Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Review Article - (2015) Volume 3, Issue 1
Brentuximab Vedotin., an anti-CD30 antibody drug conjugate (ADC) received FDA approval in 2011 for the treatment of relapsed/refractory Hodgkin's lymphoma and anaplastic large cell lymphoma based on 100% CD30 expression. In this review, we have discussed the various trials of Brentuximab Vedotin.in diffuse large B-cell lymphoma. Brentuximab Vedotin.is an ADC of monoclonal antibody conjugated with Monomethyl Auristatin E (MMAE), a microtubule inhibitor and hence facilitates selective delivery of potent MMAE to only the CD30 positive cells avoiding any off-target side effects. CD30 has restricted expression in normal tissues. According to the current trials, there does not seem to be an association between the efficacy of Brentuximab Vedotin and CD30 expression levels. Prospective trials are required to test the efficacy of Brentuximab Vedotin in diffuse large B-cell lymphoma and other malignancies and determine if CD30 positivity of tissue samples should be tested before administering Brentuximab Vedotin.
Keywords: Brentuximab vedotin; CD30; Diffuse Large B-cell Lymphoma
The most common type of B-cell non-Hodgkin lymphoma (NHL) is diffuse large B-cell lymphoma (DLBCL), which has an aggressive clinical course. Diffuse large B-cell lymphoma accounts for approximately 30-40% of those diagnosed with NHL in the United States every year [1]. Recent reports suggest a steady increase in the incidence of DLBCL, a trend that is currently independent of the human immunodeficiency virus (HIV) infection [2]. The clinical outcome of DLBCL patients has improved over the decades as a result of better understanding of lymphoma biology, advances in diagnostic and prognostic stratification using immunophenotyping, cytogenetics and gene expression profiling (GEP) studies, and advances in radionucleotide staging. CD30, a member of the tumor necrosis factor receptor family (TNFR super family 8) is involved in the activation of the canonical nuclear factor NF-κB pathway and provides tumor cell survival signaling [3,4]. Expression of CD30 is restricted in normal tissue, and CD30 is expressed in almost 100% of the Hodgkin and Reed Sternberg (HRS) cells and anaplastic large cell lymphoma (ALCL), thus serving as an attractive target of immunotherapy for classical Hodgkin Lymphoma (cHL) and ALCL [5,6]. There is a growing need to further characterize primary refractory or relapsed DLBCL at the molecular level in an attempt to identify biomarkers predictive of response to salvage therapies, to better understand the mechanisms associated with acquired resistance to immunochemotherapy, and to identify and develop therapeutic strategies against novel targets and/or pathways. Unless contraindicated by significant pre-existing co-morbid conditions, the treatment of DLBCL includes the use of rituximab and anthracycline based-multi agent chemotherapy, the aim of which is to achieve a durable complete remission (CR)? The treatment is subsequently tailored according to the stage or bulk of disease, and response to therapy. Using current rituximab-based chemotherapeutic modalities, the cure rate of DLBCL is 65% [7]. The International Prognostic Index ( IPI scoring) remains prognostic in the rituximab era. Developed in the 1990s, the IPI is the most functional clinical tool used to predict outcomes for patients with DLBCL [8]. A question was raised whether IPI remains prognostic in the rituximab era. A retrospective analysis was conducted by Sehn et al. on patients with DLBCL treated with RCHOP and outcome categories were redefined, termed the revised IPI, which was a more clinically useful predictor of outcome than the IPI in this population [9]. All groups had a predicted 4-year overall survival (OS) greater than 50%. A more recent analysis of more than 1000 patients treated with chemo-immunotherapy suggests that the IPI is useful in the rituximab era for predicting event-free survival (EFS), progression-free survival (PFS) and overall survival (OS) [10]. The IPI continues to be an important tool for clinicians to use to risk-stratify patients and to provide the prognostic information that is requested by patients during consultation. While addition of rituximab to standard doses of cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP) chemotherapy has improved the outcomes of patients with DLBCL, a significant number of patients fail to respond or relapse, thus stressing the need to develop novel therapeutic strategies.
Antibody drug conjugates are a relatively new discovery for the treatment of tumors. In the past, monoclonal antibodies have been approved by the Food and Drug Administration (FDA) for the treatment of tumors like follicular lymphoma ( rituximab) and breast cancer ( transtuzumab). In the recent past, there has been an increased focus on development of antibody conjugates. Various attempts have been made in testing of combinations of antibodies with radioisotopes or combinations of antibodies with chemotherapies. The rationale for these combination therapies is- “selected delivery of the drug to the tumor cells with receptor positivity”. US FDA has approved 2 agents: ibritumomab tiuxetan and 131-I tositumomab for the treatment of relapsed B-cell lymphomas [11-14]. Antibodies can also be modified so that they are conjugated with chemotherapeutic drugs and this facilitates selective delivery of the drug to certain tumor cells [15-18]. This idea has also been utilized for the development of gemtuzumab ozogamicin which is the first antibody drug-conjugate (ADC) to be approved for the treatment of cancer. However, it had to be withdrawn from the market in 2010 for lack of efficacy and increased mortality [19]. Despite the initial setback faced with the first antibody drug conjugate, ADCs still appear to be playing a significant role in the cancer treatment [20].
