Journal of Leukemia
Open Access
ISSN: 2329-6917
ISSN: 2329-6917
Case Report - (2018) Volume 6, Issue 2
Keywords: Peripheral blood; Leukemia; Stem cell
The coexistence of AML and CLL has occasionally been reported [1]. Most of these cases occur as a secondary event in patients receiving chemotherapy or radiotherapy [2]. CLL disease is known to be associated with immunoglobulin deficiencies and increases the risk of secondary malignancies [3]. In addition, CLL patients with coexistent solid tumors have been reported to develop MDS and AML. AML developed after CLL treatment is called therapy-related AML. Some AML patients are diagnosed concomitantly with CLL disease. The development of flow cytometry has increased the diagnosis of coexistence [4-8].
In this study we present 3 cases of CLL&AML and CLL&MDS/ AML co-existences without previous exposure to cytotoxic, immunosuppressive drugs or radiation.
Case 1
A 70-year-old male presented to our clinic with complaints of fatigue, pallor and weakness. On physical examination, 5 cm splenomegaly and 2 cm hepatomegaly were noted. Laboratory studies showed hemoglobin (Hb), 10.8 g/dL; white blood cell (WBC), 49 × 109/L; platelet count, (PLT) 58× 109/L. The peripheral blood (PB) smear showed 60% circulating blast cells and 30% lymphocytes, with smudge cells. Bone marrow examination and flow cytometric analyses demonstrated that blasts expressed CD117, HLA-DR, CD13, CD33, MPO and lymphocytes showed a typical CLL immunophenotype which was CD5+CD19, CD20, CD22 positive; and CD200, CD10, CD23, CD25, FMC7 negative (Figure 1, Figure 2A and 2B). Polymerase chain reaction (PCR) assay, CLL cytogenetic studies, AML specific genetic abnormalities panel including t(8;21), t(15;17), inv(16), FLT3-ITD, FLT3D835 NPM1, del(17)(p13.1), del(13)(q14.3), del(11)(q22.3), and centromere 12 were all negative. PCR assays for AML specific genetic abnormalities were negative. Patient classified as intermediate risk group for AML. Concomitant CLL and AML considered as a final diagnosis. Cytarabine and daunorubucin treatment (5+2) was administered. Remission was obtained after treatment. After that, dose adjusted FLAG (fludarabine + high-dose cytarabine + G-CSF) was given since FLAG is effective both AML and CLL clones. The aim was to consolidate AML and to eradicate CLL clones because of the agressive course of the disease. Examination of bone marrow aspiration, biopsy and peripheral blood smear after the second cycle of chemotherapy showed increased blast counts. A Hypometylating agent with low dose cytarabine treatment was planned. During the follow-up period patient developed pneumonia and heart failure. Treatment targeting heart failure and pneumonia was started. The patient responded the therapy, however refused further hypometylating agents and cytarabine therapy and unfortunately died 5 months after the diagnosis.
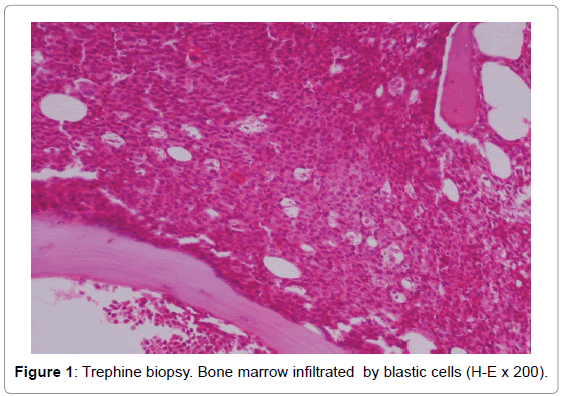
Figure 1: Trephine biopsy. Bone marrow infiltrated by blastic cells (H-E x 200).
