Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2016) Volume 6, Issue 3
Introduction: Although quality of care has become a central aspect of modern medicine, a definite relationship between quality indicators (QIs) and outcomes has not been fully established in patients with pancreatic cancer (PC). The primary aim of this study was to examine the possible association of established process-based QIs with short and long term outcomes in patients undergoing PC resection.
Methods: All adult patients undergoing resection for PC in Nova Scotia between 2001 and 2011 were included in a retrospective cohort study. Logistic and Cox model regression analyses were used to test the hypothesis that meeting selected QIs was associated with improved perioperative morbidity, mortality and overall survival.
Results: Pancreaticoduoedenectomy was performed in 82 (87%) patients and distal pancreatectomy in 12 patients (13%). Multivariable analysis adjusting for patient and tumour characteristics showed that only preoperative radiological staging obtained within 8 weeks from the date of surgery was associated with better survival (HR for death=0.34, 95% CI=0.14-0.84). Other QIs failed to show any association with perioperative morbidity and mortality and overall survival.
Conclusions: With the exception of preoperative staging within the recommended time interval, meeting QIs was not associated with improved short and long term outcome in resected PC patients.
<with aggressive biology and poor prognosis [1,2]. Except for surgery, other treatments have shown modest impact on patients’ survival and are often underutilized [3-9]. Since there are no cost-effective screening tests, a high clinical suspicion is necessary for the diagnosis of early stage tumors2 and the majority of patients are diagnosed with locally advanced or metastatic disease [2,3].
Recent studies have shown that survival of patients with PC has remained rather unchanged over the last decades with only 5-10% being alive after five years [4,10,11]. Besides established prognostic factors such as cellular differentiation, lymph vascular infiltration and tumor stage, there may be other reasons responsible for the low survival rate of these patients. Several groups have reported that PC patients receive one of the lowest rates of cancer-directed therapy among all the solid tumors [4-10] and treatments may differ based upon patients’ socioeconomic status (education level, income), place of residence (rural vs. urban), number of procedures performed in a health system (low vs. high volume hospital) and physician expertise [4-10].
The modern movement for quality improvement in health care has motivated a critical appraisal of the quality of care of PC mainly because survival remains disappointing. This has led several investigators to identify indicators and standards that are unique to this disease. Current quality indicators (QIs) for patients undergoing resection are consensus-based, and some degree of uncertainty remains about the association between these QIs and outcomes. The primary objective of this study was to test the hypothesis that surgical patients who met established QIs for PC had better peri-operative outcomes and or long-term survival after adjusting for co-morbidities and tumor characteristics. To the best of our knowledge, no other studies have tested this hypothesis except for investigations on the relationship between volume of pancreatic resections and outcomes.
This population-based cohort study included all patients older than 18 who had undergone resection for primary exocrine pancreatic cancers (PC) over a ten year period (April 1, 2001-March 31, 2011) in the province of Nova Scotia, Canada.
Patients with PC were identified based on diagnostic codes of the International Classification of Disease for Oncology, 3rd edition (ICD-O-3) using the Nova Scotia Cancer Registry (NSCR), a prospectively maintained provincial registry of all patients affected by malignant diseases. Diagnostic codes of malignancies of the exocrine pancreas used for this study are summarized in Table 1. Patients were excluded if younger than 18, with pancreatic endocrine neoplasms, lymphomas, sarcomas, distant metastatic disease from other malignancies or direct invasion of tumors originating in surrounding organs (retroperitoneum, gastrointestinal tract).
