Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 2
The aim of this study is to estimate the frequency of personality disorders in patients with recurrent unipolar or bipolar affective disorders and the possible relationship of the categorical model with two dynamic psychopathological configurations. Forty-eight patients were studied using semi-structured interviews for assessing Axis I and Axis II disorders. We found that approximately 70% of patients had some types of personality disorder according to the DSM-IV TR classification model. The most frequent personality disorders were cluster C dependent personality disorder and cluster B borderline personality disorder. The most common affective disorders were depressive bipolar I subtype disorder and manic bipolar I subtype disorder. The high frequency of personality disorders in patients who are in partial or complete remission of recurrent affective disorders can be explained by a combination of two subtypes of psycho-pathological configurations (the anaclitic or introjective configurations are based on the Blatt model) and neuro-biological interactions.
Keywords: Affective disorders, Personality disorders, Comorbidity, Psycho-pathological models, Anaclitic-introjective
The purpose of this study is to investigate whether there is a relationship between recurrent affective disorders classified as Axis I by Diagnostic and Statistical manual of Mental Disorders Fourth Edition (DSM-IV TM) and personality disorders classified as Axis II of the same manual [1]. This association has not been completely resolved as numerous studies have shown varying temporal associations (comorbidity) between recurrent affective disorders and personality disorders [2-6]. In psychiatry, the dimensional theory, which is used for assessments, considers personality disorders as clinical forms of recurrent affective disorders. This is especially true for borderline personality disorder (BPD). Other researchers consider it useful to promote BPD as Axis I of DSM-IV, anyway this approach could be not longer tenable because of DSM-5 section III dimensional model and no ‘’split’’ between Axis I-Axis II [7-9].
Classification of temperament traits (neurobiological and affective components of personality disorders) creates even more confusion. According to the Akiskal model [10-14]; some personality disorder subtypes appear as forms of syndromic or subsyndromic variants of affective disorders. Personality disorders seem to be reduced to four basic temperaments: 1) depressive; 2) hyperthymic, in which a person has a tendency to be in a euphoric mood; 3) cyclothymic oscillations between depression and an upbeat mood; and 4) irritable-explosive. The dimensional model may be useful to reduce countless nosological clinical symptoms and to study neurochemical, neuropshysiological (adding sleep and circadian pattern abnormalities) and pharmacological basics. It also leads to poor psychopathological specificity. For instance, some researchers consider cyclothymia or hypomanic personality disorder as a personality disorder, while other researchers judge these as a level of mood disorder [11,15,16].
The relationship between psychopathological states and abnormal traits of character is not a new issue. It appears in both classical psychiatry and in its most dynamic versions. The history of psychiatry goes back to the Hippocratic school trying to relate the prevalence of humors (black, yellow, sanguine, phlegmatic bile) with temperament and personality. Phlegmatic temperament and its blood type were related to the predisposition for four diseases: mania, melancholia, phrenitis or paranoia [17]. Kraepelin described several affective states, known as manic-depressive psychosis. This classification laid the basis for recognizing psychopathological subsyndromal states based on observable fluctuations in motor activity, emotions and thoughts (cognitions). Kraepelin, quoted by Akiskal, considered these manifestations temperamental (1992). From a dynamic point of view, [18] found that patients suffering from melancholy after the end of the episode also showed an obsessive-compulsive character.
Freud studied melancholy and considered the existence of "a pathological predisposition" that led to melancholy instead of mourning. He proposed a narcissistic type of relationship with the object, which now may apply to patients from cluster B (American Psychiatric Association, 1994) [1]. Freud seemed to relate melancholy with obsessional neurosis due to the degree of ambivalence present in both conditions and referred to it as " obsessive depression" [19].