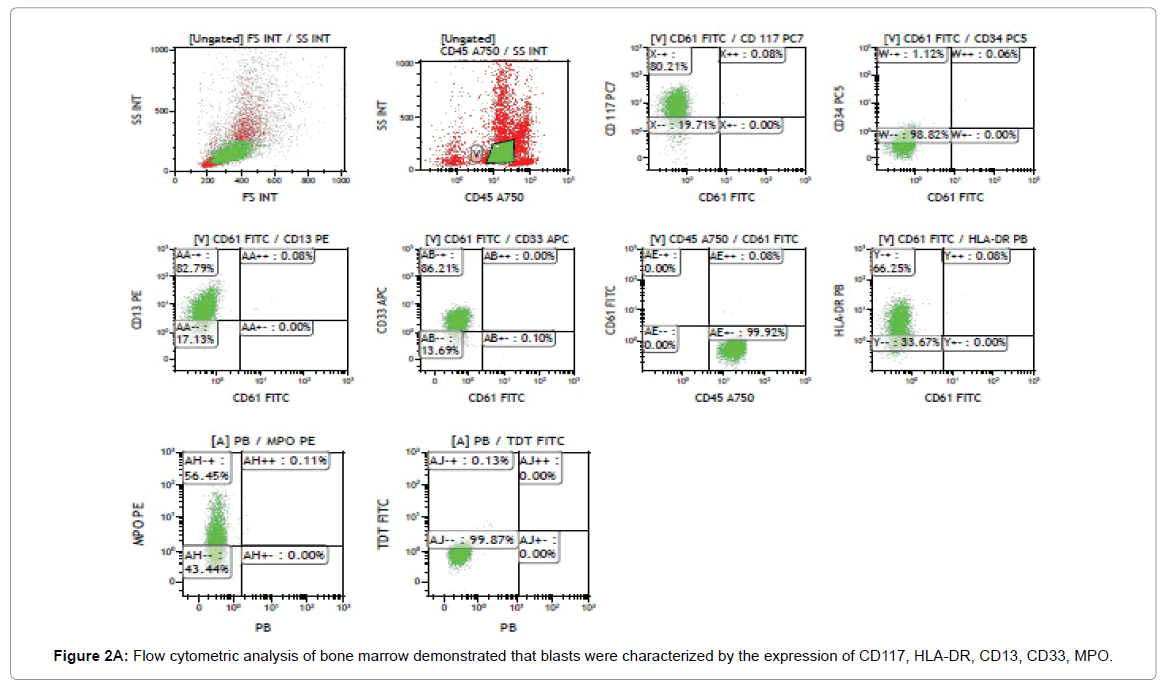
Figure 2A: Flow cytometric analysis of bone marrow demonstrated that blasts were characterized by the expression of CD117, HLA-DR, CD13, CD33, MPO.
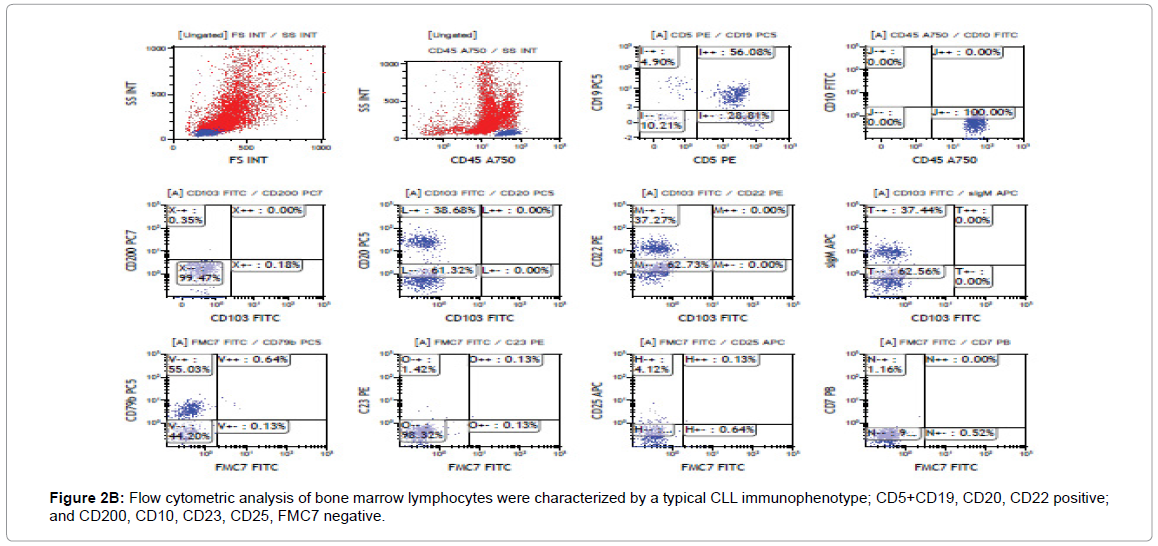
Figure 2B: Flow cytometric analysis of bone marrow lymphocytes were characterized by a typical CLL immunophenotype; CD5+CD19, CD20, CD22 positive; and CD200, CD10, CD23, CD25, FMC7 negative.
