Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2018) Volume 8, Issue 1
Abstract Objectives: Plasmapheresis has been repetitively reported as an effective treatment in hypertriglyceridemiainduced acute pancreatitis (HTG-AP). However, due to heterogeneity in presenting severity, different definition of clinical end-points and lack of well-matched control group, a definitive role of plasmapheresis is yet to be determined.
Methods: We reviewed a cohort of 142 unique patients of HTG-AP, in which 15 cases were treated with plasmapheresis. We compared the epidemiologic characteristics, presenting clinical severity and various clinical end-points between plasmapheresis group and non-plasmapheresis group directly and after successful propensity score match. The clinical trajectory of plasmapheresis group and post-match nonplasmapheresis group were plotted and compared.
Results: Patients who underwent plasmapheresis had higher triglyceride levels on admission, and had a trend toward more severe pancreatitis. The unmatched cohort revealed that plasmapheresis group had longer hospital stay, required more intravenous insulin, and had longer duration of nil per os. However post-match comparison revealed that plasmapheresis had no effect on clinical outcomes. Despite the successful match of epidemiologic characteristics and presenting clinical severity, plasmapheresis group was responding slower than post-match nonplasmapheresis group, which suggests the existence of unmeasured confounding factors and possibility of obscured benefit given the similarities in various end-points.
Conclusions: Although plasmapheresis had no apparent benefit or harm, there likely was residual confounding based on the different clinical trajectories between the plasmapheresis and non-plasmapheresis groups. Randomized controlled trial, or a larger multicentre observational study taking into consideration the clinical trajectory is needed to further evaluate the role of plasmapheresis in HTG-AP.
Keywords: Hypertriglyceridemia; Acute pancreatitis; Plasmapheresis
Hypertriglyceridemia (HTG) is a well-recognized cause of acute pancreatitis (AP), accounting for 1-4% of all episodes [1,2]. Severe HTG (serum triglyceride (TG) level above 1000 mg/dl) results from increased production or decreased metabolism of lipid products secondary to genetic and environmental factors [3-5]. The exact mechanism of hypertriglyceridemia-induced acute pancreatitis (HTGAP) is not clearly defined; the most widely accepted theory suggests that excessive TG are hydrolyzed by pancreatic lipase to free fatty acids, which form micellar structures that activate platelets and damage the vascular endothelium and acinar cells, leading to local and systemic inflammation [6,7].
Standard treatment for HTG-AP consists of pancreatic rest, fluid resuscitation, and symptom control [8-11]. Adjunctive treatment with subcutaneous or intravenous (IV) insulin, and heparin might be beneficial through reducing the TG level, although no guidelines endorse these treatments [12-15]. Plasmapheresis rapidly removes serum TGs, and has often been reported in previous literature as an effective treatment method [16-21]. However, due to the heterogeneity in reported severity of AP and clinical outcomes used to determine efficacy, and lack of well-balanced control and treatment groups, the role of plasmapheresis in HTG-AP remains unclear [6,22].
In the present study, we reviewed a cohort of patients with HTG-AP. We evaluated the clinical effectiveness in decreasing serum TG levels and the severity of AP. We also evaluated the effects of plasmapheresis on clinical outcomes by matching patients who received and who did not receive plasmapheresis.
Database setup
We retrospectively reviewed the electronic medical records of patients who were diagnosed with HTG-AP during a hospitalization at John H. Stroger Hospital of Cook County, Chicago IL from January 1, 2010 through July 31, 2016. We identified potential patients using the discharge diagnoses of AP (i.e., ICD 9 code [577.0] and ICD 10 code [K85.9]). We confirmed the diagnosis of AP based on American College of Gastroenterology guidelines, which requires that at least two of the following three criteria are fulfilled: 1) abdominal pain characteristic of acute pancreatitis, 2) serum lipase equal to or higher than 3 times of the upper limit of normal, and 3) characteristic findings of acute pancreatitis on CT scan [23]. We included patients who had an admission serum TG level of ≥ 1000 mg/dl on admission. We excluded patients <18 years of age, presence of gallstone identified by abdominal ultrasound, or who had missing data as outlined in the Data Collection section.
The present study was approved by the Institutional Review Board of Cook County Health & Hospitals System, Chicago. The database was set up and maintained by the Department of Medicine, Cook County Health & Hospitals System [24].
