Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Review Article - (2015) Volume 3, Issue 3
In vitro fertilization (IVF), a form of assisted reproductive technology has expanded since its introduction in the 1970s to enable patients with prolonged infertility and/or clinical complications to produce biological offspring. This review analyzes the topics of controversy surrounding IVF, weighing evidence concerning contemporary fertility techniques that aim to advance the field of IVF. A comparison of single embryo transfer to double embryo transfer, in the context of economic expenditure and the likelihood of multiple pregnancies, provides support for electing the former. An ethically controversial topic is preimplantation genetic screening, a technology with the potential to reduce the incidence of genetic abnormalities, thereby increasing rates of healthy pregnancies. Lastly, the integration of in vitro maturation (IVM) can allow for a more diverse patient population to benefit from IVF treatment, while simultaneously avoiding several of the associated disadvantages. The future of IVF rests on continued research and the resulting widespread integration of increasingly effective methods.
<Keywords: Embryo transfer; Insurance coverage of infertility; Outcome prediction models; Preimplantation genetic screening;
aCGH: Array Comparative Genomic Hybridization; AMA: Advanced Maternal Age; ART: Assisted Reproductive Technology; ASRM: American Society for Reproductive Medicine; DET: Double Embryo Transfer; E2: Estradiol; eDET: Elective Double Embryo Transfer; eSET: Elective Single Embryo Transfer; ES-IVM – Estrogen Suppresed In vitro Maturation; ET: – Embryo Transfer; FISH: Fluorescence In Situ Hybridization; FSH: Follicle-Stimulating Hormone; GnRH: Gonadotrophin-Releasing Hormone; hCG: Human Chorionic Gonadotrophin; ICSI: Intra-Cytoplasmic Sperm Injection; IVF: In vitro Fertilization; IVM: In vitro Maturation; LH: Luteinizing Hormone; MET: Multiple Embryo Transfer; NHS: National Health Service; NICE: National Institute for Clinical Excellence; OHSS: Ovarian Hyperstimulation Syndrome; PCOS: Polycystic Ovarian Syndrome; PCR: Polymerase Chain Reaction; PGD: Preimplantation Genetic Diagnosis; PGD-AS: Preimplantation Genetic Diagnosis with Aneuploidy Screening; PGS: Preimplantation Genetic Screening; POF: Premature Ovarian Failure; SART: Society for Assisted Reproductive Technology; SET: Single Embryo Transfer; SGDs: Single-Gene Disorders; US: United States
The emergence of assisted reproductive technology (ART) and In vitro fertilization (IVF) was marked by the birth of Louise Brown in 1978 in the United Kingdom following the materialization of assisted reproduction in the 1960s and 70s [1,2]. Shortly thereafter, crucial developments were made within this field. Although ART, defined as a treatment for both fertile and presumed infertile patients during which both the eggs and sperm are processed in order to establish a viable pregnancy, is predominantly used for infertility treatments, it has also developed into a suitable option for fertile couples with a familial history of inheritable genetic conditions [3]. ART consists of varied approaches, with IVF recognized as a prominent method, responsible for over 99% of the 176,247 total ART cycles [4]. In IVF, harvested eggs and sperm are introduced In vitro to initiate fertilization and ultimately, embryo development. Once the embryo matures to either the cleavage (day 2-3) or the blastocyst (day 5-6) stage, it is transferred to the mother’s uterus with the ultimate goal of implantation within the uterine lining and initiation of pregnancy. The use of one embryo to achieve pregnancy is specifically known as ‘single embryo transfer’ (SET) and a single fetus brought to term is designated a singleton pregnancy [5]. Another procedure to assist in fertility is intra-cytoplasmic sperm injection (ICSI), an application of ART designed for male-factor infertility. ICSI, insertion of sperm directly into the oocyte as to avoid the many obstacles the sperm encounter naturally, may be used concomitantly to or in place of IVF, depending on the patient circumstances [5,6].
Preimplantation genetic screening (PGS), a profiling technique that screens for specific genetic diseases and aneuploidy (abnormal chromosome number) prior to embryo implantation, is partially responsible for the popularity of IVF among both fertile and infertile couples. In vitro maturation (IVM), an emerging variation to IVF in which the oocyte is not only fertilized but also matured outside of the uterus, has also broadened the field by enabling women with a variety of contraindications to standard IVF, including women with polycystic ovarian syndrome (PCOS) or cancer patients undergoing chemotherapy, to take advantage of ART [7-10]. Despite the excitement surrounding IVF, the use of multiple embryo transfer (MET), introducing more than one embryo during the IVF procedure (with emphasis here on double embryo transfer (DET)), significantly improves the probability of multiple pregnancy, which is defined as the delivery of two or more infants with at least one born alive [11]. Multiple gestations introduces various potential complications to both mother and child, ensuing costs, as well as increases the risk of prematurity and intrauterine growth restriction among others, hence the ensuing skepticism regarding a MET approach to IVF.
SET versus DET and MET
Multiple pregnancy and MET
A challenge in IVF is selecting the appropriate number of embryos for uterine transfer in order to both enhance the pregnancy rate and reduce the chance of multiple pregnancy. The frequent use of DET is partially attributed to a higher probability of implantation and pregnancy simply due to the fact that an additional embryo is transferred [12]. However, the potential for both embryos to implant is higher, leading to a greater incidence of multiple pregnancy [13]. From a patient’s standpoint, the exhaustive process of IVF would ideally be completed in one cycle, which may explain the frequency with which DET is opted for, especially among patients struggling with infertility who want to maximize their chance of implantation [12]. A 2006 Canadian study showed that DET was utilized in 55.8% of all ART procedures, with 46% of all births attributable to multiple pregnancy. Not only was there a high rate of twin births, but, when compared with singletons conceived via IVF, twins showed a 10-fold increased risk of preterm delivery (<37 weeks), a 7-fold increased risk of delivery prior to 32 weeks of gestation, and a 12-fold increased risk for birth weight less than 2.5 kg [14]. In order to remedy the increased likelihood of twin or multiple births associated with DET for IVF-seeking couples, it is imperative to implement techniques like SET that will reduce the number of embryos necessary for successful pregnancy while avoiding potential complications.