CD30 was discovered in 1982 [21] and was identified as a member of the TNF superfamily which consists of 25 members. It is expressed on all Reed Sternberg (RS) cells and functions as an integral membrane glycoprotein. CD30 is expressed in 98.4% Hodgkin lymphoma (HL) cases, and also in some other hematological malignancies, notably ALCL. Expression of CD30 is restricted in normal tissue—it is only found in thymocytes during thymic development, decidual cells of the pregnant uterus and endometrium, pancreatic exocrine cells and a subset of activated lymphocytes -both B and T (CD4+ and CD8+) cells — making it a good immunotherapy target that is unlikely to have many ‘off target’ side effects [22,23].
Signaling through the TNFR superfamily of molecules affects cellular proliferation, survival, and differentiation, and these effects are mediated through the cytoplasmic domains of the receptors [24,25]. TNFR1 and Fas contain an 80-amino-acid motif, designated the death domain, that induces apoptosis through interaction with Fasassociated death domain (FADD) and TNFR-associated death domain (TRADD), which in turn recruit caspases to initiate the apoptotic cascade. In contrast, TNFR1 can activate NF-κB to prevent cell death through the interaction of TNFR1, TRADD, and TNFR-associated factor 2 (TRAF2). CD30 signaling results in pleiotropic effects depending on the microenvironment within which the cell resides. CD30 does not contain a death domain but is able to produce an apoptotic stimulus. The mechanism for this effect is thought to be related to the degradation of TNF receptor-associated factor-2 (TRAF2), thus preventing its interaction with the TNFR1-TRADD complex, thereby enhancing death signaling through the TNFR. CD30 ligand and monoclonal antibodies that interact with this signaling portion of the molecule are thought to induce apoptosis by initiating CD30 signaling without NF-κB activation. The constitutive NF-κB activity associated with cHL prevents the apoptosis induced in ALCL [26].
Brentuximab vedotin targets CD30 receptor and delivers highly toxic chemotherapeutic drug Monomethyl auristatin E (MMAE) that cannot be delivered systemically. Brentuximab vedotin consists of the monoclonal antibody cAC10 modified by the addition of a dipeptide protease-sensitive linker to permit attachment to MMAE. Monomethyl auristatin E is a synthetic analogue of dolastatin 10, a natural product isolated from Dolabella Auriculara (Indian Ocean sea hare) which acts as a potent anti-tubulin agent. The linker is composed of citrulline and valine. There are 4 molecules of MMAE per molecule of the monoclonal antibody. The dipeptide linker provides maximal serum stability with efficient hydrolysis and release by human cathepsin B [27]. Figure 1 shows the structure of brentuximab vedotin.
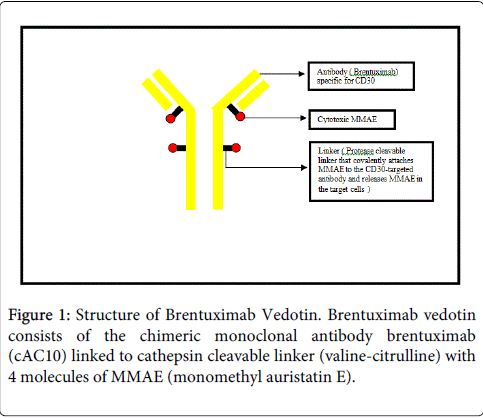
Figure 1: Structure of Brentuximab Vedotin. Brentuximab vedotin consists of the chimeric monoclonal antibody brentuximab (cAC10) linked to cathepsin cleavable linker (valine-citrulline) with 4 molecules of MMAE (monomethyl auristatin E).
Mechanism of action of Brentuximab Vedotin
Brentuximab vedotin is internalized through clathrin-mediated endocytosis into a lysosome and the dipeptide linker is cleaved through the action of cathepsin B in the lysosome and MMAE gets released. The MMAE prevents microtubule polymerization and also diffuses out of the cell because of membrane permeability to exert its action on the surrounding CD30 negative bystander cells. This latter event significantly contributes to its action [15].
