Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 1
Background: Sleep Apnea Syndrome is common and underdiagnosed in the hospitalized patient population. Protocols for evaluation of sleep apnea in the inpatient setting are not standardized.
Study question: Does requiring a sleep and breathing consultation when requesting a type 3 portable monitor to evaluate for sleep apnea syndrome in the inpatient setting lead to better follow up and continuous positive airway pressure device (CPAP) use than open access to this testing.
Methods: Retrospective chart review of patients who underwent a type 3 portable sleep study between 2008 to 2010 from a tertiary care, academic medical center. Midway through the period of review the process of ordering was changed to include mandatory pulmonary consultation. 105 patient records were analyzed for outcomes including diagnosis and ongoing care for sleep disordered breathing.
Results: The number of studies adequate for interpretation was not impacted by addition of a mandatory consult (87% vs. 92%), nor was the number of positive studies with an AHI >5 (80% vs. 73%). Follow up after undergoing a diagnostic type 3 study was significantly higher in the post intervention group (51% vs. 76%, P=0.04). Medical follow up as outpatient and CPAP initiation for those with a positive study was also significantly higher with the consultation requirement (55% vs. 84%, P=0.024).
Conclusion: In the hospitalized setting, a type 3 portable monitor for evaluation of sleep apnea when paired with a consultation from a sleep/pulmonary specialist can significant improve the likelihood outpatient follow up and improved likelihood of ongoing adherence for those who are initiated on CPAP. Large controlled multicenter studies are needed to determine if a protocol for identifying at risk hospitalized patients coupling type 3 testing with an experienced consultant in the evaluation of sleep disordered breathing translates to improved value based care.
Keywords: Type 3 portal monitor; Continuous positive airway pressure; CPAP adherence; Sleep apnea
Undiagnosed sleep apnea is common in hospitalized patients. The National Hospital Discharge Survey from 2004 registered that only 5.8% of inpatients diagnosed with sleep apnea were provided with CPAP therapy during hospitalization [1].
As far back as 1998, sleep researchers detected an increase in healthcare utilization in cardiac patients who had untreated OSA [2]. Sleep disordered breathing in general remains a significant co-morbidity that factors into readmissions. In a recent observation cohort study Central Sleep Apnea (CSA) was an independent risk factor for 6 months' cardiac readmissions and the effect size exceeded that of all known predictors of heart failure readmissions. In this same study, severe OSA was also an independent predictor of readmissions with an adjusted rate ratio of 1.49 (P=0.04) [3].
Two 2008 population-based studies, one from the United States, [4] and one from Australia, [5] also showed increased all-cause mortality in subjects with moderate-to severe OSA. The adjusted hazard ratios in both studies ranged from 3.0-6.2 for subjects with moderate-to-severe disease compared with no disease.
Cost to Benefit analyses support that the treatment of sleep apnea reduces the total cost of care through better control of comorbidities resulting in decreased health care utilization including readmissions and improvement in co-morbid conditions such as obstructive lung disease and congestive heart failure [6].
Current guidelines recommend overnight polysomnography in a monitored setting (type 1 PSG) for the diagnosis of OSA [4,7-9]. Home-based diagnosis and therapy for OSA with limited monitoring channels designed to detect sleep apnea primarily has provide an alternative to the type 1 PSG and improves access for patient care. In carefully selected patients (generally those with a high pretest probability of disease and without comorbidities), a home-based approach using the type 3 portable monitor (minimum requirement:one oximetry channel, one airflow channel, one effort belt channel) had similar clinical outcomes to those patients studied in the laboratory [10,11].
According to current American academy of Sleep Medicine (AASM) clinical guidelines, type 3 portable monitoring (PM) is not appropriate for OSA diagnosis when dealing with inpatients who have significant comorbid conditions that may degrade the accuracy of PM, including but not limited to, moderate to severe pulmonary disease, neuromuscular disease, or CHF. However, they go on to state the PM may be indicated for OSA diagnosis if a Type 1 PSG cannot be done due to immobility, age, or critical illness [12].