Case 2
A-50-year old female presented with weakness and epistaxis. Laboratory studies showed Hb, 10.8 g/dL; WBC, 3.8 × 109/L; PLT, 17 × 109/L. The peripheral blood smear showed lymphocytes with smudge cells, normoblasts, and 35% circulating blasts. Bone marrow aspiration showed 32% blastic cells which expressed CD34, CD33, CD13, CD117, CD45, CD16 and 52% lymphocytes with positive CD45, CD5+CD19, CD20, CD23, CD200 and negative CD10 expression (Figure 3A and 3B, Figure 4A and 4B). Cytogenetic studies were negative for CLL and AML panels. PCR assays for AML specific genetic abnormalities such as t(8;21), t(15;17), inv (16), FLT3-ITD, FLT3D835 and NPM1 del(17) (p13.1), del(13)(q14.3), del(11) (q22.3) were negative. Patient classified as intermediate risk group for AML. Cytarabine and Idarubucin (7+3) treatment was administered. After this treatment, bone marrow aspiration and biopsy showed remission status, and Minimal residual disease (MRD) was negative. A fungal infection and retinal hemorrhage developed during the follow up period. After resolving of infection and retinal hemorrhage, allogeneic stem cell transplantation was performed from an HLA-matched sibling. Grade 1 graft versus host disease developed. On the 100th day chimerism was 99% and there was a CLL clone (20%, CD5+CD19, CD200 positivity). Cyclosporine was stopped at 6th month. The patient was in remission at 23th month of allogeneic hematopoietic stem cell transplant without treatment.
Figure 3: A. Mature apparent lymphocytes, normoblast, and circulating blasts in peripheral blood with Giemsa staining B. Blastic cells (32%) which are expressed CD34, CD33, CD13, CD117 CD45, CD16 and lymphocytes (52%) CD45, CD5, CD19, CD20, CD23, CD200 positivity and negative for CD10 in bone marrow.
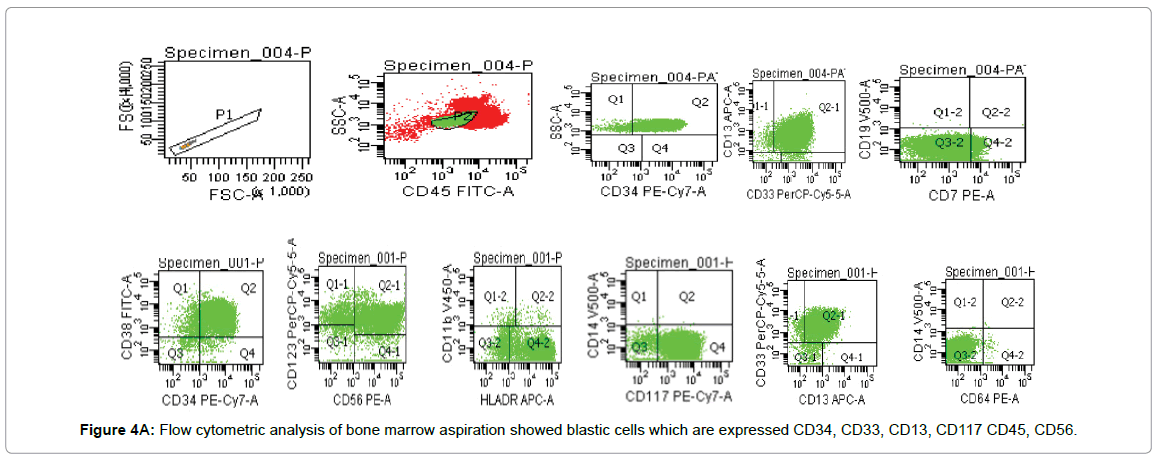
Figure 4A: Flow cytometric analysis of bone marrow aspiration showed blastic cells which are expressed CD34, CD33, CD13, CD117 CD45, CD56.
