Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Case Report - (2014) Volume 2, Issue 1
An atypical femoral fracture may be one of the devastating side effects of bisphosphonate. We present a patient who obliged to multiple surgeries for atypical femoral fracture of the femur after bisphosphonate therapy. A 63-yearold woman had been on anti-estrogen therapy for skeletal metastasis of the breast cancer. She received 90 mg of pamidronate disodium for 2 years and 4 mg of zoledronic acid for 4 years. Four month after she developed spontaneous left thigh pain, she fell from a standing height. X-ray films showed a subtrochanteric fracture of the left femur. The patient underwent surgery with an intramedullary nail, and radiation therapy was delivered to the fracture site because the possibility of a pathological fracture was unable to be excluded. Radiographs showed some evidence of callus formation, but the fracture line persisted. Two years later, the intramedullary nail broke at a screw hole in radiographs. Bipolar hip arthroplasty was performed and bone chips were grafted at the fracture site. Ten weeks after the operation, callus formation was satisfactory and she was able to walk without pain. One year after the first operation on the left femur, she complained of spontaneous pain in the right thigh and radiographs showed a lateral cortical beak sign with no evident fracture line. The patient underwent intramedullary nailing to prevent subsequent fracture. The radiological fracture sign were improved one year after the operation. The prophylactic intramedullary nailing is effective for the patients with lateral cortical thickening and/or a medial spike on X-ray.
<Keywords: A Typical Femoral Fracture (AFF); Breast cancer; Bisphosphonate; Zoledronic acid; Operation; Prophylactic intramedullary nailing; Bipolar hip arthroplasty
Zoledronic acid is a potent bisphosphonate (BP) that has been used to reduce skeletal-related events in breast cancer patients with bone metastasis [1]. Side effects associated with BP therapy include oesophagitis, renal dysfunction, osteonecrosis of the jaw, and infusionrelated reactions [2,3]. Recently, some reviews have raised concern that prolonged BP therapy may also be associated with atypical femoral fractures (AFFs). The radiographic features of AFFs include a transverse fracture line at the point of origin in the lateral cortex and a prominent medial “spike”, cortical “beaking” or “flaring” adjacent to a discrete transverse lucent fracture line, or focal thickening of the lateral cortex [4]. We report a case of bilateral AFFs in a patient with metastatic breast cancer who had been given high-dose treatment with zoledronic acid.
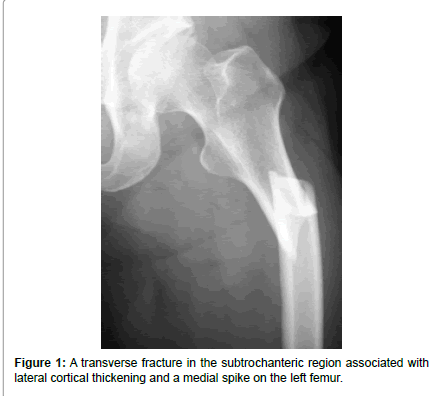
Figure 1:A transverse fracture in the subtrochanteric region associated with lateral cortical thickening and a medial spike on the left femur.
A 63-year-old Asian woman had received a diagnosis of breast cancer with skeletal metastasis in 2004 and had been on anti-estrogen therapy since then. She was advised to commence BP therapy to prevent skeletal complications, and received 90 mg of pamidronate disodium intravenously once a month for two years. The cumulative dose of pamidronate disodium was 1980 mg. In 2006, she was switched to treatment with 4 mg of zoledronic acid intravenously once a month. The cumulative dose of zoledronic acid was 208 mg. After 6 years of BP therapy, she developed spontaneous left thigh pain. Four month later, she fell from a standing height. An X-ray film of the left femur (Figure 1) showed a transverse fracture in the subtrochanteric region associated with lateral cortical thickening and a medial spike. The patient underwent insertion of an intramedullary nail (9.3 mm in diameter) into the left femur (Figures 2a). At 16 days after the operation, radiation therapy (30 Gy) was delivered to the fracture site because the possibility of a pathological fracture was unable to be excluded. Serial radiographs showed some evidence of callus formation, but the fracture line persisted after 2 years. She then developed severe pain at the left midthigh and radiographs showed that the intramedullary nail had broken at a screw hole (Figure 2b). Bipolar hip arthroplasty was subsequently performed with a modular long nail and two cables (Figure 2c). Bone chips from the femoral head were grafted at the refreshed fracture site. Treatment with zoledronic acid has been continued for bone metastasis in spite of delayed union of the fracture site. Aftter bipolar hip arthroplasty, administration of zoledronic acid was stopped focusing on fracture union. At 10 weeks after the operation, callus formation was satisfactory and she was able to walk without pain. One year after the first operation on the left femur, she complained of spontaneous deep pain in the right thigh. Radiographs showed a lateral cortical beak sign with no evident fracture line (Figures 3a and b). The blood test the patient requested treatment of her right femur before a fracture occurred. Therefore, she underwent intramedullary nailing of the right femur (Figure 3c). Although a transverse lucent fracture line became visible at the site of the lateral cortical beak sign about four weeks after the operation (Figure 3d), the patient did not develop pain and complete fracture did not occur. At 10 weeks after the operation on the left femur, the beak sign and fracture line were both improved (Figure 3e). Bone metabolism markers were within normal limits when they were measured 2 weeks before bipolar hip arthroplasty [serum tartrateresistant acid phosphatase-5b (TRAcP-5b), 487 mU/dL ; serum bone alkaline phosphatase (BAP), 16.2 U/L].