Recent studies [5,20] have evaluated that BPD is a personality disorder that shows higher percentage of comorbidity with type I and type II bipolar disorder (BD I and II) compared to the other disorders of axis II (19.4% vs. 7.4% respectively). Moreover, the emergence of "new episodes" of type I and II BD occurs more frequently in BPD compared to other personality disorders (OPD) with percentages reaching 8.2% vs. 3% respectively. More proof of the disagreement among researchers, Kernberg [16] proposed that during bipolar illness (though bipolar subtype was not mentioned), patients may suffer from borderline personality organization (BPO), psychosis, neurosis and even a normal personality. One of the authors of this study (DC) found that, in clinical psychiatry, one of the most difficult differential diagnosis is between BPO hypomanic/cyclothymic subtypes and type I or II bipolar disorder with severe impulsivity, affective instability and chaotic relationships that continue after remission of each acute episode [21].
This research is a preliminary attempt to establish correlations between cyclic affective disorders and all axis II disorders. Establishing the relationship between character traits and psychopathological conditions may be important from the following points of view: 1) prediction; 2) form and duration of psychotherapeutic and psychopharmacological treatment; 3) prevention of complications during treatment (suicide, psychotic episodes, severe regressions); and 4) the treatment of patients with a diagnosis on Axis I usually have more complications when accompanied by an Axis II disorder [22].
The following is a prospective, observational and cross-sectional study of patients diagnosed with bipolar disorder in two health centers in the city of Buenos Aires: Borda Hospital and Italian Hospital between September 2009 and June 2010.
Inclusion criteria: 1) patients of either sex between 18 and 65 years old; and 2) patient still undergoing outpatient treatment with a presumed diagnosis of recurrent affective disorders (unipolar, bipolar, mixed and rapid cycling). Exclusion criteria: 1) patients with evidence or clinical history of organic mental disorder according to DSM-IV TM; 2) patients who presented with substance and/or alcohol use disorder at the time of the study diagnosis; 3) patients diagnosed with dysthymia and 4) patients who refused to complete the informed agreement. Patients with incomplete questionnaire data (n=2) were removed from the statistical analysis.
The Structured Clinical Interview for DSM-IV Axis I Disorders User´s Guide Clinical, Version (SCID I) was used as a screening and diagnostic tool. In the second phase of the study, the Structured Clinical Interview for DSM-IV axis II Personality Disorders (SCID-II) was used in order to typify the possible personality disorder (both interview were translated to Spanish and validated version applied) [23,24]. At the time of assessment, all demographics and medication information were recorded on a separate sheet.
Each interview was conducted by psychiatrists trained in the use of assessment tools and experienced in treating patients with personality disorder. The interviews were supervised by a principal investigator to avoid misunderstandings and to make the final forms.
Variables considered in the analysis were: age, gender, type of Axis I disorder (recurrent depressive disorder; bipolar disorder type I, most recent manic or depressive episode; bipolar disorder type II, most recent hypomanic or depressive episode; bipolar disorder type I, unspecified; and recurrent unipolar disorder), type of Axis II disorder and pharmacologic treatment (this last variable was not illustrated and subsequently was not part of the research objectives).
The data were entered in an Excel Microsoft 2000 spreadsheet (version 9.0.2812) and were analyzed using the statistical package Epi Info 2000 version 1.1.2 (CDC and WHO). For all variables, the distribution of frequencies and/or percentages was established relative to the total number of cases. Statistical analysis consisted of a quantitative analysis from measures of central tendency and dispersion, yielding proportions, averages, ranges, medium or standard deviation as appropriate for each variable studied. Smith Statistical Package (v. 2.80, 2005) was used for analysis of confidence intervals.
The study group included 48 patients, of whom 50% (n=24, CI=0.35 to 0.64) were female and 50% (n=24, CI=0.35 to 0.64) were male. The patients were aged between 23 and 65 years with a mean of 47 ± 13.42 years.
