Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Mini Review - (2015) Volume 5, Issue 2
Chimeric antigen receptors (CARs) are recombinant receptors that are expressed on autologous T-cells. CAR-T usage has grown in recent years as a way to combat hematological and solid tumors. The purpose of this review is to describe new studies on CAR-T treatment along with our lab’s ideas on potential uses and pitfalls that could be investigated. The usage of TREG and antiCLTA4 as means for regulating CAR-T will also be looked at along with OX40, CD137 and CD27 receptors as means for increasing the efficacy of the treatment overall. In addition the usage of iCasp9 as a ‘suicide switch’ for the CAR-T treatment and the potential for a 4th generation CAR will be touched upon. Then the review will lead into talks about how such a treatment could be of potential use in treating solid and hematological cancer.
<Keywords: Immunotherapy, Chimeric antigen receptors, CAR-T,
Immunotherapy research has long looked for a way to harness an individual’s own immune system to fight off tumors and cancers. Many ideas have made tried to make use of natural killer cells or B-cells, however research has not moved past conceptual thinking. However current research on chimeric antigen receptor T cells may change this. With several clinical trials already in place, CAR-T research is a growing field, with physicians and scientists looking for its expansion to a variety of cancers with cytokine storm cautious [1]. The idea behind CAR-T is the modified T-Cell. The patient’s own T-cells are harvested and then genetically modified to have a receptor for a particular antigen that a particular tumor cell may display. The particular antigen that has been used is CD-19, a common tumor antigen [2]. However without an initiating signal the CAR-T cells would remain naïve within the body. This signal is provided by dendritic cells. DC cells are professional antigen presenting cells that allow for a more directed immune response than B-cells could provide [3]. However DC cells cannot pick up the CD-19 antigen to present to the CAR-T cells because it is masked by the PD1-PDL1 interaction in tumor cells [4]. Naturally, the PD1-PDL1 interaction is used in the body to prevent the immune system from attacking a particular cell; for example, the PD1-PDL1 interaction prevents the mother’s immune system from attacking the fetus’s cells during pregnancy [5]. The tumor cells have harnessed this interaction to mask themselves from the body’s immune system. Breaking this interaction is a key component of CAR-T treatment as once done tumor cells would be vulnerable to the immune system [6]. The CAR-T’s function lies in providing an anti-PD1-anti-PDL1 interaction which would allow the tumor cell to be susceptible to the host’s immune system1 [7-17].
To combat solid tumors, the CAR-T treatment being designed must not only be specific and effective but also be administered within the window in which the patient is preconditioned [18-21]. New studies have however found that when used in combination with adenovirus Ad5Δ24, CAR-T therapy with anti-PD1/PDL1 and CLTA4 strategy can be more effective [1,19,22]. Ad5Δ24, an oncolytic virus that contains the chemokine RANTES along with IL15 cytokine has shown via the intratumoral release of these two substituents, to not only attract CAR-T cells to the tumor, but also promote their local survival in the immunosuppressive environment [19]. The non-HLA CAR-T target of stromal solid tumor (i.e. ErbB) has been in study [1]. By combining Ad5Δ24 with CAR-T treatment, while the study will need to progress further before clinical trials, it does shed light on the future of CAR-T cell therapy’s role in treating solid tumors.
Expression of OX40 will prevent CAR T-cells from dying and can maintain their immune response onwards to a memory response [23,24]. OX40 is required to further augment CD4 and CD8 priming. OX40 receptors can be promoted to be expressed in T cells first by the TCR engagement. The pitfall with OX40 however is the association of increasing cytokine production. OX40 binding has been shown to initiate cytokine storms in certain infections and will presumably add to the cytokine storm already made via CAR-T therapy [23]. CD137 and CD27 both TNF receptors, are expressed in the same fashion as OX40, generally within 24-48 hours after TCR engagement [25]. They also make use of the DC cells to promote the expression of their required ligand. CD137 is expressed by primarily CD8 cells [7]. CD137 acts as a co-stimulant that enhances T-cell proliferation and has been shown to enhance immune activity to eliminate tumors [26,27]. By allowing our CAR constructs to express CD137, we will increase the efficacy of the treatment. CD27 works in a similar fashion and is also a TNF receptor; however this works more towards maintaining T-cell immunity [23]. It also helps regulate B and DC cell activation, which can allow for further DC cell activation past the initial stimulation [23,24].
CAR-T treatment is fascinating prospect in the field of immunotherapy due to its potential uses. New research is being conducted as to improving current CAR constructs and minimizing on target, off tumor toxicities. Based on all the current research we can present an ideal CAR model (Figure 1). This model will include an anti-PD1 region, anti-CD19, and OX40, CD137 and CD27 co-stimulatory domains. In addition the CAR-T cell will have Treg and anti CLTA4 to regulate the CAR-T cell numbers and maintain a basal level. This CAR construct will also incorporate the iCasp9/AP1903 suicide gene technology as a self-withdrawal mechanism [28]. This ideal CAR construct would be used as a treatment that will be administered via intratumoral injection to maximize the efficacy and minimize any side effects. New research is being conducted on a similar kind of model by Zhu et al and the results of this study will help advance our knowledge about CAR-T treatment and better mold the ideal CAR construct [29,30].
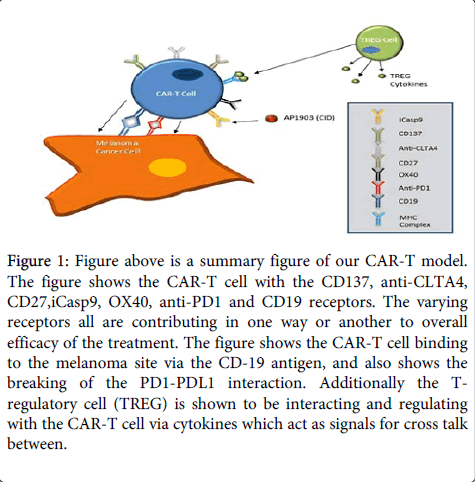
Figure 1: Figure above is a summary figure of our CAR-T model. The figure shows the CAR-T cell with the CD137, anti-CLTA4, CD27,iCasp9, OX40, anti-PD1 and CD19 receptors. The varying receptors all are contributing in one way or another to overall efficacy of the treatment. The figure shows the CAR-T cell binding to the melanoma site via the CD-19 antigen, and also shows the breaking of the PD1-PDL1 interaction. Additionally the Tregulatory cell (TREG) is shown to be interacting and regulating with the CAR-T cell via cytokines which act as signals for cross talk between.