There are different mechanisms by which brentuximab vedotin acts on the HRS cells and the ALCL cells. In ALCL, the CD30 monoclonal antibody binds to the cells which express CD30 and thus causes apoptosis through CD30 targeting also in addition to the cytotoxic effect of MMAE released within the malignant cells. However, in the HRS cells, CD30 binding delivers a proliferative signal and could potentially increase the therapeutic effect of intracellular MMAE by preventing apoptosis in a cell that has been stimulated to proliferate. This has special relevance for Hodgkin lymphoma, in which the inflammatory and immune cells that make up most of the tumor mass provide growth factor support and help the malignant HRS cells avoid immune recognition [26,28,29]. Figure 2 shows the mechanism of action of brentuximab vedotin.
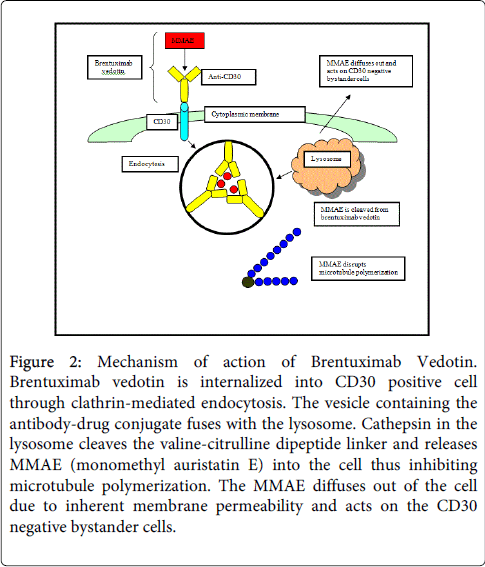
Figure 2: Mechanism of action of Brentuximab Vedotin. Brentuximab vedotin is internalized into CD30 positive cell through clathrin-mediated endocytosis. The vesicle containing the antibody-drug conjugate fuses with the lysosome. Cathepsin in the lysosome cleaves the valine-citrulline dipeptide linker and releases MMAE (monomethyl auristatin E) into the cell thus inhibiting microtubule polymerization. The MMAE diffuses out of the cell due to inherent membrane permeability and acts on the CD30 negative bystander cells.
Preclinical Studies
It was observed in the preclinical studies that the increases in exposure to the ADC and free MMAE were approximately proportional to dose. The median time to maximum concentration occurred immediately after infusion for the ADC and approximately 2 to 3 days after infusion for MMAE. Steady-state pharmacokinetics for both the ADC and MMAE occurred by approximately 21 days, consistent with the half-life estimates of 4 to 6 days and 3 to 4 days, respectively. The stability of the dipeptide linker was confirmed, with less than 2% of the MMAE being released when the ADC was incubated with human serum over a 10 day period. The peak plasma concentration attained by brentuximab vedotin is 30 mcg/ml.
On exposing HL cell lines to the ADC, apoptosis and DNA fragmentation began within 12 hours of drug exposure [30]. Brentuximab Vedotin performed well in further in-vitro studies, causing growth arrest and apoptotic cell death in CD30+ cell lines (HL and ALCL). It has been shown that Brentuximab Vedotin internalizes within 48 hours of binding to cell surface CD30 (faster in vivo than in vitro) [31], and the release of the MMAE from the antibody occurs within 24 hours of the internalization allowing a much higher MMAE concentration within the cells than the ADC concentration administered [32]. The MMAE released into the cells after cleavage of the dipeptide linker seems to be able to diffuse out of viable HL cells and exert it’s cytotoxic effect on bystander cells [32]. This proves to be significant in the regression of a tumor such as HL where the malignant cells targeted constitute a very small percentage of the total tumor volume.
Phase I studies in CD30 positive lymphomas
The results of the first multicenter phase I open label trial of brentuximab vedotin in relapsed/refractory HL has been published. The study comprised of 45 patients of which 42 patients had HL and ALCL. An objective clinical response of 38% was observed with 24% complete response (CR) [33].
Another phase I multicenter study comprised of 44 patients consisting of HL and ALCL, the observed overall response rate (ORR) was 59% with CR of 34% [34].
Phase II studies in CD30 positive lymphomas
In a large phase II single arm multicenter study, 102 heavily pretreated patients with HL who had relapsed after autologous stem cell transplant (ASCT) were treated with brentuximab vedotin. The majority of the patients had primary refractory disease. The ORR was 75% (76/102) with 34% CR (35/102) and 40% partial response (PR) (41/102) [35].
In another phase II multicenter study consisting of 58 patients with relapsed/ refractory ALCL, the ORR was 86% with CR of 57% and PR of 29% [36].
Hence, brentuximab vedotin received FDA approval for the management of relapsed/refractory Hodgkin lymphoma and anaplastic large cell lymphoma in August 2011.
Combination with chemotherapy
Using mouse xenograft models of HL, brentuximab vedotin has been combined with chemotherapy. With adriamycin, bleomycin, vinblastine and dacarbazine (ABVD) and gemcitabine, the effects appear synergistic. However with vinorelbine no additional effect was evident [37].
