Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2013) Volume 3, Issue 2
Based on the example of a cohort of patients treated at a regional Australian hospital, it is evident that many incident acute pancreatitis cases merit consideration as a chronic disease process, for a number of reasons:
• A considerable proportion of acute cases harbour underlying pancreatitis.
• An attack of severe acute pancreatitis may lead to long-term structural or functional impairment.
• Following an attack of acute pancreatitis, risk factors or precursors of chronic pancreatitis or recurrent acute pancreatitis may persist. As such, it is argued that cases of acute pancreatitis should by default be managed from the perspective of a chronic disease paradigm. A management strategy based on a prevention hierarchy is proposed.
Keywords: Acute pancreatitis; Chronic disease; Chronic pancreatitis; Severe acute pancreatitis
AP: Acute Pancreatitis; CI: Confidence Interval; CP: Chronic Pancreatitis; [FE-1]: Faecal elastase-1 concentration; FNQ: Far North Queensland; NHPAC: National Health Priority Action Council; SAP: Severe Acute Pancreatitis
Is acute pancreatitis necessarily an acute disease?
Chronic disease has various possible definitions in the literature, mostly relating to duration of symptoms [1]. In the clinical setting a number of characteristics clearly distinguish it from the acute disease event. The Dictionary of Health Services Management [2] states that chronic diseases have one or more of the following characteristics: they are permanent, leave residual disability, are caused by nonreversible pathological alteration, require special training of the patient for rehabilitation, or may be expected to require a long period of supervision, observation, or care. According to the Australian National Health Priority Action Council, [3] a chronic disease is one that:
• has complex and multiple causes;
• usually has a gradual onset, although acute phases may also occur;
• occurs across the life cycle, but prevalence typically increases with age;
• may compromise quality of life through physical limitations and disability;
• is long-term and persistent, resulting in gradual deterioration of health; and
• is not immediately life-threatening but often a cause of premature mortality.
Cardiovascular disease, diabetes, arthritis and cancer are examples of chronic diseases that have gained particular public health priority in developed countries [1].
The Marseille-Rome consensus of 1988 classified pancreatitis as either acute or chronic, thereby eliminating the previously used, but somewhat confusing categories of acute relapsing and chronic relapsing [4]. Acute pancreatitis (AP) is due to acute inflammation of the exocrine pancreas due to the inappropriate intraparenchymal activation of digestive enzymes [5]. The principal aetiological factors in most demographic settings are gallstones and alcohol [6]. In clinical terms, it is characterised by a rapid onset of typical epigastric pain in conjunction with elevated serum lipase and/or consistent appearances on medical imaging [7]. Chronic pancreatitis (CP), by contrast, involves a chronic inflammatory process with a variable but progressive course of fibrosis and loss of parenchyma [5]. The basic pathogenetic mechanism is considered to be the cumulative effect of successive acute insults, or the so-called necrosis-fibrosis sequence, on a background of oxidative stress [8]. In the Western world, the principal causative factor is alcohol [5], although various other effect modifiers such as smoking [9,10], diet [11,12] and genetic predisposition [13-15] are thought to play a part in its multifactorial aetiology. Clinical manifestations of chronic pancreatitis, which are variable in extent and time-course, are pain, malabsorption and diabetes. Chronic pancreatitis is also associated with an increased risk of pancreatic cancer [16,17]. Diagnosis is a typically composite one, based on clinical history, morphologic abnormalities and functional impairment of exocrine and endocrine function [18]. From the preceding description, chronic pancreatitis per se would have most if not all of the characteristics of chronic disease as outlined by the NHPAC [3]. In addition, by virtue of the proposed necrosis-fibrosis hypothesis, acute pancreatitis can also be seen as at least a pathogenetic pathway to chronic pancreatitis in many cases. Indeed some authors consider even a first documented attack of alcohol-related acute pancreatitis to be a manifestation of a chronically diseased pancreas [19].
