Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 1
Introduction: While Continuous Positive Airway Pressure (CPAP) is widely used to manage Obstructive Sleep Apnea (OSA), compliance can be problematic in some cases. These patients are often referred for Mandibular Advancement Devices (MADs) but there is less evidence of their efficacy in severe cases. We investigated the use of biomimetic oral appliance therapy (BOAT) to test the hypothesis that severe cases of OSA can be addressed using BOAT.
Materials and Methods: 15 consecutive adults aged >21 yrs with severe OSA that were unable to comply with CPAP according to a medical physician were treated using BOAT with or without primary mandibular advancement by a dentist with advanced training in dental sleep medicine. The mean Apnea-Hypopnea Index (AHI) of the sample was calculated prior to and after BOAT with no appliance in the mouth during the sleep studies. The findings were subjected to statistical analysis, using paired t-tests.
Results: Prior to treatment the mean AHI of the study sample was 45.9 hr-1 ± 10.5. A follow-up sleep study at 9.7 mos. ± 1.9 showed a 64% decrease in AHI to a mean value of 16.5 hr-1 ± 8.8 after BOAT (p<0.01) with no appliance in the mouth during the post-treatment sleep studies. Results for those without primary mandibular advancement were: 46.6 hr-1 ± 12.9 pre-treatment vs. 13.9 hr-1 ± 10.5 after BOAT (p<0.01); and for those treated with initial mandibular advancement: 45.2 hr-1 ± 8 pre-treatment vs. 19.5 hr-1 ± 6 after BOAT (p<0.01).
Conclusions: BOAT may be a useful method of managing severe cases of OSA in adults, and represents an alternative to CPAP and MADs. However, long-term follow up is needed to reach more definitive conclusions on these initial findings.
Keywords: Biomimetic; Oral appliance therapy
Continuous Positive Airway Pressure (CPAP) is the treatment of choice in patients diagnosed with Obstructive Sleep Apnea (OSA). However, it is prone to intolerance, and compliance is typically less than optimal [1]. As an alternative, it was thought that mandibular advancement devices (MADs) would be an effective treatment in patients with mild to moderate OSA who have failed treatment with CPAP therapy. It was also assumed that MADs would not be as effective as CPAP, and that complications would not occur; but occlusal changes with MADs are more common than previously thought [2]. Despite these findings, MADs have become a common treatment for OSA, and their primary use is in patients with mild to moderate OSA. In fact, recent studies indicate that MADs are also effective in controlling OSA in patients with severe OSA [3]. In a study of adults intolerant to CPAP, the respiratory disturbance index (RDI) decreased by about 50% with a MAD in the patients’ mouth during sleep [4]. But, the role of MADs in the treatment of severe OSA is still not well defined.
One study [5] investigated a thermoelastic MAD, and reported an increase in velopharyngeal airway size, as well as a reduction in the RDI, in patients with moderate to severe OSA when the device was worn while asleep at night. In view of these types of findings, the practice parameters of the American Academy of Sleep Medicine recommend MADs for mild to moderate cases of OSA, or for patients with severe OSA who are unable to tolerate or refuse treatment with CPAP [6]. However, other reports suggest that only 50% of the patients will be compliant with MAD therapy after about 3 years of use [7]. Therefore, we tested the hypothesis that severe cases of OSA can be addressed using biomimetic oral appliance therapy (BOAT; DNA appliance® system), which might mitigate long-term use and side effects of MADs, as no previous using this technique have been reported in the literature.
After obtaining informed consent, we included 15 consecutive adults that had been diagnosed with severe OSA following an overnight sleep study, but were unable to comply with CPAP according to a medical physician. The rights of the subjects were protected by following the Declaration of Helsinki. Inclusion criteria were: subjects aged >21 yrs. diagnosed with severe OSA following an overnight sleep study that had been interpreted by a physician; documented failure/ intolerance to CPAP therapy; good oral appliance compliance; no history of hospitalization for craniofacial trauma or surgery; no congenital craniofacial anomalies, and dentate upper and lower arches. The exclusion criteria included: age <21 yrs.; lack of oral appliance compliance; active periodontal disease; tooth loss during treatment; poor oral hygiene, and systemic bisphosphonate therapy. The study protocol (#121310) was reviewed and approved by the institution’s review board.