Of the patients, 35.41% (n=17, CI=0.21 to 0.49) were diagnosed as type I BD with the most recent episode being a depressive state. Twenty-seven percent (n=13, CI=0.14 to 0.40) received a diagnosis of BD I with the most recent episode being a manic state. Only 8% (n=4, CI=0.0022 to 0.16) presented with the most recent episode being a mixed state. Finally, only one patient displayed with the most recent episode being hypomanic and one patient had an unspecified episode (CI=-0.021-0.06 for each). Of the patients, 10.41% (n=5, CI=0.014 to 0.19) were diagnosed as type II BD with the most recent episode being depressive and three patients most recently had a hypomanic episode (CI=-0.085 to 0.13). Eight percent (n=4, CI=0.0022-0.16) received a diagnosis of recurrent depressive disorder (unipolar depression). Data can be viewed in Table 1 and graphic bar 1 (Figure 1).
| Diagnosis | Frequency |
|---|---|
| BPD. Depressive Type I (N=17) IC=0.21-0.49 | 35.41% |
| BPD. Manic Type I. (N=13) IC=01.14-0.40 | 27.00% |
| BPD. Mix Type I. (N=4) IC=0.0022-0.16 | 8.00% |
| BPD. Type IHypomaniac. (N=1) IC=0.021-0.06 | 2.00% |
| BPD. Type I Not Specified. (N=1) IC=0.021-0.06 | 2.00% |
| BPD. Depressive Type II. (N=5) IC=0.014-0.19 | 10.41% |
| BPD. Type II Hypomaniac. (N=3) IC=-0.215 | 6.25% |
| DPD. Recurring. (N=4) IC=0.0022-0.16 | 8.00% |
Table 1: Percentage of patients with recurrent affective disorders.
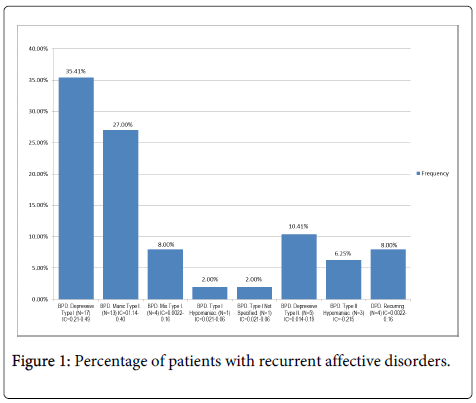
Figure 1: Percentage of patients with recurrent affective disorders.
Regarding personality disorders, nearly 23% (n=11, CI=0.33 to 0.62) did not display a personality disorder, while 77% were positive for any personality disorder (n=37, CI=0.64 to 0.89). About 27% of the patients positive for axis II disorders (n=10, CI=0.12 to 0.42) had comorbidity with other disorders on axis II.
Among those who had only one diagnosis, the majority presented with a dependent personality disorder (21%, n=8, CI=0.077 to 0.35), followed by 16% with BPD (n=6, CI=0.037 to 0.28), 11% each with histrionic and obsessive compulsive disorder (n=4, CI=.031 to .21) and finally 5.4% with narcissist disorder (n=2, CI=-0.02 to 0.13). Only one patient had avoidant or schizotypal or unspecified disorder (n=1, CI=-0.02 to 0.08). Data can be viewed in Table 2 and graphic bar 2 (Figure 2).
| Diagnosis | Frequency |
|---|---|
| Without PD (N=11) IC=0.33-0.62 | 22.90% |
| With PD (N=37) IC=0.64-0.89 | 77.10% |
| Dependent (N=8) IC=0.077-0.35 | 21.00% |
| Limit (N=6) IC=0.037-0.28 | 16.00% |
| Histrionic (N=4) IC=0.031-0.21 | 11.00% |
| Obsessive Compulsive (N=4) IC=0.031-0.21 | 11.00% |
| Narcissistic (N=2) IC=-0.15 | 5.40% |
| Avoidant (N=1) IC=-0.1 | 2.70% |
| Schizotypal (N=1) IC=-0.1 | 2.70% |
| Not Specified (N=1) IC=-0.1 | 2.70% |
Table 2: Estimated percentage of patients with personality disorder in patients who had recurrent affective disorders.
Figure 2: Estimated percentage of patients with personality disorder in patients who had recurrent affective disorders.