While Marseille-Rome’s dichotomous classification of pancreatitis represents a biologically cogent argument, when taken within the everyday clinical context it is often left wanting. Dissatisfaction can be evidenced in the use of the term “acute-on-chronic pancreatitis”, which is often accepted in colloquial clinical parlance and occasionally in published literature [20,21]. According to the International Classification of Diseases Version 10 (ICD-10) [22], the frequently observed phenomenon of an episode of acute pancreatitis occurring in a patient with underlying chronic pancreatitis could be classified as K85 (“acute pancreatitis”) but without a specific sub-classification to privilege the underlying chronic disease process; alternatively, it could be included under K86.1 (“other chronic pancreatitis”), which has provision for “recurrent” or “relapsing” chronic pancreatitis, although it is typically not the manifestations of chronic pancreatitis per se that are occurring at periodic intervals.
In essence, a considerable proportion of acute pancreatitis cases could also be considered in a broader therapeutic context as part of a chronic disease process, and thus amenable to more appropriate management strategies.
The clinic-pathological characteristics of pancreatitis in Far North Queensland
A prospective cohort study of incident cases in Cairns Base Hospital, the principal referral hospital for the region of Far North Queensland (FNQ), Australia was undertaken from March 2004 to July 2007. Cases were recruited if they fulfilled the diagnostic criteria for acute pancreatitis, namely acute onset of epigastric pain with an associated elevation in serum lipase [7].
At admission, data were collected from medical records and by facilitated questionnaire on a variety of potential explanatory variables including age, sex, indigenous status, aetiological attribution, alcohol, smoking, and diet. Outcome variables were length of hospital stay, actual severity as per the Atlanta criteria [23], and clinical, functional or morphological features consistent with chronic pancreatitis. For the latter, a diagnosis of underlying chronic pancreatitis was considered if one or more of the following were present: more than two previous (or subsequent) admissions for acute pancreatitis, chronic otherwise unexplained epigastric pain, steatorrhoea, otherwise unexplained weight loss. In addition, elastase-1 concentration ([FE-1]) was measured on the first available stool specimen following admission. Based on a previous efficacy study [24], a patient was considered to have pre-existing exocrine insufficiency if [FE-1] was less than 200 µg/g and they were predicted not to have severe acute pancreatitis with a Ranson score of less than 3.
Data analysis was performed using Stata™ version 9.0 (StataCorp, Texas, USA). Descriptive data were presented as absolute counts, means or medians, and proportions. Where applicable, standard univariate tests of comparison and multiple logistic regression were employed. Additional inferences were drawn from the data using capturerecapture [25] and principal components analysis (PCA) [26]. Only complete datasets were considered for analysis.
Supporting literature was sought using PubMed, entering terms such as “chronic pancreatitis”, “severe acute pancreatitis”, “endocrine insufficiency”, and “exocrine insufficiency”. Representative articles were reviewed, and included for discussion if relevant.
Ethical approval for the study as a whole was granted by the Human Research Ethics Committees of the Cairns Health Service District and James Cook University.
Reasons why acute pancreatitis may be considered a chronic disease
Over the 3.5-years study period, 153 cases were recruited for prospective data collection. By definition, all were of acute pancreatitis. Baseline characteristics are shown in Table 1.
| Total cases (n) | 153 |
| Mean age (years) | 44.7 |
| Males (n) | 94 (61.4%) |
| Indigenous Australians (n) | 63 (41.2%) |
| Alcohol aetiology (n) | 83 (56.9%) |
| Gallstone aetiology (n) | 36 (24.7%) |
| Other/unknown aetiology (n) | 27 (18.5%) |
| Median length of hospital stay (days) | 5 |
Table 1: Demographic and aetiological characteristics of documented acute pancreatitis cases admitted to Cairns Base Hospital, 2004-2007.