Following a confirmed diagnosis of severe OSA by a medical physician, careful history-taking and craniofacial examination was undertaken for each subject by a dentist with advanced training in dental sleep medicine, and each subject was treated using BOAT. BOAT differs from the conventional MADs as it aims to remodel the upper airway through combined maxillo-mandibular correction with or without primary mandibular repositioning. Therefore, a bite registration was obtained in the upright-sitting position with the jaw posture corrected in the antero-posterior and vertical axes specific for each subject, using a sibilant phoneme registration protocol or ‘phonetic bite’ [8]. Upper and lower polyvinylsiloxane impressions were also obtained. The upper model was then mounted on an articulator and the lower model was mounted relative to the upper model, using the bite registration captured. Blinded to two investigators (SC and GDS), a biomimetic oral appliance without primary mandibular repositioning (Daytime-Nighttime Appliance: DNA appliance®; Figure 1) was prescribed for half of the study population (8 subjects).
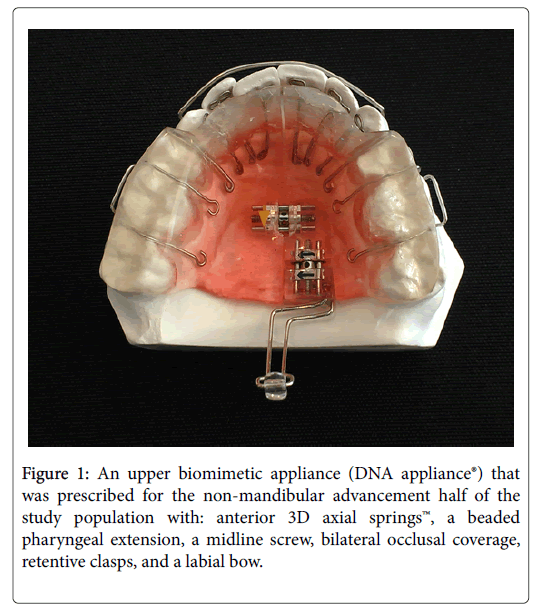
Figure 1: An upper biomimetic appliance (DNA appliance®) that was prescribed for the non-mandibular advancement half of the study population with: anterior 3D axial springs™, a beaded pharyngeal extension, a midline screw, bilateral occlusal coverage, retentive clasps, and a labial bow.
Blinded to two investigators (TG and GDS), a biomimetic oral appliance with mandibular repositioning (mandibular Repositioning Nighttime Appliance: mRNA appliance®; Figure 2) was prescribed for the other half of the sample (7 subjects). Therefore, all authors were blinded in terms of appliance allocation. BOAT is designed to address upper airway deficiencies and to correct maxillo-mandibular hypoplasia in both children and adults [9-17]. All biomimetic oral appliances used in this study had: 6 anterior 3-D axial springs™, a beaded pharyngeal extension, a midline screw, bilateral occlusal coverage, retentive clasps, and a labial bow (Figure 1), but only half of the biomimetic appliances incorporated a mandibular repositioning nighttime component (Figure 2).
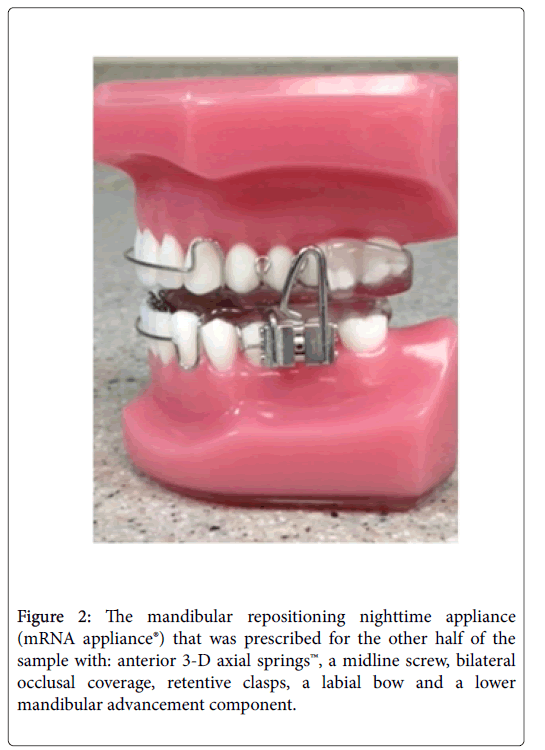
Figure 2: The mandibular repositioning nighttime appliance (mRNA appliance®) that was prescribed for the other half of the sample with: anterior 3-D axial springs™, a midline screw, bilateral occlusal coverage, retentive clasps, a labial bow and a lower mandibular advancement component.
All subjects were instructed to wear the appliances during the evening and at nighttime (for approx. 12-16 hrs. in total), but not during the day time and not while eating, partly in line with the circadian rhythm of tooth eruption [18], although this only occurs in children. Proffit [19] notes that an appliance needs to be worn for at least 8 hrs. in the mouth to have a clinical effect. Written and verbal instructions were given to all subjects.
