Table 2: Odds ratios (OR) and its 95% confidence intervals (C.I) for improvement of sleep onset and duration, and PSQI and ISI scorings, according to group (intervention/control), gender, age and baseline measurement outcome within each field, based on binary logistic regression analysis.
Cortisol in saliva
Expectedly, cortisol levels in saliva varied highly between individuals, ranging from 3 to >800 nmol/L (maximum measurement level). No significant difference between baseline and follow-up mean cortisol levels in either of the two groups could be observed. At baseline, 13 of 30 participants in the intervention group and six of twelve in the control group did not react with a with a ≥50% increase in saliva cortisol from awakening-test to test to half-hour test (the remaining eight participants had missing or incomplete saliva tests). At follow-up, the corresponding distribution was 15 of 30, and 3 of seven, respectively (tests missing or incomplete for 13 participants), showing no statistical significance in this respect.
In this study we have shown that a CBT-based group intervention for insomnia in primary care may be effective in improving individual sleep duration and quality. This is in line with what has been found in previous research, from which CBT for insomnia has strong evidence. The major advantage of the intervention in the previous study is the fact that it is group based, both making it more resource effective (with six patients in a group attending six group sessions equaling one visit for six patient receiving individual therapy), and also using the therapeutic benefits of group dynamics and sharing of experiences by other group participants.
The most pronounced sleeping improvements observed in the study were reduction of the estimated time before falling asleep and lowering of perceived insomnia severity. In the latter case, ISI decreased by about a third, a change that was not only markedly more pronounced than in the control group, but also of statistical significance when comparing the two groups. Estimated mean time before falling asleep more then halved in the intervention group, a result that also differed markedly from that of the control group, although not statistically significant. Lack of sufficient power due to the relatively low sample size, especially in the control group, is likely to be contributory to this.
Although viewed as a common and major public health problem in many countries, insomnia is still probably under-diagnosed [3]. It is known to be associated with increased morbidity in terms of both physical and psychological illness [13-15] and substantial impairment of quality of life [16,17] for those affected. Ciccone et al. illustrated that improvement of sleep quality can be associated with reversibility of related co-morbidity even on a micro morphological level, in this particular case for OSAS patients (having an established increased risk for cardiovascular disease) receiving Continuous Positive Airway Pressure (CPAP) treatment, for which significant improvement on endothelial function could be detected [17]. Moreover, insomnia is likely to have important impact on work capacity and sick leave, as suggested by DiBonaventura et al. [18]. Thus, both from an individual patient perspective, as well as on a community level, strategies for healthcare providers to adequately handle sleep disorders should be essential and of high priority. The heterogeneity of the general population brings a need for alternate treatment possibilities, of which a group based CBT approach may be one suitable alternative, depending on local resources and competence. The findings in our study provide some evidence for the method to be chosen when available.
Study limitations
The study has some major limitations, of which the small sample size must be considered to be the most important one. Especially this accounts for the control group, making reliable comparisons difficult to attain. Difficulties in recruiting participants to the control group was the main reason for this, together with a limitation of capacity to prolong the control group sample interval. The same recruitment difficulty may also have affected the results by means of possible selection bias, as is probably the case also in the study group. Another important limitation, also probably further contributing to this, is the circumstance that the study was non-randomized. However, the intention of the chosen study design was to mimic the clinical routine in the primary care context, as it is performed in reality, and to compare the intervention with how the patients would have been treated in the normal case, without the opportunity to provide the tested group intervention. This would not have been achieved if the participants had been randomized to any kind of alternative “placebo” or similar control intervention. However, conclusions from the study results should be drawn with caution, and to confirm the presented findings, further studies in a larger population would be needed.
In conclusion, the tested eight-session CBT group based intervention for insomnia appears to reduce severity and duration of insomnia, and to shorten time before falling asleep, when provided in primary healthcare.