An additional 134 admissions for acute pancreatitis, that did not consent for prospective data collection or were missed by the recruitment process, were recorded by the hospital’s medical records department. To ascertain the true admission rate for this period, the preceding two data sources were considered along with a third source from the receipt of diagnosis-specific pathology specimens. For the census period, there were 304 admissions after merging of data sources, giving a crude admission rate of 7.6 per month. Crude ascertainment rates for discharge records and prospective identification were 44% and 52% respectively. Following capture-recapture analysis using log-linear modelling, total admissions more than doubled to 644 (95% CI: 449- 1100). The adjusted admission rate was therefore 16.1 per month (95% CI: 11.1-28.1) [27].
On further analysis of the prospectively obtained dataset (n=153), it became evident that there were at least three reasons for a significant proportion of these acute admissions to be worthy of a dedicated chronic disease management model.
A considerable proportion of acute pancreatitis cases harbour underlying chronic pancreatitis
Table 2 shows the numbers and proportions of cases exhibiting the various recognised clinical, biochemical and morphological features of chronic pancreatitis. If applying a composite diagnostic criterion of having at least one of these features present, the 54.3% of these acute cases would be diagnosed with underlying chronic pancreatitis. It should also be noted that certain data regarding diagnostic features were missing due to not being actively documented in the patient’s records or non-availability of biological specimens such as a stool sample for [FE-1] estimation. The proportion of patients with underlying chronic pancreatitis may thus be even greater than that described. Absolute numbers would also likely have been considerably greater if extrapolating from the capture-recapture analysis, which would augment the overall chronic disease burden.
| Percentage | Denominator (n) | |
|---|---|---|
| 2 or more previous admissions | 29.0% | 153 |
| Chronic abdominal pain | 31.8% | 153 |
| Steatorrhoea | 14.5% | 153 |
| Otherwise unexplained weight loss | 22.4% | 153 |
| [FE-1] <200 μg/g* | 53.7% | 67 |
| Chronic pancreatitis (by composite criteria) | 54.3% | 153 |
*only in cases with predicted mild acute pancreatitis (Ranson score<3)
Table 2: Features of chronic pancreatitis in acute admissions to Cairns Base Hospital, 2004-2007.
An attack of severe acute pancreatitis may lead to long-term structural or functional impairment
While typically representing only approximately 10% of all acute cases, SAP has been reported to have a case fatality of up to 10-15% [28] and significantly greater health resource consumption [29]. Further, the clinical criterion by which SAP has been diagnosed may determine the likelihood of long-term deficits. Anatomical lesions such as necrosis or pseudocysts are more likely to lead to loss of endocrine or exocrine capacity, compared to purely physiological derangements or transient organ failure.
In the FNQ series, 11.2% (n=17) of cases developed severe acute pancreatitis, as defined by the Atlanta criteria [23], subsequent to their initial presentation. Although details of the actual lesions that contributed to the SAP diagnosis were not included in the final summary data, the potential contribution of SAP to ongoing impairment can be exemplified by initial and follow-up CT scan images from a representative case of SAP (Figures 1 and 2).
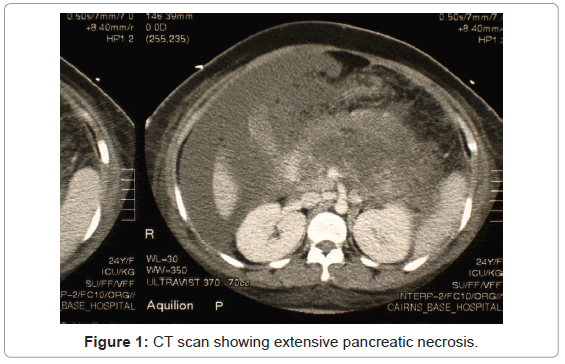
Figure 1: CT scan showing extensive pancreatic necrosis.