| ICD Codes Used for Identification of Location of Pancreatic Tumors | ICD-9-CM | ICD-10-CM |
|---|---|---|
| Malignant neoplasm of head of pancreas | 157 | C25.0 |
| Malignant neoplasm of the body of pancreas | 157.1 | C25.1 |
| Malignant neoplasm of the tail of pancreas | 157.2 | C25.2 |
| Malignant neoplasm of the pancreatic duct | 157.3 | C25.3 |
| Malignant neoplasm of other specified sites of pancreas | 157.8 | C25.7 |
| Malignant neoplasm of pancreas part unspecified | 157.9 | C25.9 |
| ICD Codes Used for Identification of Tumors Origination from Exocrine Pancreatic Cells: Neoplasm Malignant; Tumor Cells Malignant Carcinoma NOS; Undifferentiated Carcinoma; Anaplastic Carcinoma; Pleomorphic Carcinoma; Papillary Carcinoma; Papillary Squamous Cell Carcinoma; Adenocarcinoma NOS; Diffuse Adenocarcinoma; Solid Carcinoma NOS; Mucocarcinoid; Adenocarcinoid; Atypical Carcinoid Tumor; Adenocarcinoma with Mixed subtypes; Papillary Adenocarcinoma NOS; Cystoadenocarcinoma NOS; Serous Cystoadenocarcinoma; Solid Pseudopapillary Carcinoma; Intraductal Papillary Mucinous Carcinoma; Mucinous Cystadenocarcinoma NOS; Mucinous Carcinoma/Adenocarcinoma; Mucin Producing Carcinoma/Adenocarcinoma; Duct Adenocarcinoma; Acinic Cell Adenocarcinoma; Acinar Cell Cystoadenocarcinoma; Adenosquamous Carcinoma; Adenocarcinoma Neuroendocrine DifferentaionPancreatoblastoma; Carcinoma NOS | ICD-O-3 Histology Codes 8000, 8001, 8002, 8003, 8010, 8011, 8012, 8020, 8021, 8022, 8030, 8031, 8032, 8033, 8034, 8035, 8050, 8052, 8140, 8141, 8142, 8143, 8144, 8145, 8146, 8147, 8230, 8243, 8245, 8249, 8255, 8260, 8261, 8262, 8263, 8310, 8323, 8440, 8441, 8452, 8453, 8470, 8472, 8473, 8480, 8481, 8490, 8500, 8501, 8502, 8503, 8510, 8550, 8551, 8560, 8570, 8571, 8572, 8573, 8574, 8575, 8576, 8971, 8980. | |
| ICD Codes Used for Identification of Tumors Origination from Endocrine Pancreatic Cells | ICD-O-3 Histology Codes | |
| Islet Cell Carcinoma Beta-Cell Tumor: Malignant Alpha-Cell Tumor: Malignant Vipoma G-Cell Tumor: Somatostatinoma: MaligantEnteroglucagonoma: Malignant Bile Duct Adenocarcinoma Bile Duct Cystoadenocarcinoma Carcinoid Tumor Argentafin Carcinoma Tumor Enterochromaffin Cell Tumor Neuroendocrine Carcinoma Insular Carcinoma | 8150, 8151, 8152, 8155, 8153, 8156, 8157, 8160, 8161, 8240, 8241, 8242, 8246, 8337 | |
Table 1: Summary of all the International Statistical Classification of Diseases and Related Health Problems (ICD) codes used to identify patients with pancreatic adenocarcinoma included in this study.
Each patient who satisfied the inclusion criteria was assigned a unique study identification (ID) number to protect patients’ privacy. Additional administrative datasets were linked to the NSCR for completion of sociodemographic and clinical data pertinent to this study as represented in Figure 1. Linked datasets included the Oncology Patient Information System (OPIS), Medical Service Insurance (MSI) Physician Services, Medical Service Insurance (MSI) Patient Registry, and the Canadian Institutes of Health Information (CIHI) Discharge Abstract Database (DAD) [11]. These datasets were linked to the NSCR by the Population Health Research Unit (PHRU) at Dalhousie University. The methodology used to link these administrative datasets has been described in details in previous manuscripts published by our group [12-15]. Using DAD, patients who underwent surgery were identified using ICD-9/10 procedure codes. Surgical patients were excluded if they underwent palliative interventions such as biliary or gastric bypasses when found to be unresectable intraoperatively.
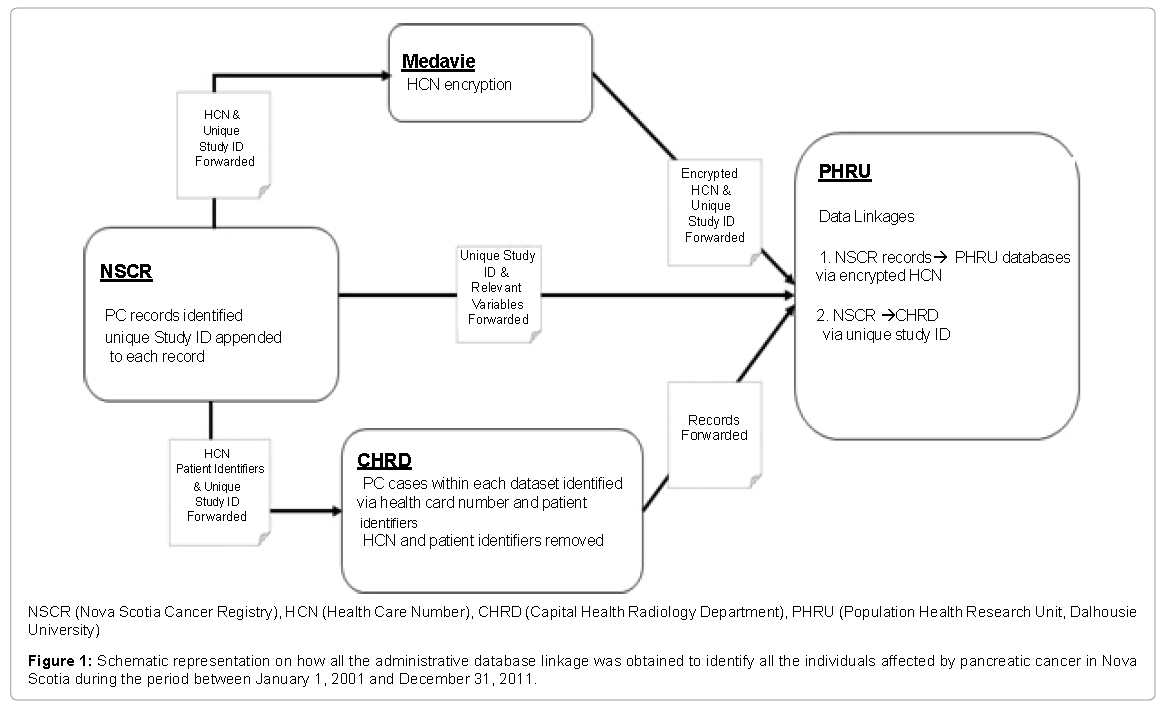
Figure 1: Schematic representation on how all the administrative database linkage was obtained to identify all the individuals affected by pancreatic cancer in Nova Scotia during the period between January 1, 2001 and December 31, 2011.
