Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2015) Volume 3, Issue 3
Objective: To determine the efficacy of osteogenic loading (OL) specific therapy for bone mass density (BMD) and musculoskeletal bone performance adaptations in both osteopenic and osteoporotic postmenopausal female subjects.
Research design and methods: We randomly assigned from a single site patient pool 55 postmenopausal patients to receive OL therapy consisting of axial bone loading through lower extremity and spinal erection kinetic chains. The subjects selected (mean age of 69 (+/-? 8.3 SD) years) were seen to have low BMD (T-Score of -1.0 or lower) or were diagnosed with osteoporosis, but had not yet started any or had declined pharmacological intervention. All subjects performed in a 24-week observational trial. The OL apparatus utilized isolates optimal ranges of motion (i.e. ranges that humans reflexively assume to absorb impact in a fall) and had been previously seen to increase BMD and functional loading in impact positions. The subjects were able to produce force/loading to fatigue in the respective movements from baseline to post. We measured multiples-of-bodyweight (MOB) baselinepost, and randomly assigned a subgroup for baseline-post DXA scans.
Results: The OL therapy intervention resulted in statistically significant increases in functional loading of bone based on self-imposed loading to fatigue of 3.2 (+/-1.0 SD) MOB to 7.2 (+/-2.0 SD) MOB in hip/lower extremity loading and 0.98 (+/-0.32 SD) MOB to 1.97 (+/-0.57 SD) MOB in the loading of the spine. A 131% and 126% increase was recorded in musculoskeletal functional kinetic chain ability respectively. The DXA subgroup saw BMD (g/cm2) increases of 14.9% (+/- 11.5% SD) in the hip, and 16.6% (+/- 12.2% SD) in the spine (p <0.01 in both baseline-post dependant data sets).
Conclusions: OL therapy as an adjunct to standard care, or as a preventative approach is both feasible and effective for improving BMD for ambulatory individuals with below -1 T-scores. Further, the metrics of MOB force/ loading levels can be viewed as measures of functional bone performance (FBP); meaning that a metric showing tolerable levels of force an individual can absorb into bone/kinetic chain relevant to protection against fracture during the deceleration of a fall impact.
<Keywords: Osteoporosis; Hip fracture; Bone; Exercise; Physiotherapy
According to the International Osteoporosis Foundation (IOF), 1 in 3 women over age 50 will experience osteoporotic fractures, as will 1 in 5 men over the age of 50 [1]. Hip fractures cause the most morbidity with reported mortality rates up to 20-24% in the first year after a hip fracture [2]. The loss of function and independence among survivors of hip fracture is profound, with 40% unable to walk independently and 60% requiring assistance a year later [3]. Physical medicine interventions independent of pharmaceuticals (e.g. exercise and physiotherapy) have not seen success with bone mass loss treatment.
Exercise and physiotherapy have consistently been shown to improve BMD, but not at significant enough levels where lifestyle changes and exercise could be seen to reduce fracture risk alone [4]. A 2007-2010 National Health and Nutritional Examination Survey (NHANES) analysis which utilized a broad scope of exercise activity and bone health, showed that no significant differences were seen in the bone health and fracture rates between exercisers and nonexercisers [5]. Congruent with this evidence, the International Osteoporosis Foundation (IOF), as well as the National Institute for Health and Care Excellence (NICE) recommends that individuals with low BMD engage in exercise, but only as a supplement to the standard of medical care.
Avoidance of fracture is the primary goal in treating low BMD or osteoporosis, but the standard of care in treating low BMD has historically related solely to pharmacological solutions. These solutions focus only on the bone itself and not on the tissues which absorb and decelerate force/loading in a fall. A methodology of observing how a bone performs under self-created compressive force could potentially be an indicator of bone quality or a metric of function under stress. This is what we mean by the term, FBP. Further, by adaptively increasing an individual’s ability to absorb force/loading, that individual can then potentially decrease their overall chances of fracture [6].
Our aim was twofold:
• 1. To report baseline force/loading FBP levels, seen in the OL therapy environment, and the rate of change in progressive loading from baseline-post 24-week intervention.
• 2. To determine potential correlation between FBP adaptation and BMD adaptation.