The enhanced likelihood of adverse outcomes due to multiple pregnancies following DET prompted researchers to generate a mathematical model, the Combined Formula, to predict pregnancy outcomes using only implantation rates and the number of embryos transferred. The Combined Formula was applied to data from multiple IVF centers to predict either failed or multiple pregnancy, with an error rate of 1.4% [15]. Estimation of the implantation rate, the total number of viable fetal heartbeats divided by the total number of embryos transferred, can drive the course of treatment to attain the desirous outcome. For example, this study suggests that a high implantation rate combined with an increased number of transferred embryos substantially heightens the risk of multiple pregnancies while insignificantly affecting the overall frequency of pregnancy [15].
As the issue of multiple pregnancies becomes an increasingly relevant public health concern [16], researchers are putting more focus on the development of models capable of predicting the outcome of a given pregnancy, based on certain characteristics identified as indicators of either adverse or favorable ART results. As Dr. Hunault and colleagues stated, “The ability to identify those treatment cycles at particular risk of leading to multiple pregnancy and for which single ET would not reduce the chance of achieving a singleton pregnancy may encourage the adoption of single ET into clinical practice” [17]. In order to most accurately ascertain probabilities of success with embryo transfer (ET), it is of utmost importance that an embryo with the highest likelihood of implantation is chosen. While currently there is no universally accepted method for picking such an embryo, some new models show promise, albeit lacking verification and publication of results [18,19]. Certain characteristics, such as duration of infertility, maternal age, number of ART treatment cycles, and patient pathology, are most inversely correlated with embryo quality and, thus, pregnancy success [17,18,20,21]. The hope of these models is that multiple pregnancy rates can be greatly diminished by screening patients to determine good candidates (and embryos) for SET and thereby decreasing use of DET.
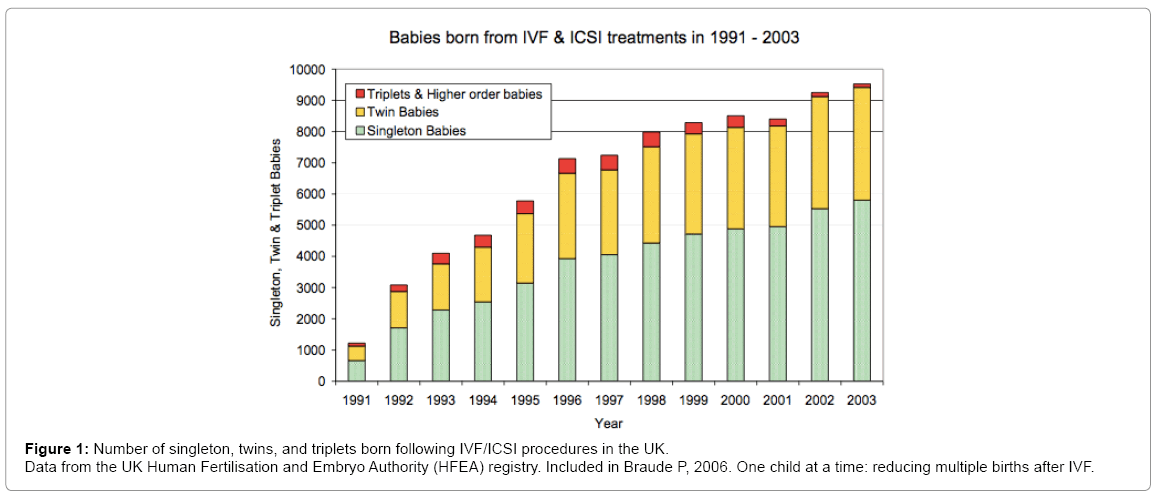
Figure 1: Number of singleton, twins, and triplets born following IVF/ICSI procedures in the UK.
Data from the UK Human Fertilisation and Embryo Authority (HFEA) registry. Included in Braude P, 2006. One child at a time: reducing multiple births after IVF.
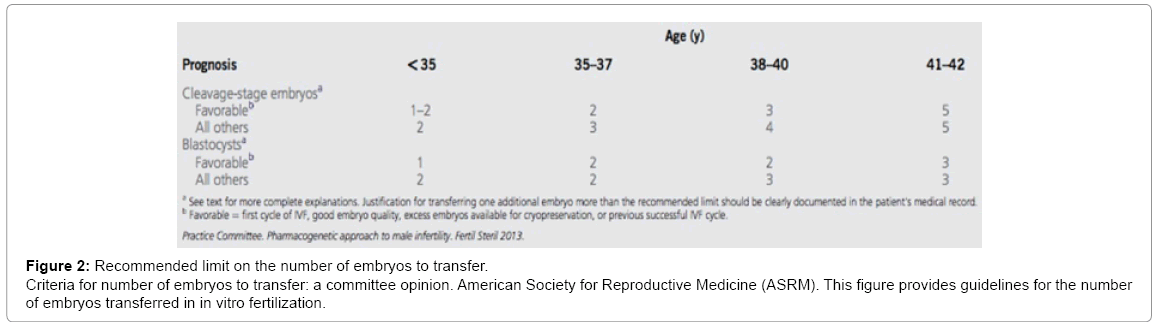
Figure 2: Recommended limit on the number of embryos to transfer.