Administrative databases utilized in this study were unable to provide all the clinical variables required to test the validity of the primary and secondary hypotheses of this study. Therefore, medical records of included patients were reviewed by the principal author (SH) who appraised the pertinent documents and extracted necessary data that were subsequently entered into the digital database used for all statistical analyses.
Approval for this study was obtained from all the ethic review boards (ERB) at each health district where patients received their treatment in the province of Nova Scotia and the investigators ensured adherence to confidentiality and safe storage of patients’ information.
Clinico-demographic characteristics: Variables of interest for the primary and secondary outcomes were patients’ sociodemographic characteristics, tumour characteristics, types of surgical treatments, perioperative adverse events and mortality within 90 days after surgery and overall 5-year survival. Sociodemographic variables included patients’ age, sex, Elixhauser comorbidity index [16], patients’ residential status (urban vs. rural) and the median income estimated using data associated with the health district where patients resided at the time of diagnosis (Individual Tax Statistics by Area (ITSA) (Tax Year 2010) [12]. The Elixhauser Comorbidity Index categorizes comorbidities of patients based on the International Classification of Diseases (ICD) diagnosis codes found in administrative data and it has been used in epidemiological studies to predict hospital resource utilization and in-hospital mortality. Each comorbidity category was categorized in present or absent. For patients with closely related comorbidities (e.g. diabetes and diabetes with a complication), only the more severe comorbidity was counted [17].
Tumor characteristics: Tumor characteristics included, tumor size (in cm), the lowest grade of cell differentiation, the anatomical location of the tumor within the pancreas (pancreatic tail, body, head), surgical resection margins (no residual disease (R0) vs microscopic residual disease (R1) andmacroscopic residual disease (R2), number of lymph nodes identified in the surgical specimen and number of lymph nodes containing malignant cells [18]. Although consensus regarding the definition of tumor involvement of the resection margins of pancreatic specimens is lacking, at our institution surgical pathologists have used the North America guidelines that define R1 resections the presence of cancer cells at the surface of the resection margin (0 mm rule) [13,14].
Short-term outcomes: Perioperative complications were categorized using the Dindo-Clavien classification [19] and only adverse events of grade III or higher developed within the 30 days or during the same hospital admission were recorded and entered in the multivariable regression model. Dindo-Clavien grade III complications included all adverse events that required surgical, endoscopic or imaging-guided percutaneous interventions. Dindo-Clavien grade IV complications included all life-threatening complication conditioning at least one organ dysfunction or requiring intensive care unit management and Dindo-Clavien grade V complications were recorded as perioperative mortalities within 90 days after surgery.
Long term outcomes: Overall survival was defined as the time interval between the day of surgical therapy and the day when patients expired independently of the primary cause of death. Patients were censored if still alive when the study was closed, or who were lost at follow up. Date of censoring was March 31, 2011 or the date of patient’s last clinic appointment.
Quality indicators: Selection of QIs was performed by using a modified list of QIs proposed by Bilimoria [12] and by Sabater [13]. These QIs were chosen as measures of the quality of care for patients undergoing surgery and were categorized into preoperative (staging and access to surgery), perioperative (intra and postoperative adverse events, R0 resection rate, the number of lymph node retrieved), and post-operative (surgical pathology reporting and referral for adjuvant therapies).
QIs chosen for the preoperative category included the presence or absence of appropriate tumor staging with a high-quality contrast enhanced abdominal computerized tomography (CT) and / or magnetic resonance imaging (MRI) in addition to access to surgical therapy within two months from the time of diagnosis. These radiological modalities determined whether or not the proper workup for resectability and metastatic disease occurred in a timely fashion and if prompt referral to surgical specialists and access to operative rooms took place. QIs chosen for the assessment of surgical interventions included Grade III to V Dindo-Clavien complications as a reflection of the quality of surgical therapy and the rates of R1 or R2 resections as a potential measure of adequacy of surgical resections.
QIs chosen for the assessment of the surgical pathology specimens and their reporting included the presence or absence of appropriate information on tumor staging. Surgical pathology QIs were met when reporting included an accurate description of the number of lymph nodes identified in the specimen [20], presence or absence of the description regarding tumor characteristics such as grade of cellular differentiation, histology, maximum size of the neoplastic mass, total number of lymph nodes containing evidence of malignant cells, presence or absence of tumor along the surgical margins (R0, vs. R1/ R2 resections), presence or absence of lymphovascular or perineural tumor invasion, and the final TNM stage according to American Joint Committee on Cancer (AJCC) Staging Manual [21].