Design:
We conducted a 24-week, single-center, randomized, observational trial with an osteopenic and osteoporotic population. Those who were osteoporotic had either not yet begun any pharmaceutical intervention, had discontinued it at least 6 or months earlier due to complications, or had refused it entirely. A single group of 70 postmenopausal female subjects were selected at random by their GP and referred to the OL therapy study (of which, 55 completed the study). For budgetary provision, a DXA scan subgroup was randomly selected with 11 subjects in order to measure potential causal effects of FBP adaptations to BMD. Subjects were to complete the once per week therapy intervention with a minimum of 18 sessions completed at the conclusion of the 24 weeks without dietary or activity modification. The Senior Medical Partner of the Stratford Village Surgery (SVS), First 4 Health Group (part of the United Kingdom National Health Services (NHS)), Chief SVS Clinical Director, and the independent review board (IRB) of the First 4 Health Group approved the study.
It is important to highlight some of the differences between the OL modality and conventional resistance exercise protocols. The highlevels of force/loading used with this modality would be unachievable with conventional means [7]. The therapy protocol with this apparatus is more infrequent and shorter in duration per session than any exercise recommendation the IOF is currently making for conventional resistance exercise. Recently, OL use with osteoporosis patients has shown greater compliance than with most physical medicine or exercise recommendations [8,9].
Setting:
The OL therapy intervention took place at a single NHS facility, SVS, located in the London Borough of Newham, England. Registered Health Psychologist at the SVS supervised the intervention. The NHS technical staff at SVS aided in the clerical aspects of the intervention.
Participants:
Subjects between the ages of 55 and 87 (with one 48 year old female who had been referred because of low BMD and early onset menopause), were referred at random to participate in this study by their GP. Primary identification of potential subjects consisted of a Tscore -1.0 or lower. One out of every 3 patients who met the inclusion criteria was asked if they wanted to participate in this study during their regular GP clinic appointments. Patient invitations were continually given until the study population was full (70 invited), and patients were seen in no particular order, therefore subject selection was random. Patients were brought to an initial orientation lecture where they were given IRB consent forms, modality consent forms, NHS exercise referral screening forms, and educated on the OL modality. The modality consent had subjects to agree to the following statement; “I give my permission to allow my de-identified data for product improvement, quality-control, and research purposes.” This language is consistent with Stanford University’s IRB de-identified data use permissions [10]. Study completion sample developed as follows:
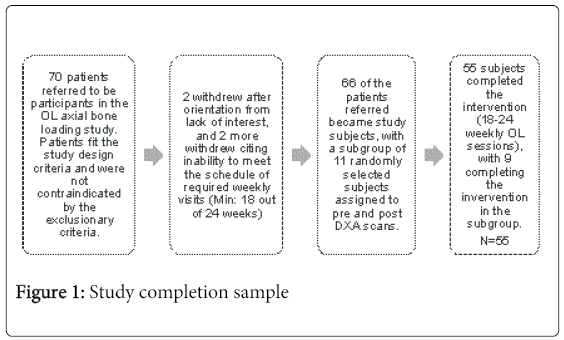
Figure 1: Study completion sample
The mean age of participants who completed the study (N=55) was 68.9 (+/-8.4 SD). Randomized subgroup (N=9) aged 63.9 (+/-11.3 SD), had baseline-T-scores in the hip of -1.23 (+/-1.54 SD) and spine of -2.17 (+/-1.55 SD). Subjects who were diagnosed with osteoporosis were 28 of the total 55, the rest being osteopenic, and this included 6 of the 9 subgroup subjects.
Patients who met the study design were excluded if: 1) limitations or contraindications to ambulatory and/or resistance training exercise are present (assessed via the required NHS exercise referral screening form); 2) acute illness or injury is present; 3) exercise or physical activity restrictions have been imposed by their health care provider; 4) there is a history of or current problems with syncope (loss of consciousness or fainting); 5) elevated blood pressure is present (≥140 mmHg systolic or ≥ 90 mmHg diastolic) when measured at their baseline testing session and is not actively being controlled by medication while under the supervision of a licensed health care provider; 6) the participant has experienced a stroke (hemorrhagic or thrombotic) within the past 12-months; 7) the participant has been treated for or has a history of an aneurysm (ballooning of a blood vessel); 8) the participant is engaging in exercise or exercise type activity 2 or more times weekly for 20 minutes or longer per session or in any resistance training during the previous 6 months. Subjects would also be excluded from the final analysis if they attended less than the required 18 of the 24 weekly sessions.
