Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Editorial - (2015) Volume 0, Issue 0
Understanding and treating cancer is one the top priorities in medical research. The use of chimeric antigen receptor T-cells (CAR-T) are increasing in popularity in the research and treatment of cancer due to their ability to utilize the expansion and killing effects of cytotoxic T cells while also having binding specificity through the chimeric antigen receptor (CAR). CAR expression and CAR-T expansion are critical for proper CAR-T functionality. Toxicity has been associated with the treatment of cancers with CAR-T however methods to control and decrease toxicity have been developed. While they first became popular for the treatment of B-cell lymphomas they are expanding to the treatment of other cancers. In this review we will discuss the current methods for CAR-T expansion, expression, and toxicity prevention while also covering current clinical applications of this therapy.
<Keywords: CAR-T, Clinical Applications, cancer, retroviral vector
Chimeric antigen receptor T-cells (CAR-T) are able to utilize the expansion and killing effects of cytotoxic T cells while also having binding specificity through the chimeric antigen receptor (CAR). CAR-T cells avoid issues common to T cell therapy such as the dependence on human leukocyte antigen (HLA) interactions for activation of T cell effector functions. HLA is often down regulated in cancer cells to promote immune system escape, which makes it more difficult for engineered T cells to activate an effector response [1]. The expression of CAR allows the T cell to shed its dependence on HLA mediated activation and elicit an effector response by binding to tumor specific surface proteins. The basic CAR consists of an antigen binding domain which is a single chain variable region antibody fragment (scFV), an extracellular domain, transmembrane domain and intracellular signaling domains. The intracellular domain is typically the CD3 ζ chain that is typically associated with the TCR complex. CAR-T is categorized in generations which increase as co-stimulatory molecules are added to its expression cassette. Co-stimulatory molecules enhance the efficacy and tumor trafficking of the CAR-T cell [2]. Fourth generation CAR-T contains a more specialized cassette of co-stimulatory molecules and other inhibitory molecules to control CAR-T proliferation in order to prevent CAR-T toxicity.
The CAR can be expressed through several different mechanisms including CAR encoding retroviral vector, mRNA transfection, lentiviral vector, transposon activity, and RNA electroporation. Lentiviral vectors transduce with non-dividing cells. These vectors completely and specifically integrate into the host genome with low immunogenicity which leads to permanent transgene expression. Low immunogenicity also endows lentiviral vectors the capacity to deliver larger DNA sequences and reduced susceptibility to silencing [2].
Another popular method for integrating the CAR gene in the T cell genome is the sleeping beauty transposon system. Sleeping Beauty (SB) is a transposon made synthetically and based on sequences of transpositionally inactive elements. SB is a superfamily transposon following a cut-and-paste transpositional reaction. In this reaction the element-encoded transposase interacts with its binding sites in the terminal inverted repeats of the transposon. This then promotes the excision of the element out of its donor site and its subsequent integration into the target DNA [3]. This method has also been adopted for DNA plasmid use for integration. Combining these two vectors yielded CAR-T cells with improved plasmid integration efficiency [4].
The preferred T cells to undergo expansion are those that are less differentiated. Expansion requires activating signals and appropriate growth environments. Stimulation signals have been summarized in Table 1 in the appendix. Figure 1 outlines the process of CAR-T expression and expansion.
| Signal | Description |
|---|---|
| OKT3 (anti-CD3 clone) | Can be used with anti-CD28 costimulating antibodies or activating cytokines (e.g. IL-2) |
| Anti-CD3/CD28 | Antibodies targeting activating/stimulatory domains to T cells |
| Bispecific T cell Engaging antibodies (BiTEs) | |
| IL-2/IL-21 | Cytokine known to induce clonal expansion of T Cells |
| Artificial antigen presenting cells | (e.g. Epstein-Barr virus) |
| (aAPCs) | Cells engineered to act as endogenous APCs would actàstimulating expansion of Tcells |
Table 1: Methods of CAR-T Cell Expansion [5].