Criteria for number of embryos to transfer: a committee opinion. American Society for Reproductive Medicine (ASRM). This figure provides guidelines for the number of embryos transferred in in vitro fertilization.
While DET is beneficial in yielding higher live birth rates in poor responders (defined as patients with a low number of oocytes available for retrieval contributing towards low pregnancy rates), the inevitable issue of multiple births needs to be addressed [22]. Apprehension about the rising incidence of multiple pregnancy associated with the use of DET has led to growing interest in elective single embryo transfer (eSET). Following the evaluation of two morphologically intact embryos, one of the two is selected for transfer, with the intended result being a singleton pregnancy [17]. However, a major source of concern among patients and clinicians is the evidence that use of eSET may reduce overall live birth rates [23,24]. The fear of an unsuccessful pregnancy with the primary IVF cycle as well as the possible need for additional treatments has likely negatively impacted patients’ decisions to choose eSET over alternative techniques such as DET. A 2003 study indicated as such, with results showing that infertile mothers had a significant preference for DET over eSET, specifically citing the possibility that the resulting infants might be the only children the mothers are successfully able to have [12].
In a study published by the New England Journal of Medicine, Dr. Ann Thurin and colleagues compared implantation and live birth outcomes of a population in which the patients were randomly assigned to undergo SET or DET. A pregnancy culminating in at least one live birth occurred in 38.8% and 42.9% of patients using SET and DET, respectively [25]. A parallel study yielded comparable data with the additional finding of a 33% increase in incidence of multiple pregnancies following DET [26]. Even more astonishing than the aforementioned data is the finding that only around 20% of multiple gestations occur with natural conception [27]. The results of a very recent study showed even more reason to choose SET: an ART treatment of two cycles of SET results in comparable pregnancy rates to that of one cycle of DET, while concurrently causing a drop in multiple pregnancy rates by more than 90% [28]. As indicated, a decline in twinning rate following SET or DET is feasible without a drop in overall pregnancy and live-birth rates by, when given the choice, opting for SET instead of DET.
Many factors, such as gene-related concerns, embryo quality, and maternal age, play a role in the prognosis of patients for pregnancy. In women aged 35 years and older, eSET is not the most viable option unless the patient has healthy embryos and a favorable prognosis. Patients determined to have “poor prognoses” are those with inadequate responses to IVF and, ultimately, lower pregnancy and live birth rates. In this group, the pregnancy and live birth rates for eSET were 17.5% and 10.8%, respectively, compared with 35.4% and 27.8% for elective double embryo transfer (eDET), revealing eDET to be the more suitable option [22]. Although the likelihood of multiple pregnancy associated with DET is a major concern, it is important to understand that the best option of technique ultimately depends on the patient’s health.
In an attempt to increase pregnancy and live birth rates while reducing the incidence of multiple pregnancies, the American Society for Reproductive Medicine (ASRM), in conjunction with SART, developed guidelines to assist couples considering ART [29]. These guidelines provide suggestions for the usage of SET versus DET dependent on patient age. While SET is favored in most cases, DET may be more efficient and less costly for patients of increased age [30,31]. Studies have also revealed that aside from SET attaining comparable pregnancy and live birth rates to DET as well as decreased risk of multiple pregnancy, SET is more cost efficient than DET in the longterm [21,24,32,33].
Widespread costs of IVF procedures
SET and DET methods share the goal of enabling couples with infertility complications to conceive; however, transfer of two embryos in DET (versus a single embryo in SET) results in a high likelihood of multiple pregnancy that can create large cost differentials. The longterm costs associated with IVF twin birth are significantly higher compared to that of an IVF singleton; yet, DET is more often utilized, mostly due to SET often requiring multiple cycles of uterine embryo transfers [11,14,32,34,35]. The use of DET often results in an increased financial burden both on the family and healthcare system, so much so that legislation has been, and continues to be, globally enacted in an attempt to decrease the use of DET in favor of SET [36]. For instance, Sweden only allows the transfer of one embryo per cycle while Denmark limits the transfer of two per cycle [12,22].
ART treatments, at the very least, incur costs for antenatal care, laboratory resources, hormones, medications, physician labor, and embryo transfer, amongst others [30]. However, the typical estimated financial burden of pregnancy does not include potential expenses relating to complications incurred during pregnancy and/or birth, or even the birth of twins, all of which are more frequent with the use of DET instead of SET [33]. The results of one study showed a 2.5% incidence of twins stemming from viable SET pregnancies while there was a grossly statistically significant 54.2% multiple pregnancy occurrence rates with DET pregnancies [37]. While extreme, these numbers are comparable to the findings of many other studies, and only further support the idea that, complications aside, electing to undergo DET runs the risk of multiple pregnancy [21,24,25,35].
A study looking at cost of IVF singleton versus multiple pregnancies found that not only were twins born earlier in the pregnancy term, but their birth weight was also noticeably lower than that of singletons. The same study also determined that 100% of patients with twin pregnancies, in contrast to 79% of patients with single pregnancies, required hospital care prior to birth [38]. These premature births and resultant lower birth weights lend themselves to post-birth problems requiring medical attention and, therefore, additional costs. When comparing hospital admissions and complications of IVF twins to those of IVF singletons, a separate study found statistically significant data indicating that not only did IVF twins require longer and more frequent hospitalization, but IVF twins also had a 2.5-fold increased risk of hospital admission across all levels of care. Even following exclusion of premature birth statistics from the data set, Dr. Pinborg and her team still found a 1.4- fold higher risk of hospitalization of IVF twins over IVF singletons [39]. Lastly, for a singleton pregnancy, about 60% of total pregnancy costs were attributable to maternal care, whereas in twin and higher-order births, 70% and 85%, respectively, of the total healthcare costs were directed towards infant care [40].