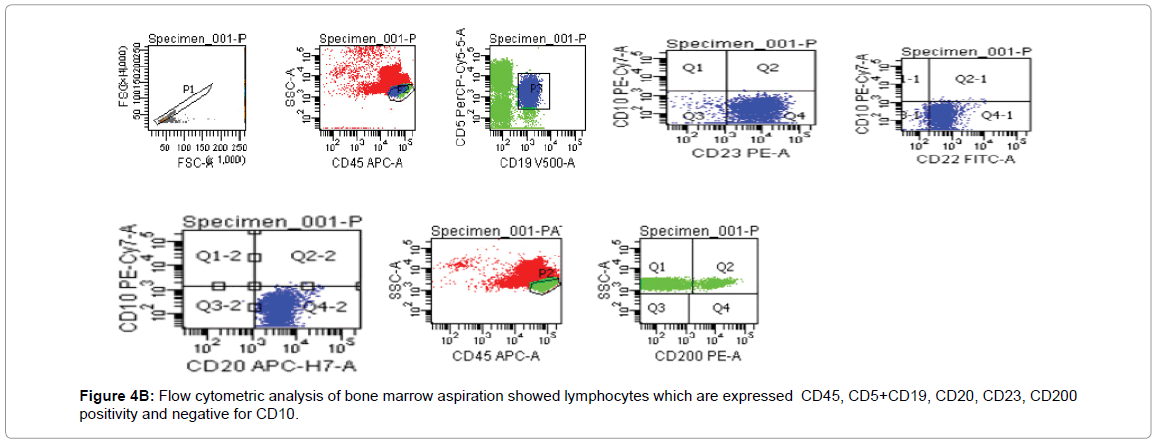
Figure 4B: Flow cytometric analysis of bone marrow aspiration showed lymphocytes which are expressed CD45, CD5+CD19, CD20, CD23, CD200 positivity and negative for CD10.
Case 3
A-55-year-old man was referred to our hospital with complaint of weakness. The laboratory studies showed Hb, 8.2 g/dL; WBC, 2.8 × 109/L; PLT, 17 × 109/L. Serum vitamin B12 and folic acid levels were in normal range. The peripheral blood smear showed neutrophil hypersegmentation and blastic cells. On physical examination 3 cm splenomegaly was found. Bone marrow biopsy showed megaloblastic and dysplastic changes in erythroid, megakaryocytic and myeloid lineages. Besides, neoplastic small lymphocyte cluster in the middle of blastic myeloid area was seen. Percentage of myeloid blasts was 15%. The pathological diagnosis of bone marrow evaluation was a coexistence of AML/KLL diseases (Figure 5A-3C). Flow cytometric analysis revealed HLA-DR, CD13, CD33, GlyA, MPO positivity. Expression rates of CD117 were 15 % and CD34 was 6 %. CD5+CD19, CD20, CD22, CD23 and CD200 were negative (Figure 6A). Diagnosis of MDS with excess blasts was considered. Decitabine treatment was started. After 4 cycles of decitabine, bone marrow aspiration and biopsy were remade. CD34, CD117, MPO were positive and blast cell number was around 30%. Lymphocytic cells activity increased at around 35%. In the concurrent flow cytometry result, the analysis of HLA-DR, CD5+CD19, CD20, CD22 were positive (Figure 6B). PCR assays for AML and CLL specific genetic abnormalities which were t(8;21), t(15;17), inv(16), FLT3-ITD, FLT3D835 NPM1, del(17)(p13.1), del(13)(q14.3), del(11)(q22.3), and centromere 12 were negative. Cytarabine and mitoxantrone (7+3) treatment was started. After cytarabine and mitoxantrone regimen control bone marrow aspiration and biopsy showed partial remission with 12% percent of blasts. FLAG regimen was applied to eradicate CLL clone. After the second FLAG regimen neutropenic fever and pneumonia developed and could not be controlled by antibiotics and supportive treatment. The patient died after 14 months of the diagnosis.