Many patients cared for in the inpatient setting have co-morbid sleep apnea. A significant proportion is undiagnosed at the time of the hospital stay. For those with a substantial co-morbid condition such as heart failure or obstructive lung disease where the co-existing untreated sleep apnea increases the likelihood of morbidity and mortality, rapid diagnosis and initiation of therapy is appealing. Factors such as decompensated heart failure, narcotics, sepsis and delirium states that result in poor sleep/little sleep need to be weighed again the risks of discharging a patient with underlying sleep disordered breathing that ultimately contributes to costs of care and may result in readmission for the same or related condition before an outpatient evaluation of the sleep disordered breathing can be completed. Inpatient evaluation of sleep disordered breathing at this time is limited to non-validated methods as the type 1 PSG is in general not widely accessible for inpatient testing. While the type 3 PM can be an effective diagnostic tool patient factors that can result in over diagnosis and under diagnosis of sleep disordered breathing need to also be considered in the inpatient setting. The appropriateness of testing and the timing of the testing require knowledge of these factors and experienced clinicians are a necessary component of any inpatient screening program.
Inpatient diagnosis of obstructive sleep apnea (OSA) may improve our ability to expedite the initiation of continuous positive airway pressure (CPAP) treatment for the more frail patients with sleep disordered breathing when a laboratory based PSG is not practical.
Prior to June 30, 2009 our academic practice offered inpatient testing using the type 3 portable monitor to evaluate for sleep apnea at the treating physician’s request. Physicians were given general guidelines that the patient should be as close to discharge as possible to allow for any acute medical issues to have the least impact on the test results and that the patient could not be on more than 4 liters of oxygen as that had led to less reliable airflow signal. Results were reported to the requesting physician and documented in the patient chart. Coordinating any follow up and initiation of PAP therapy was the responsibility of the discharging physician. In reviewing standards for care across the practice, it was noted by primary care physicians that many of these patients who had undergone inpatient testing were not aware of the test results nor were they given specific instructions regarding the results or need for follow up. This raised concerns that the open access model did not provide patients with adequate communication on results or guarantee outpatient treatment or follow up. As a result we added a mandatory pulmonary consult to the the request for the inpatient type 3 portable monitor testing in hopes that it would improve patient follow up upon discharge. In this quality improvement process, we evaluated retrospectively whether the outcomes for outpatient follow up and adherence improved when testing was directed by experienced clinicians.
This was a practice quality improvement project. Retrospective chart review was done for those patients undergoing type 3 portable sleep studies from 2008 to 2010 in our tertiary care, academic medical center. Beginning July 1, 2009 a mandatory pulmonary consultation was added to the requirements for sleep testing for hospitalized patients. The patient outcomes were evaluated comparing those before and after this added requirement.
Inclusion criteria as follows: 1) age ≥ 18 years, 2) inpatient generated request for portable monitoring for evaluation of sleep apnea, 3) Type 3 PM testing completed during the time period of July 2008 to December 2010. The outcomes assessed were the proportion of ordered studies usable for analysis of sleep apnea, (AHI>5), proportion of patients tested that had follow up after discharge, and proportion that had ongoing PAP therapy after discharge.
A Type 3 PM device (Somnostar Orbit) with 4 channels including nasal flow, chest and abdominal movement belts and oximetry channels was used for all the patients [13]. A minimum of 4 hour of recording was required for a usable test. The studies were scored a trained respiratory therapist and reviewed and edited by a board certified sleep specialist. The scoring following the American Academy of Sleep Medicine 2007 scoring requirements. Criteria for failed testing were less than 4 hours recording time or lost signal channels preventing interpretation. Failed testing did not eliminate the subject from analysis for endpoints. Subgroup analysis for obstructive versus central apnea was not done due to the nature of the type 3 monitor’s design and intended purpose specific to screening for obstructive sleep apnea only. The criteria for initiating PAP therapy was at the discretion of the physician who ordered the type 3 portable monitor test and included consideration for co-morbid cardiovascular disease, hypersomnia or sleep dysfunction in the context of an AHI of at least 5 or more events per hour.