QIs analyzed for the postoperative domain included documentation that patients were referred to and assessed by a medical oncologist and how many were considered for adjuvant chemotherapy unless perioperative complications or pre-existing comorbidities precluded this option [22].
Primary and secondary outcomes
Primary aim of this study was to assess if there was any association between meeting established QIs and perioperative complications and mortality.
Secondary outcome was to assess if there was an association between QIs and overall survival of patients who had undergone surgical therapy after adjusting for patients’ and tumor characteristics.
The sample size of patients was fixed due to the retrospective design of this study. Estimates of central tendency (means, medians) and spread (standard deviation, interquartile range) were used for continuous variables and frequency or percentages for categorical data. Continuous data were compared using t-Test and categorical variables were compared using the Chi-square test with Yates correction or Fisher exact test when appropriate.
Univariate and multivariate Cox regression analyses were performed to test the null hypothesis that QIs were associated with overall survival. Multivariable Cox regression models included preoperative staging imaging within two months (yes vs. no), surgical procedure performed within 2 months from the time of diagnosis (yes vs. no), development of post-operative complications (yes vs. no), retrieval of 10 or more lymph nodes (yes vs. no). Adjustment included patients’ age (>65 years), sex, socioeconomic status and residential status (rural vs. urban), resection margin status (R0 vs. R1/R2), tumour size, the presence of lymphovascular or perineural involvement (yes vs. no), and use of adjuvant therapy (yes vs. no).
Logistic regression analysis was used for univariate and multivariate analyses to test the hypothesis that QIs were predictors for perioperative complications (yes vs. no). In the regression models, selected independent variables included preoperative imaging within 2 months of surgery (yes vs. no), time to surgery within 2 months from diagnosis (yes vs. no), number of lymph nodes resected greater than or equal to 10 (yes vs. no), patients’ age (>65 years), sex, comorbidity score, and tumour size. Interaction terms were not examined due to sample size constraints.
An alpha level of 0.05 was be used to determine statistical significance. Tests of significance were two tailed. The output of the statistical analysis for this paper was generated using SAS software, Version 9 of the SAS System (SAS Institute Inc., Cary, NC, USA) and statistical significance was identified by two-tailed P-values of less than 0.05 and 95% confidence intervals (CI).
A total of 1094 patients were diagnosed with pancreatic or periampullary malignancies during the study period and 162 underwent surgical interventions. Among patients who underwent surgery, 94 met the inclusion criteria and represented the study population.
Socio-demographic and clinical characteristics of the entire cohort are summarized in Table 2. Overall, fulfillment of QIs varied significantly across different domains (Table 3). Perioperative complications (Dindo-Clavien class III and IV) occurred in 19% of patients and preoperative mortality in 5.3%.
| Variable | Total Number of Patients (n=94) |
|---|---|
| Age in years, median (25th, 75th) | 66.1 (59.3, 72.4) |
| Age>65 years, n, (%) | 55 (58.5) |
| Gender, n, (%) | |
| Male | 55 (58.5) |
| Female | 39 (41.4) |
| Elixhauser Comorbidity Index | |
| 0 | 58 (61.7) |
| 1 | 19 (20.2) |
| > | 17 (18.0) |
| Residence Status, n, (%) | |
| Urban | 68 (72.3) |
| Rural | 18 (19.1) |
| Unknown | 8 (8.5) |
| Income Quartile, n, (%) | |
| Q1 (Low) | 19 (20.1) |
| Q2 | 13 (13.8) |
| Q3 | 26 (27.6) |
| Q4 (High) | 33 (35.1) |
| Surgical Therapy, n, (%) | |
| Pancreaticoduodenenctomy | 82 (87.2) |
| Distal Pancreatectomy | 12 (12.7) |
| Dindo-Clavien Classification of Perioperative Adverse Events, n, (%) | |
| Grade 0-I-II | 70 (74.4) |
| Grade III | 13 (13.8) |
| Grade IV | 6 (6.3) |
| Perioperative Mortality, n, (%) | 5 (5.3) |
| Tumor Location, n, (%) | |
| Head | 82 (87.2) |
| Body | 1 (1.1) |
| Tail | 11 (11.7) |
| AJCC T Stage, n, (%) | |
| 1 | 2 (2.1) |
| 2 | 13 (13.8) |
| 3 | 74 (78.7) |
| 4 | 3 (3.2) |
| X | 2 (2.1) |
| AJCCN N Stage, n, (%) | |
| 0 | 34 (36.2) |
| 1 | 58 (61.7) |
| Unknown | 2 (2.1) |
Table 2: Demographic and Clinical Characteristics of the Study Population
| Domain | Quality Indicator | Number and percantage of patients who met established quality indicators |
|---|---|---|
| N (%) | ||
| Preoperative | Preoperative imaging with CT/MRI within 2 months | 77 (81.9) |
| Time from PC diagnosis to first treatment <2 months | 88 (93.6) | |
| Operative | Total lymph nodes examined ≥10 | 31 (33.0) |
| Clavien-Dindo grade III-V Complications | 24 (25.5) | |
| R1 Resection rate | 36 (38.2) | |
| Surgical Pathology | Reported tumour grade | 94 (100) |
| Reported tumour histology | 94 (100) | |
| Reported tumour size | 90 (95.7) | |
| Reported number of lymph nodes assessed for tumor invasion | 93 (98.9) | |
| Reported pancreatic neck resection margins | 90 (95.7) | |
| Reported pancreatic uncinate process resection margins | 46 (48.9) | |
| Reported pancreatic anterior resection margins | 4 (4.3) | |
| Reported pancreatic posterior resection margins | 16 (17.0) | |
| Reported portal vein resection margins | 10 (10.6) | |
| Reported bile duct resection margins | 76 (80.9) | |
| Reported duodenal resection margins | 78 (83.0) | |
| Reported jejunal resection margins | 77 (81.9) | |
| Reported Lymphovascular Invasion or perineural Invasion | 70 (74.5) | |
| Reported TNM stage | 23 (24.5) | |
| Postoperative | Consultation with medical Oncology | 50 (53.2) |
| Documented reason for patients not receiving adjuvant chemotherapy | 43 (45.7) |
Table 3: Summary of the indicators used to measure the quality of care of patient undergoing surgery for pancreatic adenocarcinoma in Nova Scotia (Total number of patients: 94).