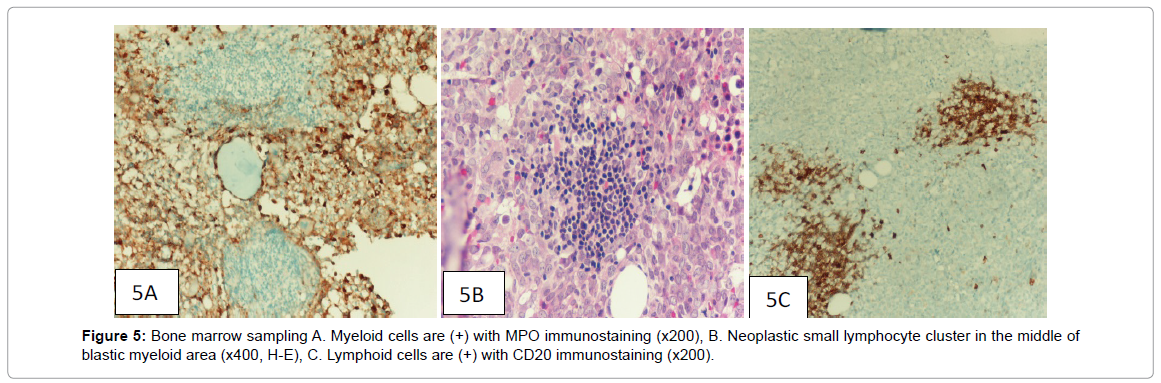
Figure 5: Bone marrow sampling A. Myeloid cells are (+) with MPO immunostaining (x200), B. Neoplastic small lymphocyte cluster in the middle of blastic myeloid area (x400, H-E), C. Lymphoid cells are (+) with CD20 immunostaining (x200).
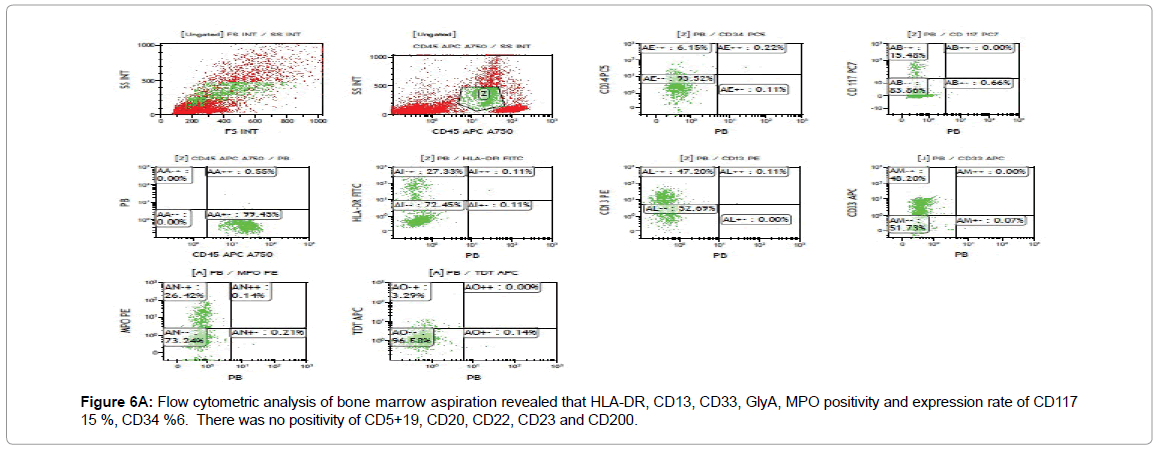
Figure 6A: Flow cytometric analysis of bone marrow aspiration revealed that HLA-DR, CD13, CD33, GlyA, MPO positivity and expression rate of CD117 15 %, CD34 %6. There was no positivity of CD5+19, CD20, CD22, CD23 and CD200.