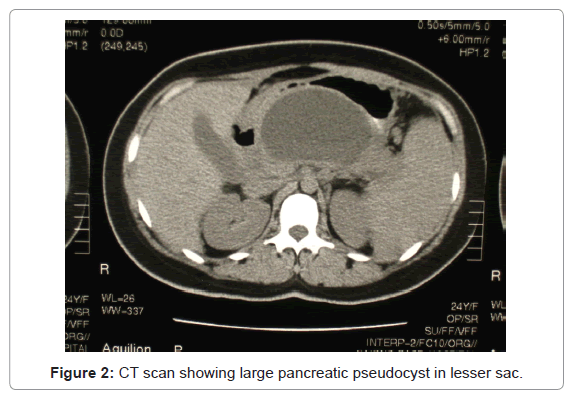
Figure 2: CT scan showing large pancreatic pseudocyst in lesser sac.
Beyond the FNQ series, the chronic sequelae of SAP have been the subject of numerous studies, although the results have been somewhat variable. This may be due to the rarity of the outcome in any particular cohort of incident cases, as well as variable follow-up periods. For example, in a retrospective cohort study of 88 patients who had undergone necrosectomy, Connor et al. [30] found that 25% of surviving patients developed exocrine insufficiency and 33% without prior diabetes developed endocrine insufficiency. By contrast, Ibars et al. [31] in a prospective cohort study of 63 acute biliary pancreatitis patients found no significant difference in endocrine or exocrine function between mild and severe cases. Andersson et al. [29] concluded that there was a higher prevalence of endocrine insufficiency after SAP although quality of life and exocrine function were no different. In summary, it would appear that on a case-by-case basis there should at least be vigilance for long-term complications following an attack of SAP.
Following an attack of acute pancreatitis, risk factors or precursors of chronic pancreatitis or recurrent acute pancreatitis may persist
Of the FNQ cohort, the median 7-days alcohol recall was 4.5 standard drinks. This tended to be skewed downwards by the cases of gallstone-related pancreatitis. However 33% (n=51) of cases admitted to drinking in excess of three standard drinks per day. Moreover, in 56.9% (n=83) of cases, the aetiology of the acute attack was attributed to alcohol. Mean daily cigarette consumption was 12.7, with 62.3% (n=94) of the cohort being current smokers.
It has been suggested that progression to chronic pancreatitis may be accelerated by a diet poor in anti-oxidants, which would otherwise serve to quench the oxidative stress of repeated clinical or sub-clinical acute attacks. While long-term dietary data was not available for the FNQ cohort, self-reported nutrient and other intakes were recorded for the 24-hour period prior to onset of acute symptoms. After adjustment for key demographic variables, no individual nutrient or other substance showed a significant association with underlying chronic pancreatitis. However, following principal components analysis (PCA), there emerged a significant positive association with a so-called “stimulant” pattern (with positive loadings on non-nutritive substances such as coffee and tobacco) and a negative association with a “nutritive” pattern (with positive loadings on major macro- and micro-nutrient groups) [32]. This is likely to be indicative of a pattern of binge behaviour in those with recurrent acute episodes related to alcohol. As such, this could inform a behavioural and nutritional management intervention forming part of a chronic disease management program.
Further examination of the cohort data revealed that 54.6% (n=83) of patients had a history of at least one other co-morbidity such as diabetes. This further validates the placement of this patient population within a chronic disease paradigm.
Towards a coherent chronic disease management strategy for pancreatitis
While the data presented from the FNQ study are representative of a particular local demographic, inferences drawn may nevertheless be generalizable to other parts of Australia and the world, in that similar risk factors for chronicity prevail and a reasonably constant proportion of patients typically develop severe complications during the course of an admission. In general, the incidence of acute pancreatitis is increasing in the Western world, largely due to the upward trend in prevalence of aetiological factors such as alcohol consumption and gallstone disease [6,33]. The consequent increase in chronic disease burden represents an even greater public health impost, and thus merits a coherent management strategy.