At univariate and multivariate logistic regression analyses, characteristics that were significant for increased risk of perioperative complications were age>65 (OR for perioperative complications 4.75; 95% CI 1.32-17.12; P=0.01) and male sex (OR for perioperative complications 3.83; 95% CI 1.14-12.83; P=0.02) (Figures 2A and 2B). A sensitivity analysis with exclusion of patients who experienced perioperative mortality showed no significant differences than when they were included.
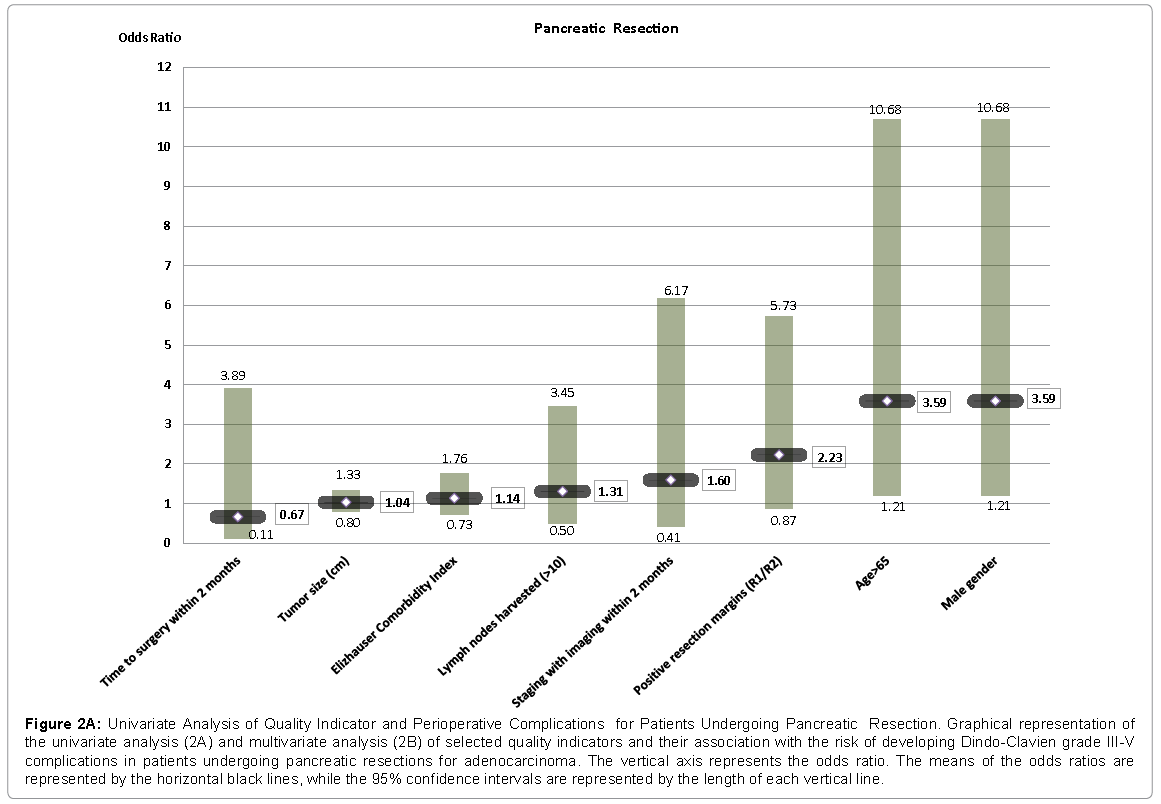
Figure 2a: Univariate Analysis of Quality Indicator and Perioperative Complications for Patients Undergoing Pancreatic Resection. Graphical representation of the univariate analysis (2A) and multivariate analysis (2B) of selected quality indicators and their association with the risk of developing Dindo-Clavien grade III-V complications in patients undergoing pancreatic resections for adenocarcinoma. The vertical axis represents the odds ratio. The means of the odds ratios are represented by the horizontal black lines, while the 95% confidence intervals are represented by the length of each vertical line.