The increased financial burden associated with IVF and possible subsequent multiple pregnancy does not fall solely on the couple involved, but is in part covered by their country’s healthcare system, depending on the specific country’s healthcare coverage particulars [5]. An interesting result from a study conducted in 2006 demonstrated that “socio-economic characteristics were comparable for both the [eSET and DET] groups, indicating that the difference in costs between eSET and DET (such as productivity costs and out-of-pocket costs) was not affected by difference in socio-economic characteristics” [41]. At the time of a study conducted by Dr. Ledger and colleagues, the National Health Service (NHS) in the United Kingdom only paid for approximately 25% of IVF and other infertility treatments implemented. However, the NHS concurrently takes responsibility for a majority of expenses from natural pregnancy and newborn care, complications included [42]. With these facts in mind, a cost-benefit analysis was conducted, focusing on multiple versus single births following IVF as it impacts the NHS. Results strongly favored single births, as it was seen that single IVF births sustained only 46% of total costs while encompassing 73% of total live births. The other 54% of costs stemmed from the other 27% of the study population that incurred multiple births [42]. If NHS coverage of fertility treatment is expanded to equal that of all aspects of natural pregnancy (an ethical issue unto itself), it stands to reason that the NHS could curb potential IVF payouts if guidelines are put in place to encourage single births. Results demonstrated as such, indicating that if more cycles of SET were financed for patients (in order to diminish gaps in perceived pregnancy chances between SET and DET), one-third of DET patients would be willing to undergo SET instead [12].
As it stands, NHS requirements for couples hoping to receive IVF treatments include demonstrating duration of infertility of no less than two years and, if the woman is over the age of 40, that IVF has not been used before [43]. However, this is itself a problem, as the waiting period preceding treatment not only causes the average age of the women undergoing IVF to increase, but this older patient population brings with it higher costs and a larger number of complications. As many studies have shown, maternal age is the most important, and best, indicator of pregnancy success; it generally informs both embryo quality and frequency, which decrease with increasing age, while abnormalities rise [18,31,44]. Advanced maternal age (AMA), patients 40 years old or more, require larger doses of follicle-stimulating hormone (FSH) to stimulate the follicle to produce collectible eggs as well as more monitoring and tests throughout the treatment cycle [5,30,45]. While progress has been made in terms of pregnancy success in older women (rising from 20.0% to 50.2% between 1997 and 2006), the proportion of women of increased age able to become pregnant is still significantly below that of younger women [30,46].
Unlike many Westernized countries, the United States (US) is only now implementing more of a nation-wide healthcare plan; it is still the case that several US insurance providers do not cover infertility treatments [11]. Dr. Stillman notes that “multiple factors, including the existence of national health care plans providing complete or partial coverage for assisted reproduction for most Europeans and legislation requiring single ET (SET) in Belgium and Sweden, have led to more rapid implementation of SET and lower multiple-pregnancy rates in Europe than in the United States” [37]. Without adequate ART insurance coverage and financial support available in most states, a large part of the United States has some of the most expensive ART procedures in the world [47]. Resultantly, most couples seeking infertility treatment in the US choose to have more embryos transferred, which creates smaller, short-term out-of-pocket costs due to higher chance of a viable pregnancy with just one cycle [48]. Insurance mandates in the US have been shown to have observable effects on the use or disuse of certain ART treatments, with more use of IVF and ICSI in states with mandatory insurance coverage [49]. At the time of a study conducted by Dr. Reynolds and her team in 2003, fourteen states had enacted varied infertility and insurance laws mandating some degree of patient coverage for treatment. Upon analyzing IVF treatment choices and neonatal outcomes in insurance-mandated states compared to noninsurance states, researchers’ findings suggested that insurance coverage not only reduces the number of embryos transferred for each patient, but also the number of higher order births [11]. Since the publication of Reynolds’ study, only one more state in the US has enacted IVF coverage insurance mandates, bringing the total to fifteen [50].
While Dr. Reynolds’ study did not find a large amount of statistically significant results promoting increased insurance coverage, a more recent study decisively demonstrated that insurance and out-of-pocket costs greatly influenced the patient’s selection of infertility treatment. Researchers limited the study population by including only patients without insurance or with the state-mandated insurance coverage. The uninsured patients were then offered the option of Shared Risk, which only incurred expenses upon a successful live birth and also minimized the cost differentials between DET and possible multiple cycles of eSET [37,51]. Once the financial disincentives of eSET were minimized, the choice of eSET over DET increased significantly from a rate of 16% for patients without either insurance or Shared Risk to 24% and 25% for those with Shared Risk and insurance coverage, respectively. As anticipated, the utilization of eSET decreased significantly as out-ofpocket expenses for the patients increased [37]. This study strongly supports the notion that it is fiscally advantageous for insurance companies as well as healthcare systems to cover a majority, if not all, of infertility treatments. Conclusive data not only paves the way for a more efficient healthcare system, but the implications of the potential for reduced costs and the use of those excess savings are enormous and largely unexplored.
Applications and procedure
The clinical value of PGS coupled with preimplantation genetic diagnosis (PGD) is in selecting genetically normal embryos for women of advanced maternal age (AMA) with recurrent pregnancy loss who are seeking use of methods such as IVF [52]. The technical distinction between PGS and PGD is pertinent in fully understanding these techniques—PGS is the generalized screening method to detect aneuploidy (abnormal chromosome number) and indicators of genetic diseases, whereas PGD is the actual diagnosis of embryos with genetic abnormalities. By screening for predictive conditions prior to implantation, couples may increase their potential for conception of a viable embryo. PGD fills an imperative niche in preimplantation medical care because it detects abnormal embryos that otherwise may appear normal [53]. Despite these advantages, there is concern about the ethical ramifications that exist when couples implement this technique, specifically for gender selection purposes. Ultimately, the primary use of these screening approaches should be as a beneficial tool for couples with infertility issues or who are carriers of inheritable conditions and hoping to have healthy, disease-free children.