In a review of hospital admissions for pancreatitis to a regional hospital in Alice Springs, Australia, Ah-Tye [34] found a significant over-representation of Indigenous patients with a preponderance of cases attributable to alcohol misuse. There was also a high readmission rate. A population-based study from a region of northern Germany showed that a third of first attacks of acute pancreatitis were alcohol-related [35], for which a chronic disease management protocol could ostensibly be invoked. The proportion of alcohol-related cases remained reasonably constant over time for this population, although the proportion of cases with necrosis or other severe complications appeared to decrease slightly [36]. In one hospital-based study from the United Kingdom, 10% of 5312 people admitted for acute pancreatitis over a 35-year period had more than one recorded episode [37]. This was probably an underestimate of recurrence in that re-admissions within 12 months were not counted. In a 10-year retrospective case series of acute pancreatitis admissions in a Swedish hospital, Appelros and Borgström [38] found that 38% of admissions were in fact recurrent episodes, and that alcohol was the predominant aetiological factor for these, once again suggesting the need for a differential management pathway. These authors subsequently noted from the same series of patients a high incidence of long-term exocrine and endocrine dysfunction in those who had an episode of severe acute pancreatitis [39]. A review of hospital admissions in Ireland for acute pancreatitis between 1994 and 2004 showed an increasing incidence that was largely attributable to heavier alcohol consumption and binge drinking. This also appeared to be occurring at a younger age [33]. Even in Saudi Arabia where alcohol is a negligible aetiological factor, almost one-third of first attacks progressed to severe acute pancreatitis with ongoing morbidity such as diabetes [40].
The chronic disease paradigm was foreshadowed by the medical philosopher Georges Canguilhem, whose work on “le normal et le pathologique” [41] basically defined health as the ability to adapt to one’s environment. He also coined a maxim that no cure could guarantee a return to biological innocence. It therefore follows that (chronic) disease management involves treatment of the ongoing effects of the disease, as well as minimisation of risk factors to avert further attacks or progression. As described by Wagner et al. [42], the basic principles of chronic disease management include: the use of evidencebased, planned care; reorganization of practice systems and provider roles; improved patient self-management support; increased access to expertise; and greater availability of clinical information. Andrews [43] provided a cogent argument for the application of these to depression. However some adaptation may be needed to apply them to the diverse clinical scenarios presented by pancreatitis. The NHPAC [3] perhaps provides a more succinct and adaptable format through the four basic action areas it proposes: prevention across the continuum; early detection and early treatment; integration and continuity of prevention and care; and self-management.
Prevention across the continuum
Pancreatitis, like any chronic disease, lends itself well to a disease prevention framework based on the established ordinal hierarchy of prevention. Primary prevention involves undertaking certain practices in order to avoid the onset of the disease [44]. In the case of pancreatitis, education on lifestyle factors such as moderation of alcohol intake and cessation of smoking, at a population level, would ostensibly lead to a diminution in the incidence of acute pancreatitis episodes and eventual progression to chronic pancreatitis or long-term sequelae arising from severe acute pancreatitis in certain cases. Secondary prevention is defined as the prevention of recurrences or exacerbations of a disease or complications of its therapy [44]. Thus patients who present with a first attack of acute pancreatitis may be offered counselling to cease alcohol or tobacco intake, in order to prevent further attacks that would lead to a chronic disease state. In the same vein, consensus practice guidelines advocate expeditious cholecystectomy for gallstone-related cases [45]. Tertiary prevention aims at providing appropriate supportive and rehabilitative services to minimise morbidity and maximise quality of life when a chronic disease state is clearly present [44]. Such measures would suitably be applied to cases of established chronic pancreatitis, many of whom interface with the hospital system by virtue of their recurrent acute attacks. Strategies would aim to optimise pain control, nutrient absorption and glycaemic control. Where available, practice guidelines may help inform management, such as those of the Australasian Pancreatic Club for exocrine insufficiency [46]. Moreover, a focus on quality of life measures and psychological management has also been recommended for these patients [47]. A fourth tier of prevention, quaternary prevention, basically refers to the avoidance of over-medicalization where interventions may be of limited utility or overtly unethical [48]. This may apply to cases of chronic pancreatitis that would not be amenable to invasive surgical or endoscopic procedures due to anatomical considerations or the persistence of correctable risk factors that would negate the benefits of such treatments. In cases of severe acute pancreatitis, it is generally advised to reserve surgical debridement of necrosis for cases with proven superinfection, in order minimise eventual functional deficits [49,50]. Also, despite the usual recommendations, early cholecystectomy is not advisable for severe acute gallstone-related pancreatitis; [51-53] it should be delayed until the acute inflammatory response has settled.