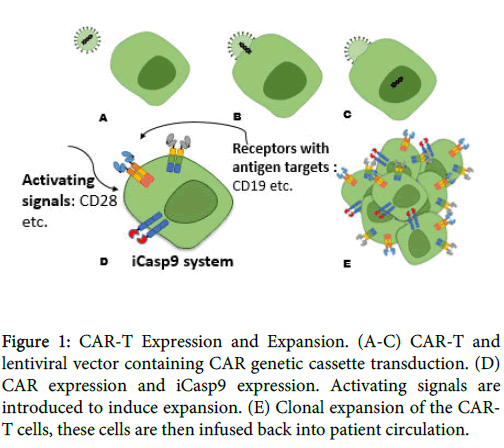
Figure 1: CAR-T Expression and Expansion. (A-C) CAR-T and lentiviral vector containing CAR genetic cassette transduction. (D) CAR expression and iCasp9 expression. Activating signals are introduced to induce expansion. (E) Clonal expansion of the CART cells, these cells are then infused back into patient circulation.
Anti-CD3/CD28 antibodies have shown better anti-tumor activity and better persistence following infusion. Ex vivo expansion using an antigen presenting cell (APC) may have a longer culture period but produce a larger amount of T cells capable of in vivo expansion post infusion [5]. A concept that has been noted to assist in T cell expansion is “Cytokine Sinks” [6]. This concept notes that depletion of lymphocytic cells (as seen with chemotherapy treatment) before CAR-T cell infusion facilitates their expansion without having to compete with endogenous lymphocytes for cytokine stimulation [7]. Late co-stimulatory signals from CD137 or OX40 can also aid in CAR-T activation by recruiting TNF family proteins [8]. This represents a different pathway than that of the signals provided by CD28.
After the T cells undergo ex vivo clonal expansion they are infused back into patient circulation where they undergo the process of “trafficking” in which they are directed to their site of action. Trafficking to the site of action can be mediated through overexpression of chemokines or molecules that will direct the CAR-T to its target site. At the appropriate tumor site, CAR-T cells must interact with the appropriate antigen, avoid inhibitory signals in the tumor microenvironment and maintain their effector function until the tumor has been eradicated. To avoid inhibitory signals and maintain their effector activity, CAR-T can be engineered to overexpress pro-survival signals, and infused with exogenous cytokines that promote expansion while avoiding T regulatory cell induction [9]. While treatment with CAR-T has shown promising results they have been shown to induce toxicity in patients through cytokine storm, autoimmune toxicity and macrophage activation syndrome which have resulted in death of participants in clinical trials [10].
On tumor off tumor toxicity is a continuous safety concern for targeted therapies and CAR-T cell treatment is not excluded. In addition to off tumor toxicity, CAR-T cells that use the retroviral method of expression run the risk of insertional mutagenesis and oncogenic expansion [5]. Some on-tumor on-target toxicities include: macrophage activation syndrome, cytokine release syndrome, and tumor lysis syndrome (TLS) [9]. TLS involves massive tumor cell lysis that releases large amounts of the tumors’ intracellular contents into systemic circulation. This often leads to hyperkalemia, hyperuricemia, hypophosphatemia, and hypocalcemia [9]. Macrophage activation syndrome denotes the condition where there is an increase in T cell expansion and elevated levels of macrophage activation in vivo. In vivo T cell clonal expansion and response to an antigen leads to a “cytokine storm”. This includes the presence of high levels of cytokines resulting in an elevated immune response (e.g. B cells, NK cells, macrophages, PMNs), inflammation, and tissue damage [3]. IL-6 is commonly elevated during a cytokine storm and at high levels can lead to trans-signaling (activation of cells not expressing IL-6 receptor).
Autoimmune toxicity or “on target, off tumor toxicity” occurs when the CAR-T attacks the correct antigen target but the tissue is non-malignant. The risk of autoimmune toxicity increases after treatment with checkpoint inhibitors. Symptoms range from mild (fever, nausea,) to severe (multiple organ failure, reflex tachycardia, death) [7].
Possible solutions include treatment with corticosteroids upon development of mild symptoms, target specific cytokine receptors in combination with treatment with CAR-T cells, and incorporation of the iCasp9 (inducible caspase 9) suicide gene. Tocilizumab is an anti-IL6R monoclonal antibody developed to help combat toxicity noted with CAR-T treatment of B cell acute lymphoblastic leukemia [2]. It has shown promising results in lowering toxicity without inhibiting the tumor killing effects of the CAR-T cell [2]. The human caspase genes are responsible for inducing cell death through apoptosis. Incorporation of the iCasp9 suicide gene using the CaspaCIDe system includes the iCasp9 and a small inert molecule that chemically induces dimerization (CID) like AP1903 [5]. Including this gene in the CAR-T expression cassette could serve as a safety switch for treatment of some cancers with high risks of CAR-T induced toxicities since only the T cells expressing this gene will undergo apoptosis upon introduction of the CID [5].