Cleavage-stage, blastocyst-stage, and polar body biopsies offer several methods to perform genetic screens of both maternal and paternal DNA. Screening of cleavage stage embryos, which arise during day 2-3 of fertilization, have been compared in efficacy to blastocyst stage embryos at day 5-6 in order to better determine the benefits of each. While cleavage-stage embryos are more easily cultured in a laboratory and yield one or two blastomeres, blastocysts have shown an increased association between embryo morphology and chromosomal status, which helps to more accurately, predict the outcome of embryo transfer [54-57]. Additionally, biopsy at the cleavage-stage has to shown to potentially cause harm to the embryo, thus creating major ethical concerns [57]. Polar body biopsies, while both ethically acceptable because of no handling of the pre-embryo as well as helpful when the embryos themselves are unable to be biopsied, are limited by the lack of paternal genetic information in polar bodies [55,58]. Biopsy testing for aneuploidy and single-gene disorders (SGDs) can be done using fluorescence in situ hybridization (FISH) and polymerase chain reaction (PCR), respectively [52,59]. FISH introduces gene-specific probes to ascertain the number of specific chromosomes that may indicate aneuploidy. Currently, chromosomes 13, 15, 16, 17, 18, 21, 22, X, and Y are the most common targets of PGD and FISH, but as to which of the listed chromosomes are screened for varies by fertility center [44,53]. Identification of inheritable diseases requires additional genetic material; therefore, PCR is used to amplify causative mutation sites for detection of particular DNA sequences characteristic of inheritable diseases [59].
Advantages of PGD in aneuploidy testing
Numerous studies reveal a direct correlation between advanced age, aneuploidy, and spontaneous abortion, as well as an inverse relationship with rate of implantation [44,45,53,60]. As such, research was conducted to evaluate the beneficial effects of PGD-aneuploidy screening (PGD-AS) on implantation and spontaneous abortion rates [52]. PGD-AS serves to not only prevent chromosomal abnormalities, but also to reduce the number of spontaneous abortions and multiple pregnancies [45,61]. While PGD-AS via FISH would theoretically increase implantation and live birth rates by selecting for chromosomally normal embryos with the highest likelihood of pregnancy success, trials researching this have been relatively inconclusive. Results suggest that, to increase the chance of a viable fetus for women of AMA, “18 genetically normal PGD-AS embryos have to be transferred to obtain one extra viable fetus” [52]. However, implantation of such a large number of additional embryos staggeringly increases the risk of multiple pregnancies. The statistical ineffectiveness of FISH may be attributed to the potential for mosaicism (populations of cells within the single embryo presenting different genotypes) as well as a limited fraction of chromosomes encompassed in aneuploidy detection [62]. Mosaicism within the embryo tested using PGD and FISH demonstrates the limitations of these techniques, since the mosaicism of the cells sampled may not be characteristic of the whole population of embryo cells [55,63]. As it stands, a majority of preimplantation embryos contain some abnormalities, whether it is aneuploidy or mosaicism, so better testing would also allow enhanced differentiation between minor and potentially catastrophic abnormalities [64]. So, the field of IVF would benefit from screening techniques that more accurately and extensively detect chromosomal anomalies, leading to better reproductive success for IVF-seeking couples.
Recent improvements, including array comparative genomic hybridization (aCGH), have improved the effectiveness of PGS by encompassing analysis of all 24 chromosomes. This new variation on aneuploidy screening allows clinicians to more accurately observe genetic abnormalities that may go undetected when PGS-AS is conducted via FISH [62,65,66]. For women of AMA and couples experiencing infertility issues, more accurate screening methods testing for both aneuploidy and translocations (rearrangement of DNA via nonhomologous chromosomal recombination) is pivotal in selecting the most genetically normoploid and viable embryos for IVF, resultantly improving likelihood of conception and potentially decreasing the number of embryos transferred each cycle [67]. In one study, the percentage of embryos showing aneuploidy jumped from 32.8% for patients 40 years old to 65.8% for patients 46 years of age [66]. In non-transferred embryos from women of AMA, 9.4% of the embryos presented one or more aneuploidies left unnoticed by FISH were detected with aCGH [62]. A secondary benefit of aCGH is the reduction in time necessary for effective embryo implantation and development. Success with traditional IVF can require 2 to 9.8 years (average of 6 years); fortunately, the data indicates that PGD can reduce the average time frame to a minimum of 3 months or roughly 1.4 IVF cycles [68]. This decrease in duration prior to pregnancy realization is paramount for those who are pursuing ART. With 3 months of IVF and accurate PGS techniques, couples will undoubtedly save on medical expenses while simultaneously screening for aneuploidy, translocations, and other chromosomal conditions as compared to usage of earlier techniques. Furthermore, with these increasingly accurate screening procedures and the associated drop in conception time, the need to implant multiple embryos may subside, reducing the incidence of unintended twin (or triplet) conception via IVF.