This study provided a good rationale for taking the combination of brentuximab vedotin with certain chemotherapeutic agents into the clinical trial setting in the future, however given the high response rates achievable with first line therapy, this may be more suitable to either the relapsed/refractory HL population or more elderly patients who are unable to tolerate standard chemotherapy.
Potential for re-treatment
It has been shown by multiple clinical experiences in the past that brentuximab vedotin does have clinical efficacy despite multiple retreatments. A case series presented at ASCO in 2010 describes patients relapsing following brentuximab vedotin and being re-treated with the drug. Seven patients had 8 re-treatments and all experienced tumor regression.
The role of brentuximab vedotin is being evaluated in a number of other trials. The AETHERA (High Risk of Residual Hodgkin Lymphoma Following Stem Cell Transplant) trial is a Phase III randomized, double-blind, placebo-controlled study of brentuximab vedotin and best supportive care versus placebo and best supportive care. In patients receiving the study drug, interim results show 75% of patients having achieved an objective response, with 34% and 40% of patients achieving complete and partial remission, respectively. Tumor reductions were noted in 94% of the patients [38]. In addition to being the focus of the AETHERA trial, brentuximab vedotin is being studied in combination with multiagent chemotherapy in the treatment of HL and ALCL.
Management of relapsed/refractory DLBCL poses a therapeutic challenge. It has been observed in 3 independent studies, that the CD30 expression in DLBCL varies from 14-25% [39-41]. Whether CD30 expression confers a prognostic value in DLBCL is debatable. A question of interest to be answered is whether brentuximab vedotin could be used in the treatment of CD30 positive DLBCL, and hence prove to be a potential therapy for relapsed/ refractory cases. A phase II study is going on to evaluate the anti-tumor activity of brentuximab vedotin in relapsed/refractory CD30 positive NHL, including B-cell neoplasms. CD30 expression is determined by immunohistochemistry per local laboratory. Sixty two B-cell lymphoma patients with variable CD30 expression by central review were enrolled in the study. Diagnosis included DLBCL (n=44), and other B-cell neoplasms (n=18) [grey zone lymphoma=6, PMBL=6, follicular lymphoma=3, posttransplant lymphoproliferative disorder=3]. Of the 43 efficacy evaluable DLBCL patients, 40% achieved an objective response ( seven complete remissions, ten partial remissions). The CD30 expression levels for patients with a CR or PR were variable and ranged from <1 to 90%. The study showed that there was no statistical correlation between CD30 expression and response rate [42].
It appears from the current results, that CD30 expression plays a questionable role in deciding the efficacy of brentuximab vedotin in DLBCL. However, this still remains a gray area as it is difficult to explain why there is no correlation between CD30 expression and efficacy of brentuximab vedotin which targets CD30 positive cells. At this point of time, we could only raise hypothesis:
(I) It could be that only a small proportion of CD30 positive cells are required for MMAE release, hence, irrespective of the percentage of cells that are CD30 positive, brentuximab vedotin may still be able to exert its antitumor efficacy.
(II) It could be that brentuximab vedotin, though is anti-CD30 specific, may also be acting on other cellular receptors, such that even if there is negligible CD30 expression on some of the cells, brentuximab vedotin could be effective in killing the cells.
(III) There may be different phenotypes of CD30 receptors, and brentuximab vedotin may be effective only against a particular type, hence, even though cells have high expression of CD30 and a higher killing effect of brentuximab vedotin may be expected, this may not always be true.
(IV) There are different methods available to test for CD30 levels and different values of CD30 expression levels could be obtained by different methods.
More prospective studies need to be done in the future to assess the use of this antibody-drug conjugate in other malignancies and evaluate if CD30 expression plays a role in improving efficacy to brentuximab vedotin.
Brentuximab vedotin, an anti-CD30 antibody drug conjugate received FDA approval in 2011 for the treatment of relapsed/refractory Hodgkin lymphoma and anaplastic large cell lymphoma based on 100% CD30 expression. CD30 has restricted expression in normal tissue. Brentuximab vedotin is an ADC of monoclonal antibody conjugated with MMAE, a microtubule inhibitor and hence facilitates selective delivery of potent MMAE to only the CD30 positive cells and hence avoids any off-target side-effects. Currently many trials are ongoing to analyze the efficacy of brentuximab vedotin in different hematological and non-hematological malignancies with variable tissue CD30 expression levels. In this review, we seek to study the trials to study brentuximab vedotin's activity in diffuse large B-cell lymphoma. According to the current trials, there does not seem to be an association between the efficacy of brentuximab vedotin and CD30 expression levels. Prospective trials are required to test the efficacy of brentuximab vedotin in diffuse large B-cell lymphoma and other malignancies and determine if CD30 positivity of tissue samples should be tested before administering brentuximab vedotin.