Data collection
We subcategorized patients into plasmapheresis and nonplasmapheresis groups based on whether they underwent plasmapheresis during their hospitalization. We abstracted the following characteristics for each patient: age, gender, past medical history (hypertension, diabetes, hyperlipidemia, and metabolic syndrome), substance use (alcohol, tobacco, illicit substances), and laboratory values. The reason for initiating plasmapheresis was extracted from clinical documents. We calculated Ranson’s Criteria and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score to assess the severity of acute pancreatitis [25,26].
Definition of clinical outcomes
We specified hospital length of stay (LOS) as the primary outcome; we collected several additional clinical end-points as secondary outcomes (duration of IV insulin and nil per os (NPO) status, need for medical intensive care unit (ICU) admission, in-hospital mortality, and complications of AP [acute and persistent kidney injury, systemic inflammatory response syndrome, and concurrent infection]).
Statistical analysis
We performed analyses to describe and summarize the distributions of variables. We used the Kolmogorov-Smirnov and Shapiro-Wilk tests to evaluate whether continuous variables were normally distributed. We used Student’s t-test to compare normally distributed continuous variables; we used Wilcoxon’s rank-sum test to compare nonparametric continuous variables; Chi-square test or Fisher’s exact test were used to compare categorical variables. We plotted Loess Curve for trends of serum TG and APACHE II scores over time up to 96 hours after admission.
To more efficiently evaluate our clinical outcomes, we performed a propensity score matched analysis for the comparison between the plasmapheresis and non-plasmapheresis groups. Candidate factors for the propensity match included baseline laboratory values (serum TG and lipase levels), severity of illness (Ranson’s Criteria, APACHE II score), age, gender, co-morbidities, and substance use; we matched plasmapheresis and non-plasmapheresis patients in a 1:1 ratio using the Nearest Neighbor Method [27]. To ensure a successful match, we compared characteristics between the two groups using Wilcoxon’s signed rank test. The effect of plasmapheresis on primary outcome was then evaluated using mixed effects linear regression models, with the pair-matched clusters entered as a random effect. All statistical analyses were performed using STATA (Version 14.0). We considered P-values of ≤ 0.05 as statistically significant.
Cohort characteristics
We identified 142 patients who had a confirmed diagnosis of HTGAP (Table 1). The majority were male (107; 75.3%); the mean age was 39 (range 20 to 63) years. All patients received standard treatments with pancreatic rest, fluid resuscitation, and subcutaneous or IV insulin, fifteen patients (10.6%) underwent plasmapheresis based on physician judgment and patient consent, while 127 patients (89.4%) received only conservative management without plasmapheresis. No significant differences existed between groups regarding age and gender distribution, past medical history or substance use history.
| Variables | Plasmapheresis (N=15) |
No-plasmapheresis (N=127) |
|||
|---|---|---|---|---|---|
| Epidemiology Variables | Mean/N | SD/% | Mean/N | SD/% | **P-value |
| †Age, years mean (SD) | 42.1 | (-10.2) | 39.4 | (9.7) | 0.32 |
| *Male gender | 12 | 80 | 95 | 74.8 | 0.31 |
| *Past Medical History | |||||
| Diabetes Mellitus | 9 | 60.0 | 59 | 46.5 | 0.32 |
| Hypertension | 7 | 46.7 | 42 | 33.1 | 0.29 |
| Hyperlipidemia | 7 | 46.7 | 54 | 42.4 | 0.76 |
| Metabolic syndrome | 4 | 26.7 | 23 | 18.1 | 0.42 |
| *Substance abuse | |||||
| Tobacco | 6 | 40 | 39 | 30.1 | 0.47 |
| EtOH | 4 | 26.7 | 45 | 362 | 0.46 |
| Clinical Severity Variables | |||||
| †Laboratory values | |||||
| Lipase (Unit/L) | 1167 | 1602 | 1181 | 2378 | 0.9 |
| TG (mg/dl) | 7193 | 2812 | 3511 | 2465 | <0.01 |
| †Severity of AP | |||||
| APACHE II score | 11.4 | 4.3 | 9.1 | 5.6 | 0.06 |
| Ranson's Criteria | 3.73 | 1.98 | 3.07 | 1.69 | 0.08 |
Abbreviations: N, number; SD, standard deviation; EtOH, alcohol;
†Normally distributed continuous variable. Presented as mean value and standard deviation.
*Categorical variables. Presented as number and percentage of patients.
** P-value obtained with Student's t test for continuous values, Chi-square test or Fisher’s exact test for categorical variables.