Utilization of PGD for SGDs and X-linked diseases
One of the most clinically valuable advantages of PGD is detection and avoidance of particular SGDs. This method of prenatal diagnosis can help couples who are carriers of SGDs such as cystic fibrosis or the X-linked diseases hemophilia A and B. In a clinical trial, PCR-amplified DNA fragments were analyzed using individualized PGD tests specific for the genetic makeup of each couple, allowing targeted testing for disorders of interest. The trial further indicated that this personalized method of PGD led to a 38% increase in patients with a live birth or ongoing pregnancy, in contrast to rates of 13% to 29% in previous trials where solely single-gene PGD methods were used [59]. Preimplantation diagnostic methods provide the potential for improved chances of delivering healthy offspring by avoiding transfer of embryos testing positive for SGDs. However, couples do have to be counseled on the possibility of unearthing genetic abnormalities that the patients were previously unaware of [55]. If the couple elects to utilize more precise testing, the need for multi-embryo transfers and possibility of medical complications will most likely be minimized.
Ethics of PGD
PGD-assisted sex selection can significantly benefit couples challenged with X-linked diseases; by selecting for genetically female (XX) embryos, couples can likely avoid the potential for a male child to inherit an X-linked dominant disease. In using PGD to analyze singular genes of X-linked disorders, the X-chromosome in combination with the numerical element of the sex chromosomes is considered an acceptable diagnostic strategy due to the ability to check for consistency between the two components [69]. However, the controversial use of PGD in sex selection due to a personal preference is a considerable ethical concern. In a survey regarding PGD use in IVF, researchers found that “twothirds of Americans support the use of PGD to prevent the birth of a child who would develop a fatal childhood disease, and just under 40% supported its use for sex selection” [70]. A more recent study published observed that 20 of 38 fertile patients, both those under and over the age of 35, indicated “gender selection” as the primary reason they chose to undergo chromosomal screening [71]. The issue with sex selection is that many deem it as discrimination against a particular gender and a mechanism of gender bias. In countries like China and India, the preference for male offspring supersedes that for females and the increased availability of gender selection via PGD would likely result in a spike in the number of couples have male children [70]. In terms of allocating of resources, it is advisable that clinicians and the general public ensure that PGD is used solely to optimize the welfare of couples with inheritable genetic disorders or those facing difficulties with conception.
Progress of IVF
Originally proposed to overcome the potential side effects of the standard ovarian stimulation technique characteristic of IVF, In vitro maturation (IVM) aims to induce the development of immature oocytes. Initially used for women with polycystic ovary syndrome (PCOS), IVM has become a viable option not only for normo-ovulatory women, but also for women with other contraindications that preclude the success of conventional IVF. PCOS, characterized by an ovary with a lack of dominant follicle and instead a large number of small follicles due to a hormonal imbalance, puts the patient at a much higher risk of developing ovarian hyperstimulation syndrome (OHSS) if standard IVF treatment is used [10,72]. Conventional IVF treatments typically involve a gonadotropin-releasing hormone (GnRH) agonist to inhibit an early luteinizing hormone (LH) rise to avoid early oocyte maturation and establishment of a dominant follicle, thereby allowing the growth and harvesting of multiple large follicles [73-75]. This procedure, IVFGnRH, has been found to be a milder form of hormonal stimulation for patients and decreases risk of OHSS and other complications. However, in treatment cycles where hormone levels were not thought to be a risk or concern, such as in normo-ovulatory patients, human chorionic gonadotropin (hCG) and follicle-stimulating hormone (FSH) are used to “prime” ovaries, typically called hCG and FSH priming, respectively [9,76,77]. IVM eliminates the need for excess gonadotropin stimulation to induce ovulation because the oocytes are collected while still of smaller size and are grown In vitro instead of in vivo [78]. The goal of IVM is to reduce or completely eliminate disadvantages associated with the typical IVF procedure, including the cost of hormonal administration, risk of ovarian hyperstimulation syndrome (OHSS), and the inestimable burden on patients [79]. The results from these various studies indicating improved fertilization and clinical pregnancy rates of IVM comparable to conventional IVF may make use of hormonal stimulation less frequent in the future [80].
Additionally, major concerns were allayed when data indicated that there was no increased incidence of congenital abnormalities or perinatal complications with usage of IVM [78]. Despite this, IVM is not widespread for a few reasons: PCOS women only represent 5-10% of ART patients, normo-ovulatory women do not typically have enough antral follicles required for early oocyte retrieval in IVM, and lastly, due to In vitro matured oocytes having a reduced developmental potential compared to those matured in vivo [10,78,81].
There is substantial room for improvement and study in IVM procedures, including but not limited to the administration of estrogen and progesterone, the additives in the culture, and the gonadotropins utilized [78]. Ample evidence has shown that hCG priming enhances oocyte maturation and clinical pregnancy rates, while evidence for FSH priming remains limited; however, because FSH is believed to improve follicular health and to increase the quantity and quality of oocytes, especially in PCOS patients, some studies continue to include this step while others have removed FSH priming from their protocols [78,80,82- 85]. By investigating these topics, the obstacles of lower implantation and maturation rates may be overcome. With the incorporation of IVM into IVF procedures so that the embryo is both grown and inseminated In vitro, not only will a more diverse group of patients benefit from IVF, but there will also be lower costs, burden, and likelihood of multiple pregnancy.