Randomization and Blinding:
After patients were referred at random by their GP, they attended the orientation session lecture given by the principal investigator and were informed further about the study. They were then screened for the aforementioned exclusion criteria to become a subject. As there was no control group and this was an observational study, the subjects could not be blinded. However, the DXA scans were conducted by NHS laboratory staff unaffiliated with the study, none of whom knew which of the patients in the clinic were subjects in the study. Therefore, the DXA analysis portion was blinded. The DXA analysis was performed by SVS DXA radiology technicians.
Intervention:
The subjects were asked to return to the SVS one time per week at a regularly scheduled interval to complete one OL session. There was no variation in duration or intensity of the OL protocol from the baseline session to subsequent sessions. Subjects were told to engage to their perceived maximum force/loading level while not reaching a point of discomfort. The protocol included: one compressive movement with upper extremities; one movement with lower extremities; one movement with core activation; and one movement with spinal compressive forces recruited, for a total of 4 movements with a total exercise time of 15 minutes. Though the 4 movements each last only 5 seconds in duration, the device adjustments are specific (to the mm), and take the full 15 minutes to identify the correct optimal axialcompressive positions. The protocol was designed with emphasis being placed on maximum muscular recruitment in positions of optimal leverage and biomechanics, resulting in the greatest selfcontrolled axial loading of bone [7-9,11,12 ]. In the movements, compression of the entire kinetic chain is measured at approximately 5cm of compression between axial bone compression as well as joint capsule compression [7]. The OL modality is unique to the force/ loading of individuals in the same way impact would be absorbed in a fall; an individual would have the time to reflexively react and absorb impact. The force/loading, FBP levels were tracked in each movement and for each session via Internet server tracking software to ensure no loss of data. Subjects were instructed not to change their eating habits during the intervention.
Outcomes and Measurements:
The primary outcome measures were FBP (from baseline to post), as collected from the OL device based on loading in the respective movement compared with bodyweight. Only 2 of the 4 OL movements were analyzed in the FBP data, the hip loading and spine loading events, which correspond to the hip and spine areas that are scanned in DXA analysis and are the basis for diagnosis of low BMD or osteoporosis. Secondary outcomes reported were changes or lack of changes in the subgroup BMD levels.
NHS lab technicians recorded both baseline and post-DXA scans of all subjects who were blended into their regular patient load, thereby blinding technicians to which individuals were subjects in this study. Baseline DXA scans were performed no more than 7 days before the initial baseline OL session. Post DXA scans were performed 60 days after the protocol completion due to the availability of the DXA table that was used for the baseline scans. Programme supervisor technicians twice measured bodyweight; first at the baseline OL appointment and again at the conclusion of the 24 weeks. DXA scans were done with the Hologic Discovery™, manufactured by Hologic Inc., 35 Crosby Drive, Bedford, MA. United States. All subjects had baseline-post DXA measures performed on the same DXA table with the exception of subject 6, who had the baseline-DXA performed at another location. OL therapy was performed with bioDensity™, manufactured by Performance Health Systems LLC., 401 Huehl Road, Suite 2a, Northbrook, IL. United States.
Each time a subject arrived for their OL session, standard procedure was to inquire if subjects have had any physical problems, issues, pain, discomfort, or other issues since their last OL session. Typically, subjects would call, e-mail, or volunteer this information before their next session without being prompted. However, we include this procedure to help maximize safety for participants by screening for complications, contraindications, or adverse events related or not to their previous OL sessions.
Adverse Events and Compliance:
There were no adverse events during the 24-week intervention. However, 11 of the subjects were not able to adhere to the minimum 18 OL sessions and 2 subjects were not able to return for their post- DXA scan. Six of the 11 subjects who did not meet the minimum number of completed sessions, did so as a result of family travel. Five subjects dropped out of the study without giving reason. All subjects complied with each OL session and achieved momentary fatigue in each of the 4 movements with each session.
Statistical Analysis:
First author collect all data, and tested for delta between baselinepost MOB levels for FBP in both hip and spine force/loading respectively. Corresponding subgroup DXA measures were analyzed baseline-post. Baseline-post measures were analyzed as a T-test of dependent variables. The hypothesis was that there would be a difference between the pre-post measures of dependent variables. A Spearman’s Rho correlation coefficient test (R) was used to determine congruency between the FBP delta in the hip and FBP delta of the spine comparing subset to test group. analyses were performed using SPSS™ version 21 (SPSS Inc., Chicago, IL).