Table 1: Characteristics of patients with hypertriglyceridemia-induced acute pancreatitis by whether plasmapheresis was initiated, John H. Stroger Hospital of Cook County.
Before the propensity match, compared to the non-plasmapheresis group, the plasmapheresis group had higher baseline serum TG levels 7193 vs. 3511 mg/dl, (p<0.01); and a trend toward higher mean APACHE II scores, 11.4 vs. 9.1 (p=0.06) and Ranson’s Criteria score 3.73 vs. 3.03 (p=0.08).
Description of plasmapheresis group
Among the fifteen patients who received plasmapheresis, the mean serum TG level on admission was 7193 mg/dl (range 3221 to 12806 mg/dl). The average baseline APACHE II score was 11.4 (SD=4.3). The documented reason for initiating plasmapheresis included severe HTG (n=6), severe acute pancreatitis (n=3), and delayed response to conservative management (n=6). The average timespan from presentation to emergency department to first plasmapheresis session was 43 hours (range 16 to 84 hours). Ten patients (66.7%) required only one session of plasmapheresis while five patients (33.3%) had two plasmapheresis sessions, one each day for two consecutive days. Average serum TG level decreased from 5573.8 mg/dl (SD=4.9) days. One patient (6.7%) had recurrent AP 173 days post discharge (Table 2).
| Age /Gender |
TPE reason | Timing (hours) |
Sessions | Lipase (u/l) |
APACHE II score |
TG pre-TPE (mg/dl) |
TG post-TPE (mg/dl) |
LOS (days) |
|---|---|---|---|---|---|---|---|---|
| 57/ M | HTG | 32 | 2 | 1611 | 13 | 7102 | 994 | 8 |
| 50/M | HTG | 22 | 2 | 247 | 7 | 8600 | 802 | 4 |
| 36/M | Severe AP | 37 | 1 | 2457 | 12 | 6177 | 950 | 13 |
| 33/M | Severe AP | 48 | 1 | 436 | 11 | 2889 | 188 | 16 |
| 28/F | DI | 84 | 1 | 229 | 5 | 1464 | 710 | 10 |
| 57/ M | DI | 26 | 2 | 1832 | 18 | 3210 | 749 | 22 |
| 42/M | DI | 25 | 1 | 244 | 9 | 12806 | 620 | 11 |
| 45/M | DI | 84 | 1 | 872 | 11 | 1849 | 527 | 14 |
| 40/M | HTG | 78 | 1 | 527 | 7 | 1915 | 745 | 5 |
| 40/F | DI | 66 | 2 | 149 | 12 | 9396 | 929 | 12 |
| 50/M | DI | 22 | 2 | 446 | 18 | 9306 | 338 | 11 |
| 41/M | HTG | 29 | 1 | 849 | 12 | 1772 | 238 | 5 |
| 53/M | Severe AP | 48 | 1 | 6412 | 19 | 1939 | 634 | *N/A |
| 24/F | HTG | 16 | 1 | 214 | 12 | 11194 | 1710 | 7 |
| 37/M | HTG | 24 | 1 | 980 | 6 | 3988 | 246 | 7 |
Abbreviations: M, male; F, female; TG, triglyceride; APACHE, acute physiology and chronic health evaluation; TPE, plasmapheresis;
LOS, length of stay; HTG, severe hypertriglyceridemia; DI, delayed improvement on conservative treatment; AP, acute pancreatitis;
N/A, non-applicable;
* Not applicable due to in-hospital mortality.
Table 2: Description of patients (N=15) who received plasmapheresis for hypertriglyceridemia pancreatitis.
Propensity match
Before the propensity-match, the two groups (plasmapheresis and non-plasmapheresis) patients differed in their baseline TG levels, APACHE II (P=0.06) and Ranson’s criteria scores (p=0.08). non- pairs; these differences were resolved by the matching process (Table 3). To further explore possible clinical differences between the two groups, we evaluated the clinical trajectory of patients in both groups from the time of admission to the time preceding initiation of plasmapheresis— we temporally matched the non-plasmapheresis group. The plasmapheresis group had a slower decline in their TG levels and a non-significant trend toward a worse APACHE II score (Figure 1). Suggesting that despite successful propensity matching for admission characteristics, the plasmapheresis patients were not improving as rapidly in biochemical or possibly physiologic indices.