At the time of the quality assessment, patients were interviewed when possible via telephone at the time of the chart review to report on their status of medical follow up after discharge regarding the suspected sleep apnea. They were also asked if they were currently using PAP therapy. Medical follow up for the sleep apnea was defined as the presence of an adherence download in the medical record, a Type 1 PSG completed as an outpatient after the inpatient evaluation, or an outpatient follow up visit for which the sleep apnea as a problem addressed during the visit. The outpatient chart audit for follow up documentation included specialists (either sleep or pulmonary) and the primary care physician. Data was analyzed using STATA software for Windows OS. Analysis was carried out using Fishers Exact test. The P-value of <0.05 were considered as statistically significant.
A total 105 patients underwent testing during the period of chart review. Fifty six patients underwent inpatient PM testing prior to the requirement of pulmonary consultation and 49 underwent evaluation after the intervention (Table 1).
| Follow up with positive(POS) study | PAP Follow up with usable study (POS+NEG) | Follow overall All tested | |
|---|---|---|---|
| PRE intervention | 17/ 31 | 18/35 | 21/56 |
| POST intervention | 21/25 | 25/33 | 28/49 |
| Fishers exact test | P=0.02 | P=0.04 | P=0.05 |
Table 1: Quality Initiative Outcomes. Follow up on results and PAP therapy initiation was significantly higher across all groups after the addition of the mandatory consultation (intervention) associated with ordering an inpatient type 3 PM to assess for sleep disordered breathing. A positive study (POS) was defined as at least 4 hours of study with an AHI >5. Those with AHI <5 were considered negative (NEG). Some tests were failure (unusable due to lead failure). Follow up was significantly improved in all categories after addition of the pulmonary consultation.
The number of usable studies was similiar comparing groups(pre intervention 87% vs. post intervention 92% usable, P=ns), as was the number of positive studies with an AHI >5 (pre intervention 80% vs. post intervention 73%, P=ns). The average recording time was 9.1 hours for those undergoing testing prior to the intervention of a mandatory consultation intervention and 7.75 hours for those after the intervention.
Documented outpatient medical follow up for the sleep apnea was significantly higher in the post intervention group (Pre intervention 51% vs. post intervention 75%, P=0.04). For those with a positive study, PAP initiation and ongoing use was significantly higher with the consultation requirement (pre intervention 55% vs. post intervention 84%, P=0.02).
Phone contact was not possible in 26 of the 56 (46%) pre-intervention patients with 13 of them having died prior to the start of the study. Phone contact was not possible in 20 of the 49 (40%) post intervention (P=ns) with 3 dead prior to the study. For those with whom we were able to discuss their current status, their reports of use of cpap were added to the medical follow up statistics when they were not being followed at our institution (Figure 1).
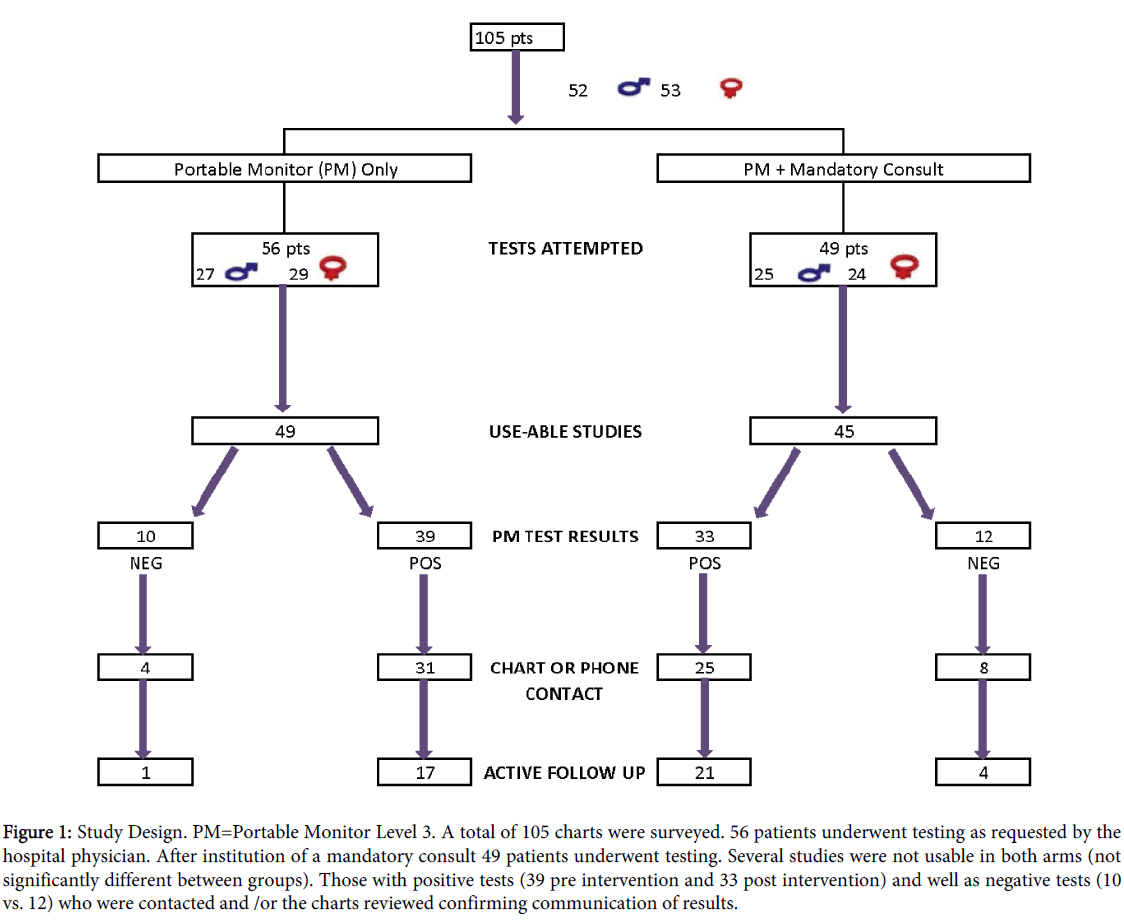