BOAT requires professional adjustments approximately every 4 weeks, and all subjects reported for review each month. At each monthly follow-up, examination for the progress of craniofacial correction was recorded. Adjustments to the devices were performed to optimize their efficacy. Only gentle pressures were transmitted to the teeth and surrounding tissues and the functionality of the devices was checked with the subject activating a mild force on biting. The subjects were encouraged to maintain their treatment protocol as outlined at the beginning of treatment. Development of the lower arch was implemented using a separate lower appliance (Figure 3) to permit arch re-coordination. A lower appliance (Figure 3) was implemented between 1 to 3 months after the upper appliance unless the subject was wearing the biomimetic appliance design that incorporated the mandibular repositioning nighttime component at the outset (Figure 2). Every 3 months, the overnight sleep studies were repeated. The post-treatment sleep tests were done with no appliance in the mouth and were interpreted by a medical physician. The mean apneahypopnea index (AHI) of the study sample was calculated prior to and after BOAT, and the findings were subjected to statistical analysis, using paired t-tests.
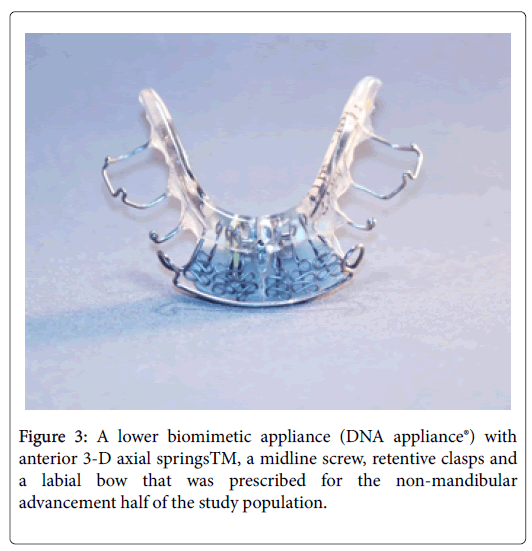
Figure 3: A lower biomimetic appliance (DNA appliance®) with anterior 3-D axial springsTM, a midline screw, retentive clasps and a labial bow that was prescribed for the non-mandibular advancement half of the study population.
Of the total of 15 adults in this study (Table 1), 8 were treated without primary mandibular advancement (Table 1) and 7 were treated with initial mandibular advancement (Table 1). Prior to treatment the mean AHI of the total study subjects was 45.9 hr-1 ± 10.5 with no appliance in the mouth when the sleep studies were done. A follow-up sleep study was done at a mean time interval of 9.7 mos. ± 1.9. At this time, the AHI decreased to a mean value of 16.5 hr-1 ± 8.8 (p<0.001) after BOAT with nothing in the mouth when the posttreatment sleep studies were done. This finding represents a fall in the mean AHI by 64% for the total study sample.
| Total Sample | Non-mandibular advancement | Primary mandibular advancement | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre AHI | Post AHI | Mths | Age | Pre AHI | Post AHI | Pre AHI | Post AHI | |
| Mean | 45.9 | 16.5 | 9.7 | 60.2 | 46.6 | 13.8 | 45.2 | 19.5 |
| Std | 10.5 | 8.8 | 1.9 | 5.6 | 12.9 | 10.5 | 7.9 | 5.9 |
Table 1: Summary of findings of subjects treated with BOAT with or without primary mandibular advancement. AHI: Apnea-Hypopnea Index,Std: Standard deviation.
For the subjects treated without primary mandibular advancement, there were 8 adults in this part of the study (Table 1). Prior to treatment the mean AHI of the subjects without primary mandibular advancement was 46.6 hr-1 ± 12.9. The final sleep study was done at a mean time interval of 10.4 mos. ± 2.6. At this time, the AHI decreased significantly (p<0.001) to a mean value of 13.9 hr-1 ± 10.5, which represents a fall in the mean AHI by 70% for this sample. Indeed, three subjects had an AHI of between 3 hr-1 to 5 hr-1 with no appliance in the mouth when the post-treatment sleep studies were done.
For the subjects treated with primary mandibular advancement, there were 7 adults in this part of the study (Table 1). There was no statistical difference in the initial AHI between this group and those without primary mandibular advancement. Prior to treatment the mean AHI of these study subjects was 45.2 hr-1 ± 8. The final sleep study for this group was done after approximately 9 mos. At this time, the AHI decreased significantly (p<0.001) to a mean value of 19.5 hr-1 ± 6 after BOAT, which represents a fall in the mean AHI of 57% for this study sample. Therefore, it appears that the upper airway can be improved in adults with severe OSA by targeting craniofacial correction with or without primary mandibular advancement using BOAT.