| Variables | Plasmapheresis (N=15) |
Pre-Match Non-plasmapheresis (N=127) |
Post-Match Non-plasmapheresis (N=15) |
|||||
|---|---|---|---|---|---|---|---|---|
| Clinical Severity Variables | Mean/N | SD/% | Mean/N | SD/% | **P-value | Mean/N | SD/% | ††P-value |
| †Laboratory values | ||||||||
| Lipase (Unit/L) | 1167 | 1602 | 1181 | 2378 | 0.9 | 781 | 634 | 0.39 |
| TG (mg/dl) | 7193 | 2812 | 3511 | 2465 | <0.01 | 7411 | 3385 | 0.85 |
| †Severity of AP | ||||||||
| APACHE II score | 11.4 | 4.3 | 9.1 | 5.6 | 0.06 | 11.4 | 5.7 | 1.00 |
| Ranson's Criteria | 3.73 | 1.98 | 3.07 | 1.69 | 0.08 | 3.7 | 2.0 | 0.93 |
| Clinical Outcomes Variables | ||||||||
| Hospitalization course | ||||||||
| †Length of stay (days) | 10.3 | 4.9 | 6.9 | 4.9 | <0.01 | 7.7 | 3.2 | 0.12 |
| †Length of IV insulin (days) | 4.7 | 2.5 | §3.9 | 1.5 | 0.32 | §4.7 | 1.4 | 0.5 |
| †Length of NPO (days) | 5.1 | 3.2 | 3.9 | 3.4 | 0.04 | 4.1 | 1.5 | 0.77 |
| *Require MICU admission | 15 | 100.0 | 49 | 38.6 | <0.01 | 9 | 60.0 | 0.02 |
| *In-hospital mortality | 1 | 6.7 | 4 | 3.2 | 0.43 | 0 | 0.0 | 0.50 |
| *Complications of AP | ||||||||
| SIRS | 6 | 40.0 | 70 | 55.1 | 0.27 | 8 | 53.3 | 0.72 |
| Concurrent infection | 3 | 20.0 | 33 | 25.9 | 0.61 | 5 | 33.3 | 0.68 |
| AKI upon admission | 8 | 53.3 | 59 | 46.5 | 0.61 | 10 | 66.7 | 0.71 |
| Persisted AKI at 48hours | 4 | 26.7 | 10 | 7.9 | 0.02 | 1 | 6.7 | 0.33 |
| *Re-admission for AP | 2 | 14.3 | 23 | 18.4 | 0.7 | 1 | 6.7 | 0.60 |
Abbreviations: TG, triglyceride; APACHE, acute physiology and chronic health evaluation; MICU, medical intensive care unit; IV, intravenous; NPO, nil per os; AP, acute pancreatitis; SIRS, systemic inflammatory response syndrome; AKI, acute kidney injury; mean, mean value; n, number; SD, standard deviations;
*Categorical variables. Presented as number and percentage of patients.
†Continuous variables. Presented as mean value and standard deviations.
§Based on patients who received intravenous insulin and were successfully switched to subcutaneous insulin.
**P values obtained with Student’s t test for parametrical continuous variables; rank sum test for non-parametrical continuous
variables; Chi-square test or Fisher’s exact test for categorical variables.
††P values obtained with Wilcoxon signed rank test for continuous variables; Chi-square test or Fisher’s exact test for categorical
variables.
Table 3: Pre-math and post-match comparison between plasmapheresis and non-plasmapheresis group.
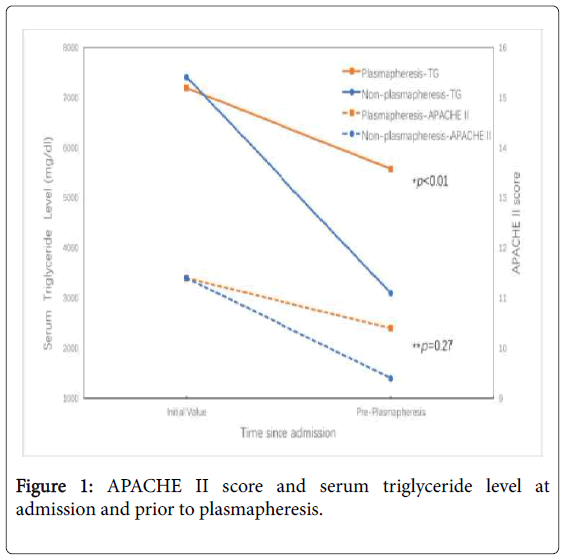
Figure 1: APACHE II score and serum triglyceride level at admission and prior to plasmapheresis.