Figure 1: Study Design. PM=Portable Monitor Level 3. A total of 105 charts were surveyed. 56 patients underwent testing as requested by the hospital physician. After institution of a mandatory consult 49 patients underwent testing. Several studies were not usable in both arms (not significantly different between groups). Those with positive tests (39 pre intervention and 33 post intervention) and well as negative tests (10 vs. 12) who were contacted and /or the charts reviewed confirming communication of results.
As a practice improvement project, the addition of a mandatory pulmonary consultation linked to the Type 3 PM testing did lead to significant improvement in outpatient follow up and ongoing PAP therapy for all those seen in consultation based on the documentation in the patients’ medical records. The reason why adding the consultative requirement to the inpatient testing request improved the outpatient follow up and PAP adherence may in part be the result of ownership in communication and active management on the part of the consultants during and beyond the inpatient setting. Engaging in discussion with the patient throughout the process on the impact of sleep apnea on health reinforced through repeat bedside visits and outpatient office follow up visits may have decreased drop outs.
As a retrospective review, there were several weaknesses inherit in our study. The cohorts were fixed based on the time they underwent testing. The cohort without a mandated consultation was tested at an earlier time period. A prospective controlled study was not possible and same time comparison analysis could not be done due to insufficient numbers tested during the time prior the implementation of manadatory consultation for all requested inpatient studies. Public awareness of sleep apnea and treatment has steadily increased over time, so there is possibility of improved adherence in the group with the mandated consultation as a result of having been tested in an environment of better awareness of the value of treatment that the pre-intervention cohort.
Untreated sleep apnea is a common condition in hospitalized patients. Untreated sleep disordered breathing is considered a risk factor for readmission when coupled with co-morbid diseases. As more and more focus is brought on improving quality of care through reducing readmission rates, addressing sleep disordered breathing for hospitalized patients will become a necessary component of the inpatient practice of medicine. We have demonstrated that the Type 3 portable monitor coupled with involvement at the outset by the pulmonologist can result in improved likelihood for ongoing treatment for some patients. Consistent application of diagnostic and treatment protocols for the hospitalized patients will be necessary to realize the full savings in healthcare utilization costs associated with addressing sleep disordered breathing in the hospital setting.
A larger prospective controlled study of accelerated diagnostic and treatment clinical pathways for the hospitalized patient will be needed to explore the potential of subsequent health care savings associated with treatment of sleep disordered breathing.