Although , long-term follow up using a larger sample size is needed to make more definitive conclusions on these initial findings, according to Guilleminault and Stoohs [20] there is a distinct interaction between craniofacial morphology and the upper airway, at least in pediatric patients. This present study suggests that combined maxillo-mandibular, biomimetic oral appliance therapy (BOAT) with or without primary mandibular advancement may be a useful method of managing severe cases of OSA in adults, and may represent a viable alternative to CPAP and MAD therapy. Lettieri et al. [21] compared the efficacy of adjustable and fixed MADs for the treatment of OSA. About 37% of their sample had severe OSA (AHI ≥ 30) while sleeping with the device. With adjustable MADs the AHI was reduced to <5 hr-1 in about 57% cases compared to 47% with non-adjustable appliances. For both devices, success was more common in patients with less than severe OSA. Therefore, the severity of AHI should be considered when selecting the type of MAD. But in our present study, no differences in outcome were found when comparing a biomimetic appliance with or without primary mandibular advancement. Presumably, BOAT permits correction of craniofacial components that might not be addressed with MADs alone. In that respect, it would be interesting to analyze the results of the sleep studies performed at 3 months and 6 months, in order to estimate the progress of their improvement, but not all patients were available for this detailed assessment. However, further studies to replicate these current findings, including patients with different disease severity, allowing stratification that might be correlated with the two treatment protocols, are being planned for the future.
Anandam et al. [22] evaluated long-term cardiovascular mortality in patients with severe OSA treated with either CPAP or MAD therapy. They reported that the residual AHI for MAD-treated patients was higher than a CPAP-treated group, but concluded that both CPAP and MAD may be effective therapies to reduce the risk of cardiovascular fatalities in patients with severe OSA. Although CPAP is regarded as the first option for patients with severe OSA, one study [23] investigated whether patients with severe OSA could use a MAD as an alternative treatment to CPAP. In that study, the AHI decreased with MAD use from 30.7 hr-1 to 13.2 hr-1, and they concluded that MADs completely reduce sleep disordered breathing in selected patients with severe OSA. Note that for the subjects treated without primary mandibular advancement in our present study, the mean AHI decreased from 46.6 hr-1 to a 13.9 hr-1 (p<0.001), with no appliance in the mouth for this sample. Similarly, for the subjects treated with primary mandibular advancement in our study the mean AHI decreased from 45.2 hr-1 to 19.5 hr-1 (p<0.001) with no appliance in the mouth. Therefore, BOAT appears to correct sleep disordered breathing in subjects with severe OSA possibly using a different corrective mechanism than MADs, such as craniofacial correction and non-surgical, upper airway remodeling or “Pneumopedics”. This pneumopedic notion is supported by preliminary work that indicates midfacial bone volume [12] and nasal cavity volume [9] increases in adults undergoing BOAT, as well as morphologic changes in the upper airway [10,13,17], which we refer to as upper airway remodeling or pneumopedics. Pneumopedics may be regarded as an epigenetic phenomenon in the sense that morphologic changes are elicited in craniofacial locations remote from the site(s) of genetic change [24], as predicted by the spatial matrix hypothesis [25].
Phillips et al. [26] compared health outcomes after 1 month of CPAP and MAD therapy in patients with moderate-severe OSA. They reported that while CPAP was more efficacious than MADs in reducing the AHI, compliance was higher with MADs. Surprisingly perhaps, neither treatment improved blood pressure, in contrast to sleepiness and quality of life for both treatments. It was therefore concluded that the similar effectiveness for both treatment modalities may be explained by the greater efficacy of CPAP being balanced by better compliance with MADs. Similarly, Lam et al. [27] assessed the efficacy of MADs in patients with severe OSA and hypertension at 3 months and 1 year intervals. It was found that MADs reduced systolic blood pressure in subjects with hypertension and OSA. In those subjects with retrognathia, MADs reduced the AHI from 47.5 hr-1 to 13.1 after 1 year. These AHI results are similar to those noted in our present study; however, although we did not assess blood pressure or hypertension in this present study, our post-treatment sleep studies were performed with no appliance in the mouth while sleeping. Nevertheless, these differences provide further premises for future studies using BOAT. In addition, Tegelberg et al. [28] evaluated the effects of MAD treatment on cognitive functions in patients with moderate-to-severe OSA. After 6 months of MAD treatment, cognitive functioning improved and the AHI decreased with 54% of the patients showing normal breathing during sleep while wearing the MAD. Nevertheless, both treatment modalities presumably represent life-long use if the health outcomes noted above are to be maintained. While we did investigate cognitive function in this current study, BOAT may provide a novel protocol of managing severe cases of OSA and its clinical sequelae in adults, and thus represent an alternative to CPAP and MADs.
We would like to thank Vicky Autry CDT, ArtWires, LLC, Florida, USA, for fabricating the appliances used in this study.