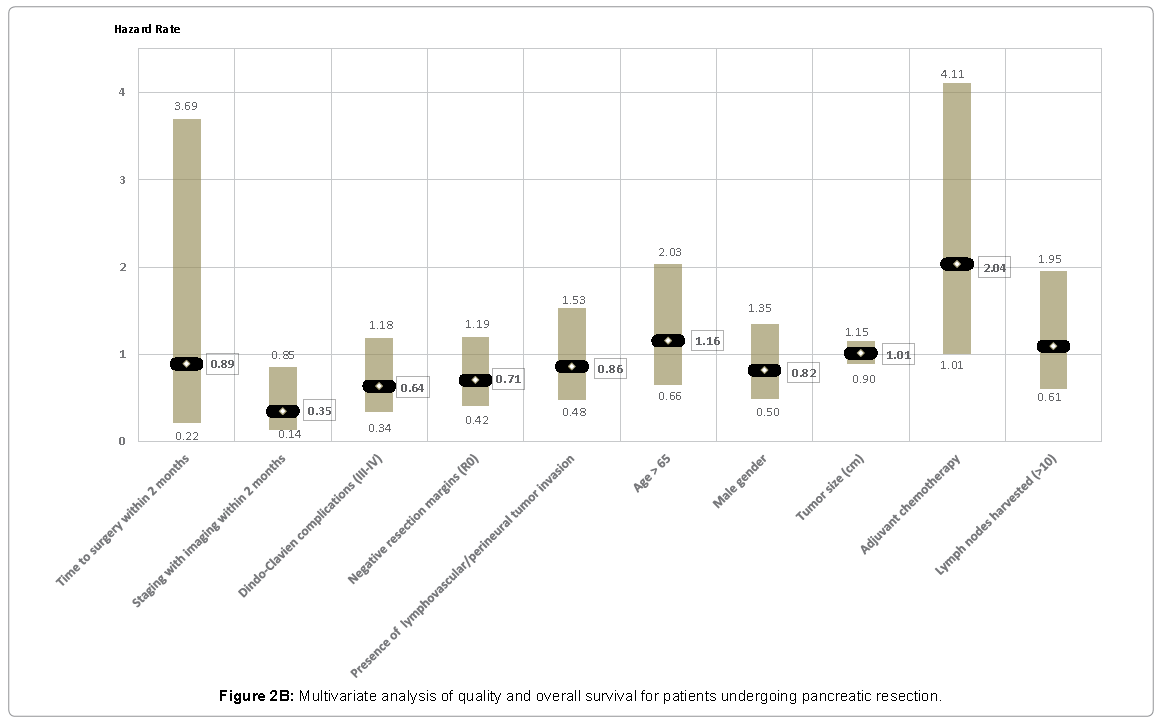
Figure 2b: Multivariate analysis of quality and overall survival for patients undergoing pancreatic resection.
At univariate Cox regression analysis, QIs associated with improved overall survival were appropriate radiological staging within 2 months before surgery (HR for death 0.40; 95% CI 0.21-0.76; P=0.005), lack of major complications (HR for death 0.47; 95% CI 0.28-0.77; P=0.003) and negative resection margins (HR for death 0.58; 95% CI 0.37-0.91; P=0.017).
At multivariate analysis, the only variable that showed statistical significance for overall survival was appropriate preoperative radiological staging within the recommended 2 months (HR for death 0.34; 95% CI 0.14-0.84; P=0.01). On the other hand, administration of adjuvant chemotherapy was found to be associated with lower overall survival (HR for death 2.03; 95% CI 1.00-4.10; P=0.047) (Figures 3A and 3B).