An emerging alternative
While the progression of IVM is encouraging, especially for those unable to utilize traditional IVF treatments, it still is not ideal due to the circumstances of certain patients, such as those with smaller than average follicles [10,72]. Estrogen Suppressed-IVM (ES-IVM) is a new and promising approach to IVM with slight modifications that eliminate the need for FSH stimulation and cycle monitoring. By removing the FSH stimulation step, ES-IVM has many benefits including reduced costs, fewer side effects, and lowered risks that are typically coupled with other IVM procedures [79]. The majority of IVM procedures use a small dose of gonadotropins or the patient’s natural cycle (in which there is no ovarian stimulation and instead the naturally growing follicle is collected for use), but data suggests this shortens the follicular phase, thus negatively impacting its growth and success [5,86]. ES-IVM instead uses a suppressive dose of estradiol (E2) that inhibits the development of a singular dominant follicle, thereby maintaining a larger group of small antral follicles from which oocytes can be retrieved. Additionally, the dose of E2 has easily predictable outcomes concerning the follicular response to the hormone, removing the need for expensive regular monitoring [79]. Concerns about lower implantation rates are alleviated because E2 elongates the proliferative phase of the endometrium, which may result in an improvement of those rates. Clinical pregnancy, live birth, and even implantation rates rivaled those of comparative natural-cycle IVM and low-dose stimulation IVM [79]. This study suggests that, upon demonstration of widespread success through further study, ES-IVM should become the preferred method of IVM in a diverse population of patients, ranging from normo-ovulatory women to those with contraindications as to usage of IVF; with comparable pregnancy rates and improved implantation rates, ES-IVM substantiates the ineffectiveness of FSH and provides a less costly and overwhelming process of IVM.
Choosing IVM
Women diagnosed with PCOS are unable to take advantage of standard IVF due to concomitant hormonal stimulation, whereas IVM would only be a worthwhile option if it resulted in similar pregnancy rates. Using IVM in PCOS patients has eliminated the risk of OHSS and has yielded comparable antenatal rates, in addition to a lower frequency of twin pregnancy [80]. Additionally, in a disorder characterized by ovarian resistance to FSH (thus excluding IVF as a viable option), IVM can provide the means for reproduction in these patients as well [87]. This is critical in that patients such as those affected by various hormonal disorders can also take advantage of IVF if used in conjunction with IVM. At the present, there is limited data on using IVM with IVF in normo-ovulatory women as well as the implantation and pregnancy rates as compared with conventional IVF [88]. The relatively few studies published indicate not only decreased embryo quality and viability but also a significantly lower implantation rate following IVM with IVF versus that of conventional IVF [8,77,78,83]. While advances have been made as to improving IVM protocol and ensuring better success with embryo transfer, due to the nature of patients undergoing IVM significantly larger numbers of embryos are needed for transfer to ensure comparable rates to IVF [9,89]. As such, the ethical concerns associated with the increased number of embryos usually transferred in IVM for PCOS patients cannot be put to rest without further study; that being said, with the rate of progress occurring with respect to IVM, it is not unreasonable to believe that SET may soon become an option for patients electing IVM with IVF.
With the increase in cancer survivors due to advanced research and treatment options, an option for conception is needed that can overcome the premature ovarian failure (POF) and infertility due to chemotherapy and radiation [8]. Dr. Chian’s study proposed a possible method of fertility preservation in these women: immature oocytes should be retrieved in an unstimulated menstrual cycle prior to starting chemotherapy, matured In vitro, and then vitrified (a specific form of cryogenesis, or freezing of embryos) [8]. IVF is often not as viable a choice because hormonal administration may stimulate tumor development [90]. This study had a remarkably high clinical pregnancy prevalence of 44.7%, comparable to standard IVF, and no adverse obstetrical or perinatal complications were identified. Although this study was intended for cancer patients beginning chemotherapy, Dr. Chian and colleagues suggested that this approach would be an effective and motivational solution for women with decreased fertility due to multiple sclerosis, certain autoimmune and genetic diseases, ovarian tumors, and endometriosis [8]. In a separate published case report, Chian and colleagues outlined their achievement of the first healthy live birth stemming from IVM with a natural menstrual cycle and oocyte cryopreservation with vitrification [7]. Not only does IVM provide a method for reproduction in these patients, but the promise of potential biological children may also improve the treatment process for the patients and serve as motivation. With the advances made in science, infertility is slowly being overcome and the conjunction of IVM with IVF will better help introduce the possibility of biological children for women with a multitude of complications and for whom it has previously been impossible.
Cryopreservation and fertility restoration
Until recently, women diagnosed with cancer were given a bleak prognosis for having a live birth due to the adverse effects treatments such as radiation and chemotherapy have on fertility. Studies indicate a constant 30-50% decrease in probability of successful pregnancy for cancer survivors [16]. The ASRM revealed in 2014 that oocyte cryopreservation (and its use with other forms of ART) is no longer an investigational procedure in fertility preservation for cancer patients due to the recent surge in data on clinical outcomes [16,29,90,91]. When discussing fertility treatment options, it is important to consider not only the method and timing of the gonadotoxic therapies, but also the specific cancer’s parameters, patient age, and partner status [92].
Two of the most commonly utilized procedures in fertility preservation are ovarian tissue cryopreservation and oocyte cryopreservation. In order to restore fertility, ovarian cortical tissue is reimplanted into the pelvic cavity, an orthotopic site, or a heterotopic site. This procedure is then followed by natural conception or oocyte collection and ART [91,93]. While in theory either the orthotopic site or heterotopic site can be used as the site for implantation, so far live births have only resulted from orthotropic transplantations [91].
Excision and cryobanking of a young patient’s ovarian tissue presents an interesting alternate approach to fertility preservation. Ovarian tissue cryopreservation is the only treatment option available to young, prepubescent girls diagnosed with cancer because other procedures involve hormonal stimulation to induce ovulation and oocyte retrieval [91]. Another advantage to this method is that since there is no hormonal stimulation, there is no delay in cancer treatment. It is suggested that there is a negative correlation between increasing age and the number of immature oocytes able to be retried from ovarian tissue [94]. Coupled with this notion is the observation that cryopreservation of ovarian tissue is only really able to preserve primordial and primary follicles because of their increased resistance to cryoinjury from the freezing procedures involved [91,94]. As such, ovarian tissue cryopreservation and retrieval are especially suited to younger patients and provide hope that these patients may be able to achieve a successful pregnancy when desired. This topic is discussed further in an article we previously published [91].