Based on the work of Gordon [54] and Kumpfer and Baxley [55], there is an alternative three-tiered classification of preventive strategies, which can also be suitably applied to pancreatitis. Universal prevention involves the whole population at risk from known aetiological factors. In the case of pancreatitis, such interventions may comprise public health promotion campaigns advocating moderation in alcohol consumption and balanced nutritional intake. Selective prevention is where specific at-risk groups may be targeted based on recognised demographic or other characteristics. From the FNQ cohort described, it would thus be reasonable to develop strategies directed at the Indigenous community or even men in general. Indicated prevention is defined as a screening process that aims to identify individuals with early, potentially remediable disease or those exhibiting high-risk behaviours. Specific primary, secondary or tertiary interventions would then be prescribed. Such a strategy could conceivably be applied to any patient admitted for the first time with acute alcohol-related pancreatitis. Further, those with clinical, morphological or biochemical evidence of chronic pancreatitis detected on acute admission could be offered an education and followup program. Indicated prevention is also implicit in the numerous guidelines that advocate early cholecystectomy following an attack of gallstone-related pancreatitis [45,49,50].
Early detection and early treatment
Another cornerstone of chronic disease management is early detection facilitating early treatment. Diagnosing chronic pancreatitis in those presenting acutely or, more broadly, those acute cases that would benefit from a chronic disease management model, is the key imperative. Early diagnosis of chronic pancreatitis per se (prior to onset of constant pain, malabsorption or diabetes) remains somewhat challenging, particularly if relying solely on a morphological or functional investigation to confirm the disease process. Furthermore, to detect underlying chronic pancreatitis in such a manner, opportunistically during the course of an acute admission, poses additional logistic difficulties. Faecal elastase-1 concentration ([FE-1]) is simple and non-invasive test that has been shown to have excellent sensitivity and specificity for cases outside the acute setting [56]. It has also been shown to have good diagnostic performance for detecting incipient chronic pancreatitis in non-severe acute cases [24]. However, obtaining a stool specimen from a patient in the course of a brief acute hospital admission may be logistically difficult. From a pragmatic point of view, it may simply suffice to assume that patients who have had more than one acute attack and/or without abatement of risk factors such as alcohol abuse, effectively have chronic pancreatitis and should be offered a comprehensive management program.
Integration and continuity of prevention and care
Regarding an integrated and continuous program of care recommended for chronic disease, acute pancreatitis is traditionally managed in surgical units, unless Intensive Care is required for supervening severe complications. The reasons for this would seem to stem from the well-established need for prompt cholecystectomy in cases of acute biliary pancreatitis, and for surgical debridement (necrosectomy) in the relatively uncommon eventuality of infected necrotic pancreatitis [45,57]. The predominant therapeutic paradigm of Surgery relates to an acute episode of care with the ostensible outcome of “cure” or at least of definitive abatement of prevailing symptoms, in contrast to a chronic disease paradigm, which involves repeated episodes of care with the ultimate objective being disease attenuation rather than complete resolution. Even in cases of acute pancreatitis that do not require operative intervention, it is assumed that the disease process and/or its causative factors cease when the patient is discharged. Certainly later complications ensuing from the acute episode, such as pseudocyst and pancreatic fistula, may necessitate surgical interventions. Moreover, based on the evidence from the FNQ cohort, it would appear that a more consciously multidisciplinary approach, calling upon disciplines other than Surgery, is warranted for many of the cases that present in the acute context. For example, gastroenterological and dietetic support is required for cases of exocrine insufficiency, where prescribed treatments may include enzyme supplementation, gastric acid suppression, medium-chain triglycerides and other nutritional advice [46]. Many cases of AP, even those without severe manifestations, may have transient or permanent exocrine or endocrine deficiencies that would warrant some form of replacement therapy. In a small prospective cohort study from the United Kingdom, Boreham and Ammori [58] demonstrated that acute pancreatitis cases with necrosis were likely to have residual exocrine insufficiency and that this also correlated with endocrine insufficiency. Psychological and rehabilitative input is recommended where substance abuse remains an issue and chronic pain management where pain persists beyond the acute episode. As well as pharmacotherapy, the latter may entail radiologically or endoscopically guided ablative techniques. Furthermore, dedicated follow-up of presumed chronic cases is required to detect any deterioration in function that could be corrected or attenuated by a specific intervention. However this may be somewhat difficult in the case of entrenched chronic pancreatitis cases where alcohol abuse and other lifestyle factors mitigate against compliance.