Clinical outcomes
Before propensity matching, the non-plasmapheresis patients had shorter lengths of stay and duration of IV insulin, and were less likely to be admitted to the medical ICU or have persistent acute kidney injury (Table 3). After propensity matching, the only different clinical outcome was that the non-plasmapheresis patients were less likely to be admitted to the medical ICU. When we plotted the trend in mean serum TG level from admission (Day 0) and to Day 4, we found that HTG resolved at Day 4 for both groups, even though the plasmapheresis group had a slower decline in TGs before plasmapheresis (Figure 2). Similarly, the daily average APACHE II score for the two groups were identical on Days 1 and 4; however, the plasmapheresis group had a non-significant trend toward higher APACHE II scores on Days 2 and 3 (Figure 3). There were no statistically significant differences regarding in-hospital mortality, complications of AP, or rate of re-admission for AP during an average follow-up of 893 days.
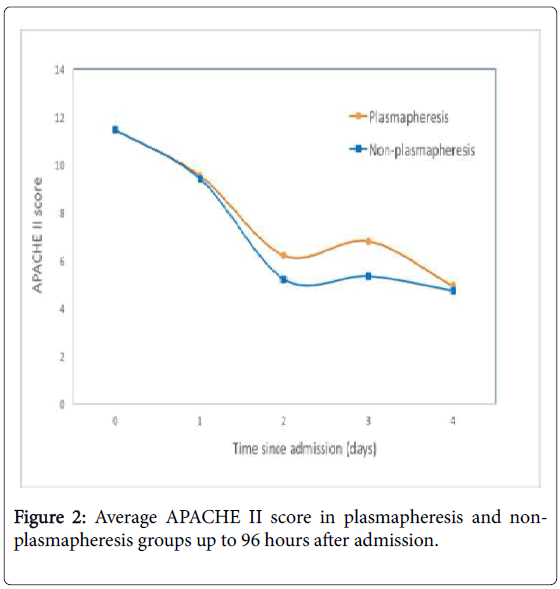
Figure 2: Average APACHE II score in plasmapheresis and nonplasmapheresis groups up to 96 hours after admission.
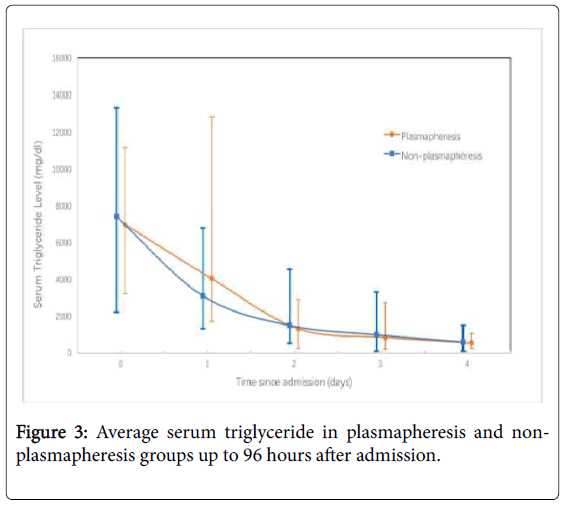
Figure 3: Average serum triglyceride in plasmapheresis and nonplasmapheresis groups up to 96 hours after admission.
In post-match analyses, by mixed effect linear regression, plasmapheresis did not increase LOS with statistical significance (95% Confidence Interval: -0.60, 5.14). Similarly, there were no differences in length of ICU stay (for those who required ICU admission), length of NPO, in-hospital mortality, complications of AP or rate of readmission for AP (Table 3). The plasmapheresis group still was more likely to be admitted to the medical ICU, 100% vs. 60% in the nonplasmapheresis group (p=0.02), likely because initiation of plasmapheresis required admission to the medical ICU.
From our entire cohort, we found that patients who underwent plasmapheresis had higher TG levels on admission, and had a trend toward more severe AP. The unmatched cohort also revealed that the plasmapheresis group had longer LOS, required more IV insulin, and had a longer duration of NPO status. However, after performing a successful propensity-score match, we were better able to make inferences about the effectiveness of plasmapheresis. From the matched cohort, we found that despite similar baseline characteristics, plasmapheresis had no effect (neither beneficial nor deleterious) on clinical outcomes.