A recent source of conflict among researchers and clinicians concerns the method for freezing the retrieved tissue. The two most widely-recognized protocols are slow cooling and vitrification, which differ from each other mostly in the rate that the tissue samples are cooled along with the concentration of the cryoprotectant used in the procedure [91]. Slow cooling occurs with careful, gradual decreases in temperature until the tissue reaches the desired frozen state. Vitrification involves a much faster cooling process and uses a more complex solution of cryoprotectants in order to better preserve the tissue samples in the cooling. While any challenges to the tissue’s environment may negatively impact the sample’s survival, it has been demonstrated that cleavage-stage embryos as well as blastocysts that do not sustain injury during the cryopreservation process, whether it be vitrification or slow cooling, can implant at the same rate as their fresh equivalents [58,77,90,95,96]. In one of the largest randomized controlled trials conducted regarding the matter, over 3000 fresh oocytes were compared to 3000 vitrified oocytes. Of the 92.5% vitrified oocytes that survived the freezing process, the study found cryopreservation had no significant impact on fertilization, development, or implantation of the oocytes compared to the controls. Clinical pregnancy rate per cycle and embryo transfer along with multiple pregnancy rate were also consistent between the study’s populations [97].
While these study results are encouraging, these techniques, especially in combination with IVM, still have improvements to be made before they become common in the field of ART. Currently, malignant tumors in women are a contraindication to retransplantation of ovarian tissue because of the risk of reintroducing cells that may metastasize to the ovaries after the re-transplantation [95,98]. However, for those patients with a cancer that has a low risk of reimplanting tumor cells, there is the possibility of follicle maturation In vitro without transplantation [92]. However, data from a 2013 study indicated that, while IVM is possible in immature oocytes retrieved from non-stimulated ovaries, there is a significant decrease in blastocyst survival following maturation, cryopreservation, and activation [99]. As discussed in a 2015 survey, complete In vitro maturation of oocytes from cryopreserved ovarian tissue has not yet been successful in humans [92]. While there is some indication of success and developmental potential of IVM oocytes following cryopreservation, there is currently not enough clinical data available concerning outcomes in patients with cancer to justify using it as standard of care, especially when compared to the significantly more successful rates seen in established IVF/IVM [77,99].
The introduction of ART, and IVF more specifically, was a muchneeded push for progress in the sadly under-funded and underutilized field of fertility. What began as a somewhat archaic procedure has now progressed to the possibility of transferring one, two, or more embryos (SET, DET, and MET, respectively). Couples are now even able to choose which IVF method they would prefer, whereas previously it was solely at the clinician’s discretion. These technological advances have spread to encompass genetic screening prior to treatment as well as alternative methods, such as IVM, to enhance not only the viability of the pregnancy but also the live birth rate while minimizing neonatal complications stemming from the high rate of multiple pregnancy present in IVF procedures.
While the advancements made to the field of ART are very apparent, there is certainly room for improvement. The frequency with which multiple pregnancy and associated complications occur in women following embryo induction using DET should, in theory, deter usage of DET. Unfortunately, this does not seem to be the case, as DET is still opted for at a rate comparable, if not higher, to SET.
Preference for DET over SET is, for the most part, not medically related. While some patients reasonably elect DET due to having “poor prognosis” and wanting to maximize their chance to reproduce, too often it seems that couples are basing their choice on their short-sighted understanding of the financial costs associated with SET versus DET. While SET may take more than one treatment cycle, and thus invoke multiple times the treatment cost, it does not have the high incidence of multiple pregnancy and complications that DET does, causing DET treatments to incur greater cumulative expenses. As such, more governmental and insurance regulation is needed to ensure that IVF is used as efficiently as possible to maximize resources as well as societal benefits.
The efficacy of IVF is strengthened when screening and diagnostic techniques are implemented. Due to the awareness of well-documented DNA sequences that are indicative of single-gene disorders, couples with a familial history of certain disorders can feel comforted in knowing that many of these physiologically degenerative and emotionally tolling illnesses will not arise in their future offspring. However, along with the advantages of PGS, there are apparent ethical concerns surrounding its potential misuse, including gender selection for personal preference and even the potential for selection of eye color and other physiological features. With ethics in mind, it is important to consider those who would most benefit when guiding usage in PGS and IVF procedures and work to tailor therapies towards this population.
By removing the excess gonadotropin stimulation and retrieving immature oocytes for development In vitro, IVM provides a way to further advance the field of IVF. Its incorporation into traditional IVF procedures and cryopreservation methods will enable a clinically diverse group of patients to benefit from ART, including women with PCOS, genetic disorders, and cancer survivors as well. Furthermore, with the utilization of IVM several of the disadvantages of IVF can be eliminated: there will be decreased costs, less of a burden on the patient (without the need for monitoring and regular hormonal admission), and most importantly, a decreased likelihood of multiple pregnancy. With further research, IVM and fertility preservation techniques will result in effectiveness similar to that of traditional IVF.
IVF is the foundation of a massive surge in technologies related to the field of assisted fertility. The global use of IVF escalates regularly, and scientists as well as governments have been working to accommodate this popularity while increasing public access to IVF. As such, there has been a jump in the use of SET versus DET in recent years, especially in those countries with a nationalized healthcare system, such as the UK. While the United States does not yet have such a universal healthcare system, recommendations for efficient resource distribution and guidelines have been created to steer fertility treatment and correlated methods such as PGS and IVM. Undoubtedly, In vitro fertilization is a highly efficacious tool, requiring additional research to further assist couples most in need of this technique while simultaneously needing governmental and clinical control to ensure these methods are being ethically used.
The authors would like to thank Mr. Paul J. Fine for his proofreading, formatting, and editing contributions.