Self-management
The remaining “action area” for chronic disease according to the NHPAC is self-management. This has always been seen as a challenge for pancreatitis, typically because of the lifestyle factors associated with the aetiology of those cases exhibiting chronic disease characteristics. Nevertheless, active acknowledgement by clinicians and patients of the “teachable moment” may serve as the initiating point for the patient in taking responsibility for their own care [59]. Teachable moments are basically describe naturally occurring health events thought to motivate individuals to adopt risk-reducing behaviours [60]. As with key events that may be exploited to promote smoking cessation [60], an admission for acute pancreatitis could provide a trigger to increase patients’ awareness of the role of alcohol, smoking and diet in the progression to chronicity. Engagement in an active follow-up process could also be actively encouraged for those with evidence of underlying chronic pancreatitis or those who had an episode of severe acute pancreatitis.
Managing pancreatitis as a chronic disease
The FNQ cohort, supported by a growing body of literature, provides a case for considering incident pancreatitis cases, by default, from within a chronic disease framework. This represents a paradigm shift from the traditional acute “surgical” model of care.
Based on the principles of chronic disease management as outlined above, a feasible, generalizable and multimodal algorithm for incident cases of acute pancreatitis is suggested in Figure 3. Such a model of care should be embedded within a more holistic chronic disease framework, given the prevalence of co-morbidities within this patient population.
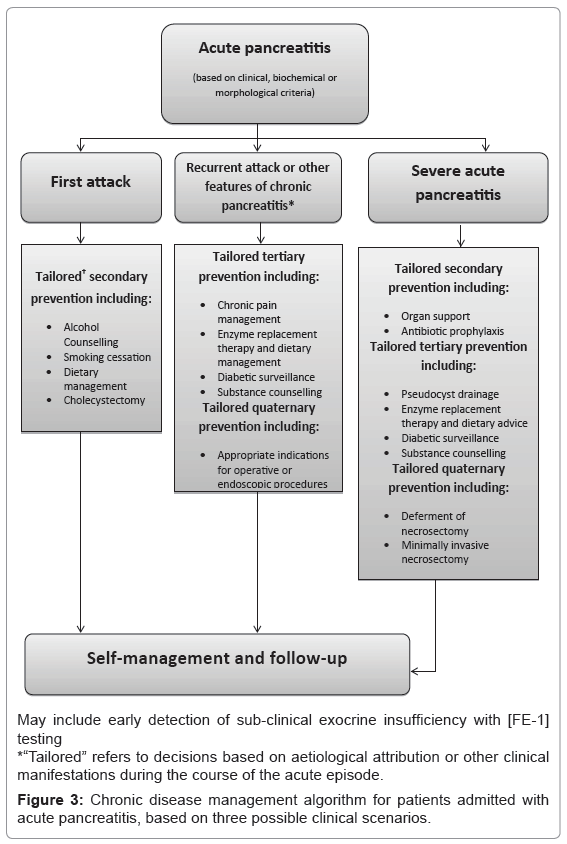
Figure 3: Chronic disease management algorithm for patients admitted with acute pancreatitis, based on three possible clinical scenarios.