Plasmapheresis was first described by Betteridge et al. in 1978 for management of HTG-AP, and since then was reported in numerous cases reports/series as an effective treatment method [16-21,28]. In their systematic review, Click et al. reviewed 301 unique patients with HTG-AP who underwent plasmapheresis from 74 case reports/series, and concluded that plasmapheresis is highly effective in reducing serum triglyceride levels and improving symptoms [29]. However, due to heterogeneity in reported criteria of severity of AP, uncontrolled nature of data and lack of comparison groups, it is difficult to make strong recommendations on the role of plasmapheresis in HTG-AP [29]. Afari et al. compared 3 cases of HTG-AP treated with plasmapheresis and 11 cases managed conservatively; they concluded that plasmapheresis effectively reduced serum TG levels but was associated with longer hospital stays [30]. Similarly, in their retrospective study of 10 patients with HTG-AP during pregnancy among which 5 underwent plasmapheresis, Huang et al. concluded that plasmapheresis reduces serum TG levels significantly and shortens hospital stay [31]. Chen et al. directly compared 20 patients who underwent plasmapheresis to 40 who did not and found that plasmapheresis didn’t change mortality or complications [32]. The small sample sizes and lack of similar control groups in regards to presenting serum TG levels and severity of AP complicate clinical decision making based on these studies.
Similar to previous studies, when viewed as a case series, plasmapheresis appeared to dramatically reduce TG levels when assessed using pre- and post-intervention values. After propensity matching however, the non-plasmapheresis groups had similar decreases in the TG level despite having comparable baseline levels. After propensity score matching, plasmapheresis had no effect on the following additional clinical parameters: LOS, duration of time as NPO, duration of IV insulin, in-hospital mortality, and rate of readmission for AP. Complications of AP, including systemic inflammatory response syndrome (SIRS), concurrent infection, transient and persistent acute kidney injury (AKI) also were no different between groups.
Before concluding that plasmapheresis did not appear to be beneficial, we further explored the success of our propensity-score match on the trajectory of patients’ condition before they received plasmapheresis. By evaluating the longitudinal clinical course in our patients, we found that the plasmapheresis group was not responding as quickly to conservative measures. Despite a seemingly successful match, some residual confounding likely remained [33]. The similarity in various end-points after plasmapheresis may indicate that there were some beneficial effects from plasmapheresis; this group of patients “caught up” to the non-plasmapheresis group as measured by improved TG levels and APACHE II scores. As all plasmapheresis were conducted in ICU setting, patients in plasmapheresis group universally required medical ICU admission, while only 60% patients in nonplasmapheresis group required ICU admission. However, this difference likely reflects hospital protocol (i.e., initiation of plasmapheresis requires an ICU admission) instead of objective differences in clinical outcomes.
Currently no clear guideline exists regarding for which patient plasmapheresis should be initiated. It is suggested that for patients with severe AP, severe or very severe HTG, and/or delayed response to conservative management, plasmapheresis may provide benefit [6]. In our post-match comparison, there was no clear clinical benefit from plasmapheresis; however, by observing a slower clinical improvement in the plasmapheresis group, which might have prompted the initiation of plasmapheresis before their intervention, the benefit may have been obscured. This comparison also demonstrated that HTG-AP is a dynamic process with significantly different individual response to therapy; thus, during the acute phase, close monitoring of clinical status and frequent evaluations of the effects of optimized conservative measures are necessary.
Several limitations exist for the present study. As mentioned above, even after an apparently successful propensity score match, there may have been residual confounding in the slower resolution of HTG in the plasmapheresis group before intervention. This counterintuitive finding demonstrated the inadequacy of matching only based on clinical severity upon initial presentation, and suggested the existence of confounding effects of individual response to therapy which was not measurable with retrospective study design. Our study was also limited in that it is from a single center and inclusive of a relatively small number of patients who underwent plasmapheresis; thus, it was potentially underpowered to detect real differences between groups.
In conclusion, we present the first retrospective cohort study evaluating plasmapheresis as a treatment method the treatment of HTG-AP using propensity score matching to adjust for baseline characteristics. Although plasmapheresis had no readily apparent benefit or harm to patients, there likely was residual confounding based on the different clinical trajectories between the plasmapheresis and non-plasmapheresis groups. Our findings provide justification for either the use of a randomized controlled trial, or a larger multicenter observational study taking into consideration the clinical trajectory of patients to further evaluate the role of plasmapheresis in HTG-AP.