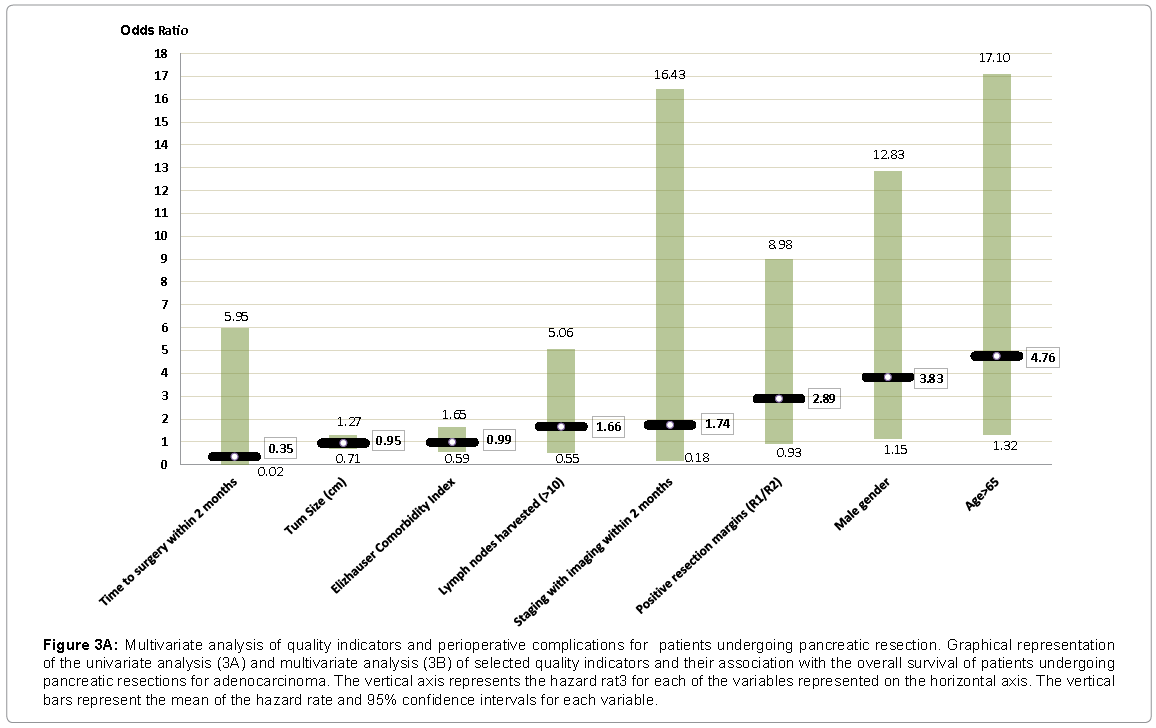
Figure 3a: Multivariate analysis of quality indicators and perioperative complications for patients undergoing pancreatic resection. Graphical representation of the univariate analysis (3A) and multivariate analysis (3B) of selected quality indicators and their association with the overall survival of patients undergoing pancreatic resections for adenocarcinoma. The vertical axis represents the hazard rat3 for each of the variables represented on the horizontal axis. The vertical bars represent the mean of the hazard rate and 95% confidence intervals for each variable.
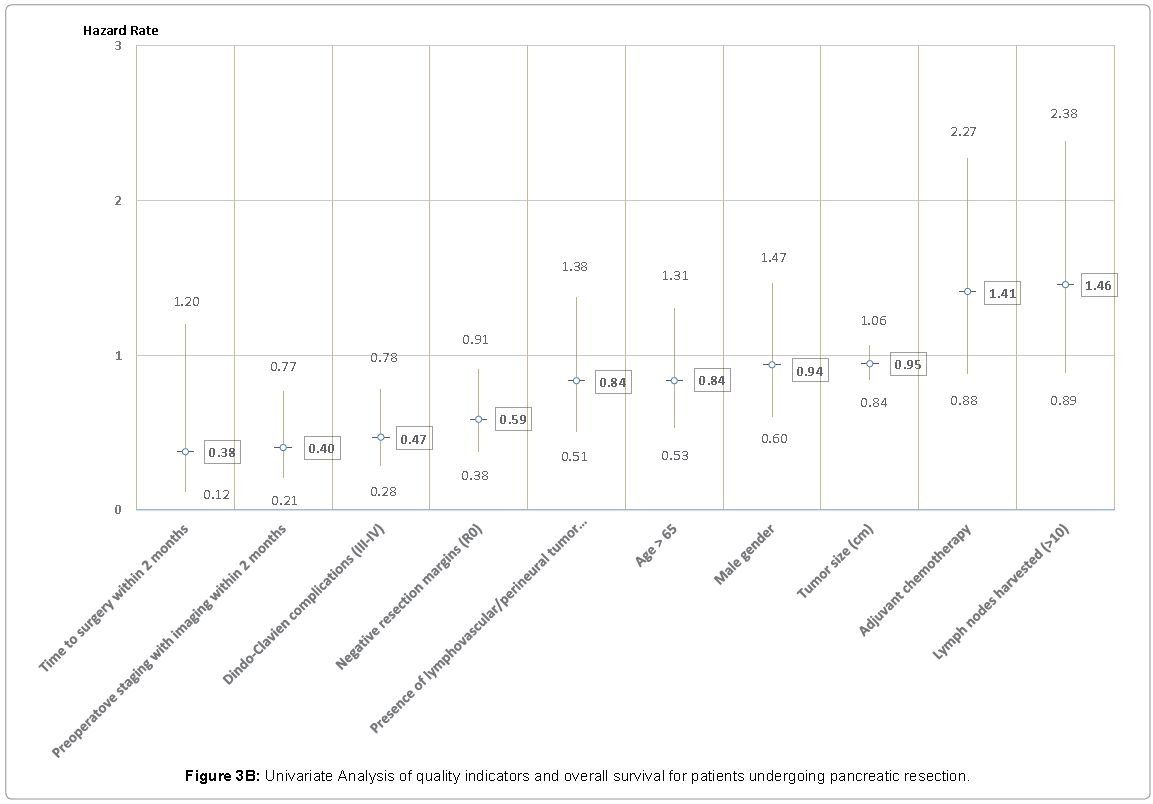
Figure 3b: Univariate Analysis of quality indicators and overall survival for patients undergoing pancreatic resection.