CD19 is the current hot target of CAR-T therapy. CD19 is a B lineage specific protein that regulates B lymphocytes activation and is expressed throughout all stages of B cell differentiation except for the hematopoietic stem cell and plasma cell stage [8]. The cell stage specific expression of CD19 makes it a good target for CAR-T treatment of B-lineage diseases. Although popular, CD19 is not the only focus of clinical trials that are making use of the CAR-T cell.
Epidermal growth factor receptor (EGFR) is another target for CAR-T therapy. EGFR is a member of the epidermal growth factor family of receptor tyrosine kinases (RTKs). There are four members of the EGFR family: ErbB2 (HER2/neu), ErbB3 (HER3), and ErbB4 (HER4). In many cancer cells, activation of EGFR leads to a signaling cascade that activates the oncogene KRAS, which is commonly mutated to a constitutively active form in oncogenic cells. [4]. Cancers involving KRAS mutations include pancreatic, adenocarcinomas, non-small cell lung cancer (NSCLC). Table 2 in the appendix outlines other current clinical trials involving CAR-T cells. Current clinical trials can be viewed on www.clinicaltrials.gov.
| CAR-T target* | Clinical Trials | Cancers** | Supplementary Reference |
|---|---|---|---|
| BCMA | NCT02215967 | Myeloma,Plasma-Cell/ Myeloma-Multiple | S21, S22, S23 |
| CEA | NCT02416466 | Liver Metastasis | |
| NCT02349724 | Lung, colorectal, gastric, breast, and pancreatic | ||
| CD19 + Mesothilin | NCT02465983 | Pancreatic Cancer | |
| CD 19 | (CD19 clinical trial information can be found in supplementary Table 1) | ||
| CD 20 | NCT01735604 | Hematopoietic/Lymphoid Cancer | S24 |
| CD 28 | NCT00881920 | Lymphoma/ Myeloma/ Leukemia | |
| CD 123 | NCT02159495 | AML | |
| CD 138 | NCT01886976 | Relapsed and/or Chemotherapy Resistant Multiple Myeloma | |
| Myeloma, toxicity noted: inflammation [5]. | |||
| CD171 | NCT02311621 | Neuroblastoma / Ganglioneuroblastoma | |
| CD30 | NCT02259556 | Hodgkin's Lymphoma | |
| NCT02274584 NCT01316146 | NHL | ||
| NCT01192464 | |||
| Note: Relapsed patients retain high CD30 expression making them good candidates for CAR-T targets[5]. | |||
| CD33 | NCT01864902 | Relapsed AML/ Chemotherapy Refractory AML | S4 |
| cMET | NCT01837602 | Metastatic BreastCancer/ Triple Negative Breast Cancer | |
| ROR1 | NCT02194374 | CLL/SLL | |
| EGFR | NCT01869166 | Advanced malignant gliomas, Advanced EGFR-positive Solid Tumors | |
| NCT02331693 | |||
| EGFRvIII | NCT01454596 | Malignant Glioma/ Glioblastoma/ Brain Cancer | S16, S17, S18, S19, S20 |
| GPC3 | NCT02395250 | Hepatocellular Carcinoma | |
| GD-2 | NCT02107963 | Sarcoma/ Osteosarcoma/ Rhabdomyosarcoma/ Neuroblastoma/ Melanoma | S1,S2,S3 |
| NCT01822652 | |||
| NCT01953900 | |||
| VEGFR2 | NCT01218867 | Metastatic cancer, metastatic melanoma, renal cancer | S11, S12, S13 |
| Mesothelin | NCT01897415 | Metastatic PDA | |
| NCT01583686 | Metastatic Cancer, Pancreatic Cancer, Mesothelioma, Ovarian Cancer | S14, S15 | |
| NCT02414269 | Malignant Pleural Disease/ Mesothelioma/ Metastases/ Lung Cancer/ Breast Cancer | ||
| NCT02159716 | Metastatic PDA/ | ||
| Epithelial Ovarian Cancer/ Malignant Epithelial Pleural Mesothelioma | |||
| NCT02388828 | LTSFU | ||
| HER-2 | NCT02442297 | Glioblastomas | |
| NCT01109095 | Glioblastoma Multiforme | S19 | |
| PSMA | NCT01140373 | Prostate Cancer | |
Table 2: Clinical trials on tumor antigen targets for CAR-T and their associated diseases. * All clinical trial information and supplementary references were obtained from clinicaltrials.gov. ** Abbreviations can be found in supplementary Table 2.