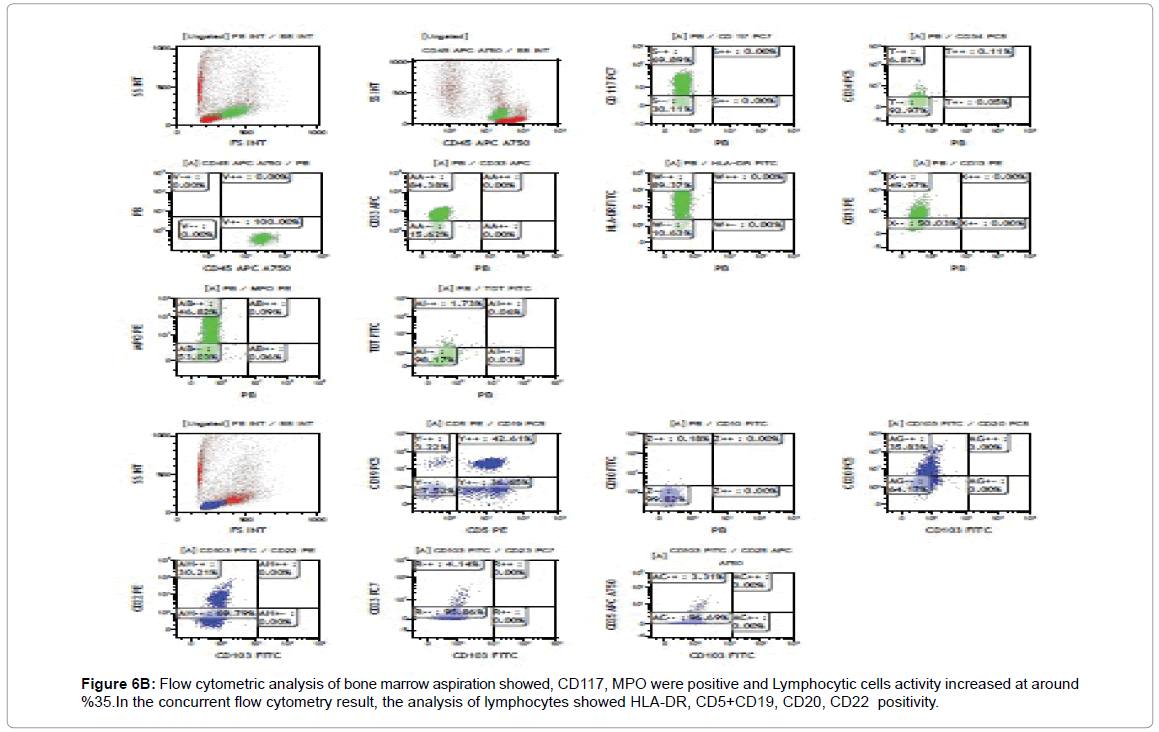
Figure 6B: Flow cytometric analysis of bone marrow aspiration showed, CD117, MPO were positive and Lymphocytic cells activity increased at around %35.In the concurrent flow cytometry result, the analysis of lymphocytes showed HLA-DR, CD5+CD19, CD20, CD22 positivity.