A high percentage of personality disorders were found in patients who were in complete or partial remission of recurrent affective disorders according to DSM-IV TM diagnostic criteria. This data is generally consistent with current literature reviews. A high degree of variability in the rates of comorbidity is similar to our findings with the largest association in cluster C Axis II disorders. This is especially true for dependent personality disorder and BPD (Table 2 and graphic bar of Figure 2). This association may have a variety of predisposing factors including: a) neurobiological (including the well-known sleep disorganization in affective disorders); b) genetic (as a diathesis toward affective, impulsive and interpersonal relationships or as a personality trait among various affective disorders); c) psychosocial; d) life special cycle period in women like postpartum [25] and d) a combination resulting in the interaction of these factors [26]. We hypothesize that points b, c and could be related to BD in parents and the tendency of their offsprings to show more sleep problems, aggressive behavior, ADHD diagnosis and emotional reactivity all features that could also be related to personality disorders traits in adolescence, the known onset of BD [27].
In the subgroup of patients with mood disorders without personality disorders (a figure close to 25% in our research) it could be considered part of the neurobiological dominance hypothesis. Affective disorders could be an example of severe emotional deregulation and sometimes cover the cognitive dimension. So the older term "manic-depressive psychosis” is still useful [28].
In this paper, we suggest the high correlation responds to a high index of Axis I- Axis II association. From a theoretical point of view, a relationship can be established between the depression model investigated by Blatt [29] and subtypes of personality disorders. Blatt considers two essential psychopathological configurations, which are presented in a continuous of immaturity towards higher levels of personality integration. These configurations are the anaclitic and the introjective types.
In the first type, the central conflict is about the nature and quality of interpersonal relationships. Anaclitic psychopathology derives mainly from difficulties in achieving and maintaining deep and meaningful relationships. Critical is finding appropriate objects that give integration to the self (“libido is seeking for object rather than instinctual gratification”, [30]. According to Blatt, this psychopathological predisposition can span from undifferentiated schizophrenia to personality disorders such as dependent, borderline and anaclitic depression (abandon depression) [31].
In this study, approximately 48% of patients have the anaclitic configuration with respect to personality disorders and in a majority of the cases it is associated with some mood disorder. We suggest that the personality disorder in this situation would also be associated with biological predisposition. The disruption of attachment (the neurobiological underpinning of relationships) or their inevitable transformations leads these patients to more depression or as a defense have manic/ hypomanic episodes. In the latter situation, there is a tendency to confirm, at least theoretically Kleinian hypothesizes the occurrence of mania as a defense against depression and object dependency [18,19,32,33] anticipates this configuration and its relationship to the blues. He considers three fundamental premises in this condition: 1) object loss; 2) ambivalence; and 3) the regression of the libido to the self. In short, according to Blatt’s model, the anaclitic configuration (including a form of depression) is characterized by: feelings of hopelessness, emptiness and abandon anxieties with desperate desire to maintain physical/emotional contact with objects.
Instead, in the introjective type of organization has a particularly intense interest about defining personal and individual achievement and the maintenance of highly differentiated limits of self-respect. It correlates to Blatt's subtype, the DSM-IV obsessive-compulsive personality disorder and the narcissistic personality disorder subtype. In our study, the prevalence of these clinical forms was lower (11% and 4, 5 % respectively).
In summary, our study confirms high rates of association between Axis I mood disorders and Axis II disorders (psycho-pathological trait). The separation between the axes should be reconsidered beyond neurobiological etiologies. Recurrent affective disorders are associated with non-integrated forms of relationships with significant others, along with difficulties in maintaining self-esteem and problems with self/other differentiation (anaclitic and introjective pathology respectively). These results should be taken as preliminary findings mainly due to: 1) low number of cases studied, b) cross sectional rather than longitudinal observation, 3) absence of randomization, 4) no control group, 5) the proposed Blatt model would not explain all manic/hypomanic episodes unless they can be considered as a defense against depression or painful and unsuccessful attempts to restart the relation with the object in front of a threat of abandonment in anaclitic organization.
To Martín Ruiz, M.D., Cintia Pereira, Psych and Carolina Vairo for patients provition.