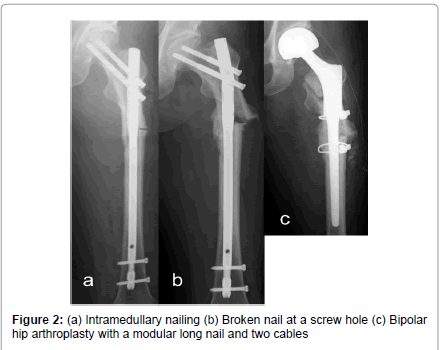
Figure 2:(a) Intramedullary nailing (b) Broken nail at a screw hole (c) Bipolar hip arthroplasty with a modular long nail and two cables.
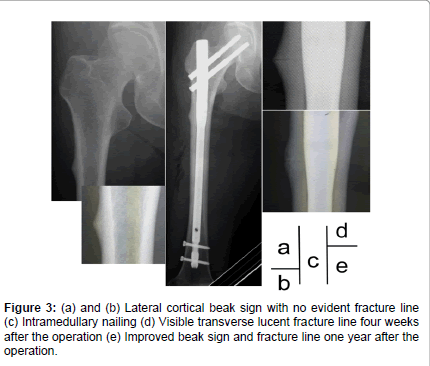
Figure 3:(a) and (b) Lateral cortical beak sign with no evident fracture line (c) Intramedullary nailing (d) Visible transverse lucent fracture line four weeks after the operation (e) Improved beak sign and fracture line one year after the operation.
Multiple case series and reports have documented atypical lowenergy or spontaneous non-spinal fractures in patients receiving BP therapy for osteoporosis [5-8]. These studies have identified subtrochanteric femoral fractures, which have usually been found in patients with osteoporosis. There have been several reports about AFFs in breast cancer patients with bone metastasis who were on zoledronic acid therapy [9-13]. Puhaindran et al. reported that all of their patients who developed AFFs had prodromal ipsilateral thigh pain for at least two months, and suggested that it was useful to ask patients receiving long-term intravenous BP therapy about such symptoms [13]. Physicians who manage patients with skeletal metastases should be aware of the emerging association between BP therapy and AFFs, wince heightened awareness will lead to early detection of incomplete fractures. In the report of the task force on AFFs, Shane et al. stated that healing of complete fractures was not assessed in 198 of 310 reported cases, but healing was delayed in 26% of the other 112 cases [14]. Therefore, if there is no symptomatic and radiographic improvement of an incomplete fracture after conservative therapy, prophylactic intramedullary nailing should be strongly considered because these patients may progress to complete fracture. In our patient, the right femur underwent intramedullary nailing before complete fracture occurred and the fracture line was first detected at four weeks after the operation. Therefore, there seems to be little possibility that an incomplete fracture will heal with observation alone. In this case, the AFF on the left side was misdiagnosed and treated with radiation therapy. AFFs should be differentiated from bone metastatic lesion on the basis of characteristic radiological findings before the treatment because radiation therapy would not have inhibited bone remodeling. Moreover teriparatide therapy that could accelerate healing of the fracture is contraindicated for a patient who received radiation therapy to the bone metastasis.