The association of AML and CLL has previously been reported. AML is considered to develop as a secondary leukemia after CLL treatment likewise that after having given alkylating agents particularly chlorambucil, melphelan, nitrosureas and radiotherapy [9]. In the present study history of the patients did not reveal any known leukomogenic drug, radiotherapy and CLL treatment exposure before the diagnosis MDS and AML. Acute myeloblastic leukemia and CLL, which are two different and unrelated malignancies, have occasionally been diagnosed simultaneously in treatment-naive patients. AML is about 10 to 50 times more frequent in CLL patients than in the agematched general population. In one report, eleven patients developed AML during the course of untreated CLL, whereas AML and CLL were diagnosed concomitantly in 16 patients [10]. The concomitant occurrence of AML and CLL might stem from a common stem cell defect, leukomogenic factors or from a genetic predisposition in some patients. We found no cytogenetic abnormalities in our cases; however, Hematopoietic Stem Cells (HSCs) with multiple genetic abnormalities might have caused the development of several myeloid and lymphoid progenitors that consequently turned into leukemic stem cells. Recently it was reported that CLL cells did not originate from differentiated mature lymphocytes but rather from primitive HSC [11]. Aberrant Wnt signaling is observed in both CLL and AML patients and might play a role in transforming pre-leukemic stem cells into the leukemic stem cells [12]. Our cases support the idea that AML and CLL might demonstrate two separate disease processes, which is CLL originates from abnormal CD5+CD19 positive lymphoid clone whereas AML originates from myeloid from CD34, CD117, CD13, CD33, and MPO positive myeloid clone. Lu CM et al. showed that in a patient AML and CLL developed from different clones [13]. We only showed immunophenotypic features of AML and CLL were different. This phenotypic difference does not rule out a possibility that two clones might be related. Kikushige et al. reported that the tendency to generate clonal B cells had already been acquired at the HSC stage in CLL patients [11]. In this setting, HSCs might be considered as the critical cellular target in the oncogenic process. This is an arguable subject that needs to be elucidated.
Most cases have been diagnosed based on morphology and cytochemical evidence. Both methods have questionable limitations. After the development of multi-color flow cytometric analysis elucidation of different malignant clones became evident [8]. Common usage of cytometric analysis might reveal greater incidence than expected especially in elderly patients with a low number of monoclonal lymphocytes. In the patient, we tried to treat the AML clone at the beginning. We observed remission in both AML and CLL clones. However, after the second cycle with dose-adjusted FLAG regimen relapse occurred. This might be explained by advanced age due possibly to developing genetic abnormalities. In the second case allogeneic stem cell transplantation was performed from HLA-matched sibling. At least 27 months after transplantation patient is alive and has complete hematologic cytogenetical remission for AML and CLL. Regarding the allogeneic stem cell transplantation limited number of transplanted patients has been reported and optimal transplant time is unclear [14]. If adverse prognosis is considered allogeneic stem cell transplantation might be the best option in transplant-eligible patient who are under 60 years old. Such patients should be transplanted after remission is obtained. It is questionable to perform allogeneic stem cell transplantation to obtain a remission for both AML and CLL clones. It seems reasonable to achieve remission for AML clone after performing allogeneic transplantation because of the aggressive course of the disease. Prospective studies are needed to prove this hypothesis. The third case showed 15% of blastic cells and was diagnosed as MDS with excess blast type II, however after 4 cycles of decitabine treatment transforming to AML and CLL was noticed. CLL development after the diagnosis of MDS or AML was not found in the literature. This is the first case from this point of view. It might be questionable that AML developed after administration of decitabine. The nature, duration and intensity of the treatment might explain the development AML but not CLL. CLL might have developed during the initial leukomogenic process of the disease.
As a conclusion, we reported 3 cases presented concomitant AML and CLL diseases, which have no exposure to radiation and cytotoxic agents. These cases support the idea that AML and CLL might demonstrate two separate disease processes originating from abnormal different clones. Allogeneic transplant should be an option in transplant eligible patient.
The authors have no relevant conflicts of interest to disclose.