The baseline-post measures showed significantly increased mean MOB loading ability for the total (N=55) and subgroup (N=9) as well as significantly increased BMD with the subgroup in both the hip and spine (p ≤ 0.01). All subjects gained BMD in either the hip, spine or both and no BMD values declined from baseline. Statistically significant congruency was seen in adaptations of FBP between total and subgroup baseline-post (p ≤ 0.05 for the hip and p ≤ 0.05 in the spine). Bodyweight did not significantly change in this intervention.
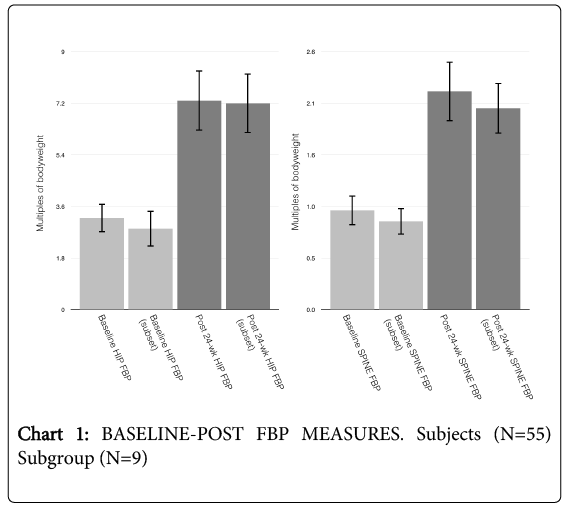
Chart 1: BASELINE-POST FBP MEASURES. Subjects (N=55) Subgroup (N=9)
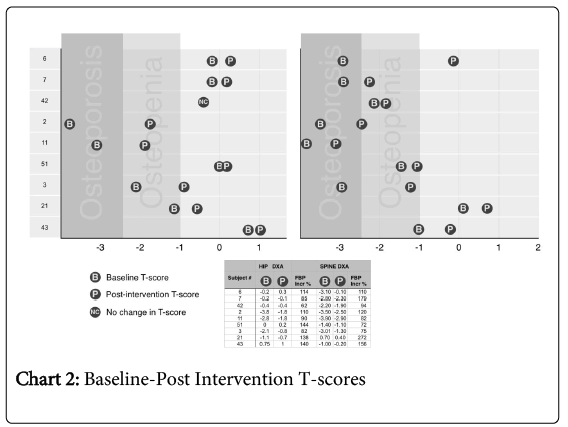
Chart 2: Baseline-Post Intervention T-scores
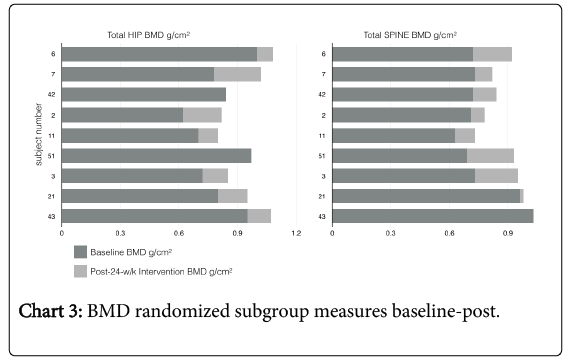
Chart 3: BMD randomized subgroup measures baseline-post.
Hip FBP results: Subjects had no bodyweight change from pre-post OL therapy intervention, therefore MOB calculations were constant to a standing bodyweight. Subjects had mean baseline FBP force/loading events of the lower extremities (LE) of 3.24 (+/-1.02 SD) MOB to a post intervention mean of 7.32 (+/-2.09 SD) MOB. This is a 132% (+/-61.9% SD) increase in FBP of the hip/LE musculoskeletal kinetic chain.
Hip FBP results (subgroup): Subjects had no bodyweight change from pre-post OL therapy intervention, therefore MOB calculations were constant to a standing bodyweight. Subjects had mean baseline FBP force/loading events of the lower extremities (LE) of 3.56 (+/-2.09 SD) MOB to a post intervention mean of 7.0 (+/-2.29 SD) MOB. This is a 176% (+/-88.4% SD) increase in FBP of the hip/LE musculoskeletal kinetic chain.