In our study, we found that meeting pre-selected QIs for PC was not associated with improved perioperative outcomes after adjusting for patients’ and tumors’ characteristics. Also, we found that crosssectional imaging tests within 2 months from the date of surgery was the only QI associated with improved overall survival. These negative findings, however, should be interpreted cautiously. First of all because the number of patients enrolled might have been insufficient to test the primary hypothesis (type II error) and future studies with larger sample size are necessary. Second, it is important to keep in mind that the suboptimal quality of the surgical pathology reports of tumor invasion of all resection margins might have been responsible for some of these tumors to be understaged.
In 2014, Statistic Canada reported that in Nova Scotia, 5-year overall survival of PC patients was 4.7% in comparison to the national rate of 9.1%. These results might have been the consequence that, contrary to other Canadian provinces, in Nova Scotia a formal and coordinated quality improvement intervention for PC has never occurred. Hurton [11] raised the possibility that different socio-demographic characteristics of patients living in Nova Scotia could explain those findings [23-26]. Another explanation is that suboptimal care of PC patients treated in Nova Scotia manifested in their inferior survival.
Although this study was primarily designed to assess if established QI for PC surgery were associated with perioperative outcomes and survival, by testing this hypothesis we found that in Nova Scotia, many established QIs for PC were not met. In fact, approximately 18% of patients underwent surgical therapy with radiological tests older than 2 months and 6% of patients waited longer than eight weeks for their surgeries. Nevertheless, despite the long waiting times, the rate of resection with positive margins (R1/R2) in our study was 38% similar to others recent studies [15].
The status of the resection margins depends not only on the way surgical resections are performed, but also on whether the pathologists complete a thorough review of the specimen. For these reasons, both the College of American Pathologists and the Royal College of Pathologists of Canada have put forth recommendations on how the pathological examinations of a pancreatic resections should be performed to reduce the variability of reporting [27]. These recommendations have been implemented in our centre only during the last three years. Consequently, it is possible that the true rate of positive resection margins in our population was higher because in the early years of this study pathologists were not following any particular protocol and might have missed cancer cells along the resection margins of some of the included patients.
Due to the lack of synoptic reports, we also found that the overall quality of the description of the surgical pathology findings was suboptimal with 52% missing data on the state of the uncinate process margin, 96% failing to report data on the anterior margins, 83% missed any description of the posterior margins and 90% lacking data on of the portal vein margins. Conversely, margins with lower risk for tumor invasion were described appropriately more frequently: bile duct edges were properly reported in 81% of cases and duodenal and jejunal margins in 83% and 82% respectively. Similarly to the state of the resection margins, adequate lymph node harvesting and/ or pathological reporting (>10 LN) and complete TNM descriptions occurred only in the minority of patients (33% and 24% respectively) with the description of lymphovascular tumor invasion missing in 25% of the reports.
The quality of pathology reports might have influenced adjuvant treatments. In fact, patients with surgical pathology reports that did not mention positive resection margins or lymph node involvement were rarely referred to medical oncologists after their surgeries. The main reason was that in our institution, referral patterns, and medical oncological therapies were not unified and some providers perceived that there was no benefit for postoperative chemotherapy except for patients at high risk of recurrence (e.g. positive resection margins or positive lymph node involvement). Although this approach has changed, we found that in our cohort chemotherapy was a negative predictor of overall survival at multivariate analysis due to selection bias.
We feel that the main limitation of this study was the inadequate number of patients and the low quality of surgical pathology reporting. The incidence of PC in Canada is 8-10 per 100,000 inhabitants [11]. Therefore, when we designed this study, we estimated that about 70-80 patients are diagnosed with PC every year considering that the population of Nova Scotia has been overall stable and approximately 940,000 inhabitants. We also assumed that 15-20% of these patients would have undergone surgery leading us to expect about 120-160 eligible individuals. Contrary to these estimates, the final number of patients was only 94. Several factors were responsible for this small number. The main one was that the resection rate of PC in Nova Scotia was only 14% as the vast majority of patients was diagnosed late or had co-morbidities that precluded surgery. Additionally,13 medical records were lost while the province transitioned from paper to digital health personal records.
Despite these weaknesses, our study is original since it is the first to investigate potential relationships between QIs and outcomes after PC surgey in a single healthcare payer system. Overall, this is a negative study except for the fact that adequate preoperative imaging tests obtained within two months before surgery appear to be associated with better overall survival. One can speculate that patients who underwent preoperative cross-sectional imaging studies within the recommended period of time had a lower risk of occult metastases. Another possibility is that adequate radiological staging was a proxy for better access to health care services in our region.
In conclusion, to the best of our knowledge, this is the first study to analyze possible associations between QIs and short and long-term outcomes of patients undergoing surgery for PC. Except for appropriate pre-operative radiological staging within two months from the date of surgery, meeting other QIs did not appear to be associated with better outcomes after adjusting for patients’ and tumor factors. These negative findings might be due to the small sample size of patients who were enrolled and understaging of their tumors. Because of the increasing emphasis on the quality of care delivered to patients with PC, we feel that it is important that future studies will be carried out on a much larger population and with standardized reporting systems to reduce the risk of type II statistical errors and misclassification of tumor staging.