Hip DXA results: (total hip analysis) Mean T-Score went from -1.23 (+/-1.54 SD) to -0.46 (+/-0.94 SD). BMD (g/cm2) went from a mean of 0.821 (+/-0.132 SD) to 0.933 (+/-0.108 SD). Subjects realized a significant increase (p ≤ 0.01) of 14.89%(+/-11.55% SD) in BMD of the hip during the 24-week OL intervention.
Spine FBP results: Subjects had no bodyweight change from prepost OL therapy intervention, therefore MOB calculations were constant to a standing bodyweight. Subjects had mean baseline FBP force/loading events of the spine of 0.98 (+/-0.32 SD) MOB to a post intervention mean of 2.18 (+/-0.65 SD) MOB. This is a 127% (+/-49.7% SD) increase in FBP of the spine and spinal erector musculoskeletal kinetic chain.
Spine FBP results (subgroup): Subjects had no bodyweight change from pre-post OL therapy intervention, therefore MOB calculations were constant to a standing bodyweight. Subjects had mean baseline FBP force/loading events of the spine of 0.96 (+/-0.35 SD) MOB to a post intervention mean of 1.97 (+/-0.57 SD) MOB. This is a 122% (+/-71.5% SD) increase in FBP of the spine and spinal erector musculoskeletal kinetic chain.
Spine DXA results: (total Spine analysis) Mean T-Score went from -2.17 (+/-1.55 SD) to -1.32 (+/-1.17 SD). BMD (g/cm2) went from a mean of 0.769 (+/-0.131 SD) to 0.887 (+/-0.100 SD). Subjects realized a significant increase (p ≤ 0.01) of 16.64% (+/-12.19% SD) in BMD of the total spine during the 24-week OL intervention.
We saw a statistically significant increase of FBP and BMD in subjects with 24 weeks/sessions of OL intervention. This in itself can indicate a decrease in the potential for fracture based on the BMD change, but the FBP metric bears some specific and useful characteristics previously unseen in bone health diagnostics and therapy. While DXA is the clinical standard method for measuring BMD in the lumbar spine and hip/femur areas, the DXA diagnostic looks to fracture prediction only by analyzing bone [13,14]. Divergence is seen between T-score and age with loss of functional movement contributing to the higher incidence of fracture [15]. As other musculoskeletal characteristics of fracture avoidance are not a component of DXA analysis [16], compounded with bisphosphonate related atypical fracture in patients who show healthy DXA results [17], the need for a comprehensive musculoskeletal metric of bone health for fracture potential diagnosis exists. In the past 5 years more research has been made available focusing on the relationship between musculoskeletal deficiency and the likelihood of fracture [18,19]. This direction in research has afforded therapists to apply restorative biomechanics protocols, in an effort to further engage musculoskeletal kinetic chains for greater function, which can then aid in fracture avoidance [20,21]. In addition to biomechanics and normalized movement patterns, patients using the OL therapy modality can engage the musculoskeletal system at higher levels, which can allow for a greater level of performance in all tissues involved in the OL movements, including: tendons, ligaments, muscle, as well as bone.
Absorbing momentary peak energy within bone is one of the largest fracture causing factors seen in cadaver extracted hip femoral complex [22]. These loads seen with failure of cadaver extracted hip femoral complex are lower in force energy (450 joules) than that of high impact exercise. Further, animal testing has shown that deceleration of impact has enabled test animals to avoid fracture, whereas preexhaustion exposes them to fracture due to the inability to decelerate the peak forces within bone [6,23]. Increases of performance (FBP) in these impact absorption/deceleration ranges of motion provide for discussion in the future of both functional diagnostics corresponding to fracture avoidance as well as physical medicine therapy intervention designed to decrease potential fractures.
There were a number of limitations to this analysis, as there was no double-blinding. Developing a placebo exercise intervention could potentially have an osteogenic effect as well. The general sample and the DXA subgroup was kept small in order to prevent a exceeding budget while still providing an ample number of subjects with which to assay data trends.
OL therapy as an adjunct to standard care, or as a preventative approach, is both feasible and effective in improving BMD for ambulatory individuals with poor bone mass. Further, the metrics of MOB force/loading levels can potentially be viewed as measures of FBP based on the correlation seen between gains in FBP in the test group compared with the DXA subset. We can now have a potential metric showing tolerable levels of force an individual can absorb into their bone/kinetic chain, in order to protect against fracture during the deceleration of a fall impact. More research with a larger sample size is required to determine fracture avoidance predictability with FBP metrics with respect to either diagnostics or therapy.